Successful Left Trisectionectomy for Intrahepatic Cholangiocarcinoma in a Patient with a Right-Sided Round Ligament: A Case Report
Masashi Utsumi, Masaru Inagaki, Koji Kitada, Naoyuki Tokunaga, Koki Omoto, Naoki Onoda, Kosuke Yunoki, Hiroki Okabayashi, Ryosuke Hamano, Hideaki Miyaso, Yosuke Tsunemitsu, Shinya Otsuka, Rika Omote

TL;DR
A rare case of successful liver surgery for cholangiocarcinoma in a patient with a right-sided round ligament is reported, highlighting the importance of understanding anatomical anomalies.
Contribution
This case report presents a successful left trisectionectomy in a patient with a rare anatomical anomaly and intrahepatic cholangiocarcinoma.
Findings
A 3-D CT of the portal vein helped visualize the vascular anomalies associated with the right-sided round ligament.
Left trisectionectomy with extrahepatic bile-duct resection was successfully performed, and the patient showed no recurrence three months post-surgery.
Abstract
A right-sided round ligament (RSRL) is a rare congenital anomaly characterized by the umbilical vein being connected to the right paramedian trunk. As it is associated with intrahepatic vascular anomalies, it poses special difficulties in hepatic resection, and an accurate understanding of those anomalies is indispensable. An 80-year-old man visited a health clinic with the chief complaint of jaundice. Hyperbilirubinemia and impaired liver function were detected upon laboratory examination. Therefore, the patient was referred to our hospital for further examination and treatment. Contrast-enhanced computed tomography (CT) demonstrated dilatation of the intrahepatic bile ducts and the presence of a hypovascular tumor of 30 mm in size in the left lateral segment of the liver. The anterior branch of the portal vein (PV) formed a right-sided umbilical portion of the PV and was connected to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
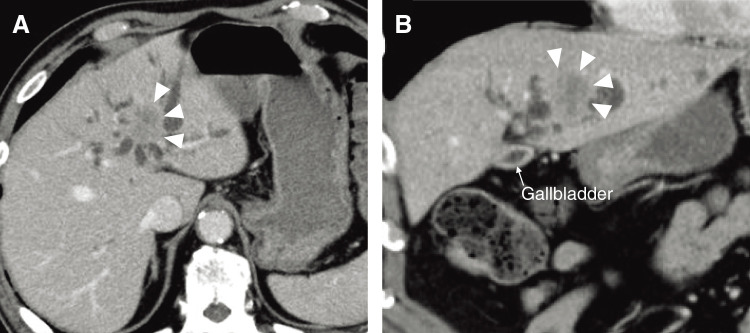 Fig. 1
Fig. 1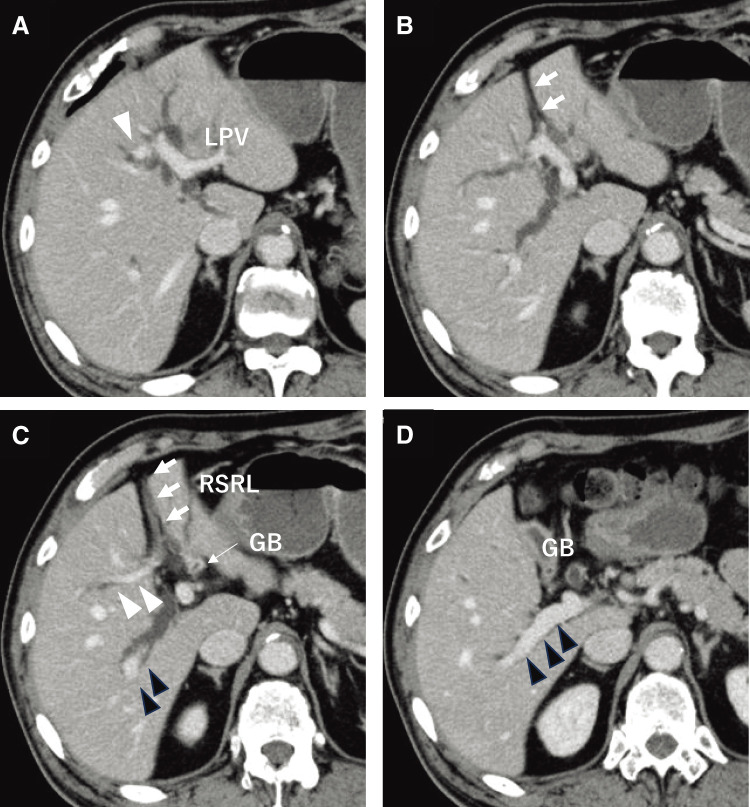 Fig. 2
Fig. 2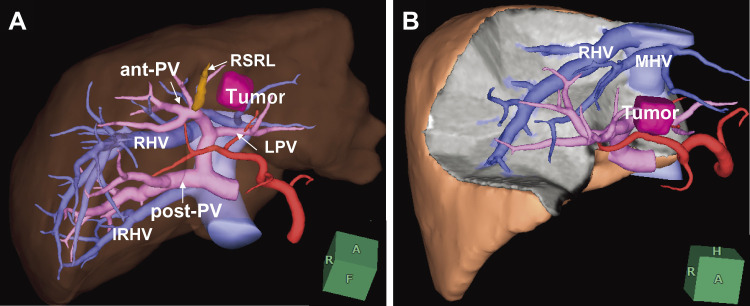 Fig. 3
Fig. 3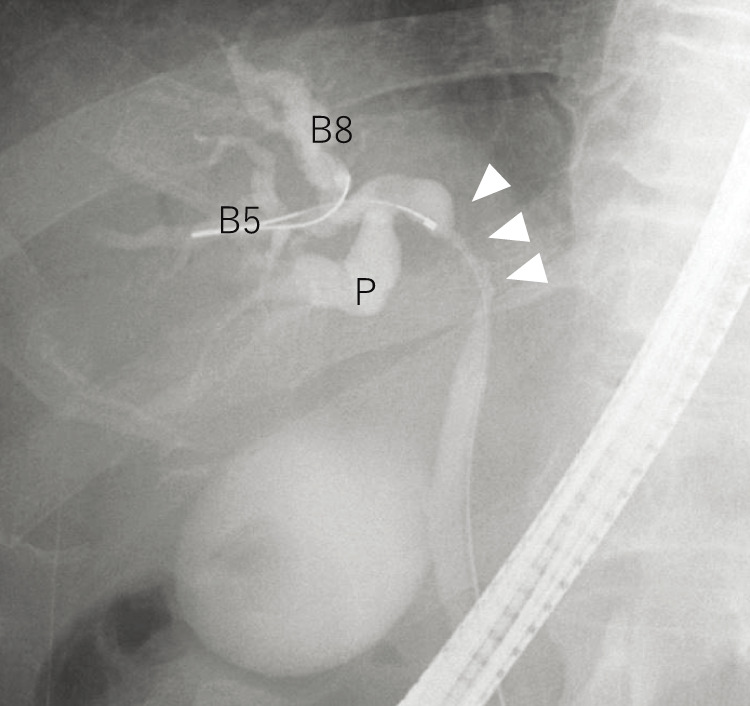 Fig. 4
Fig. 4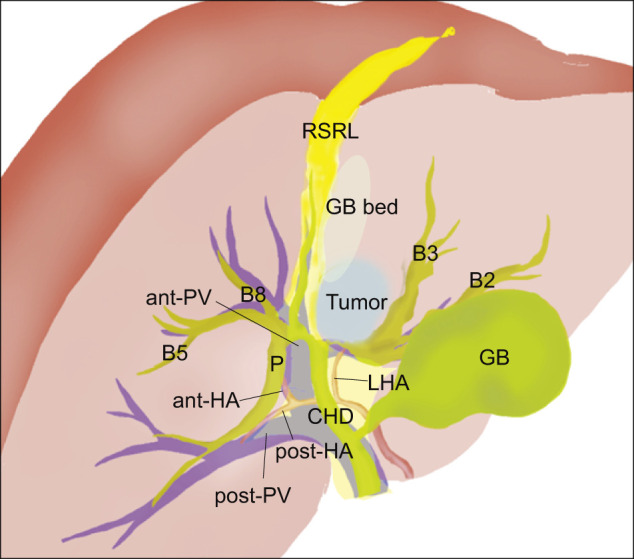 Fig. 5
Fig. 5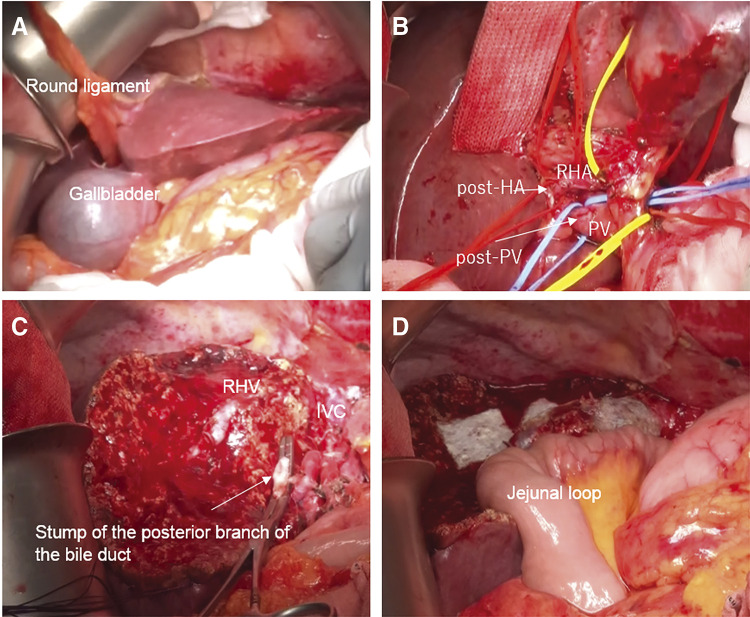 Fig. 6
Fig. 6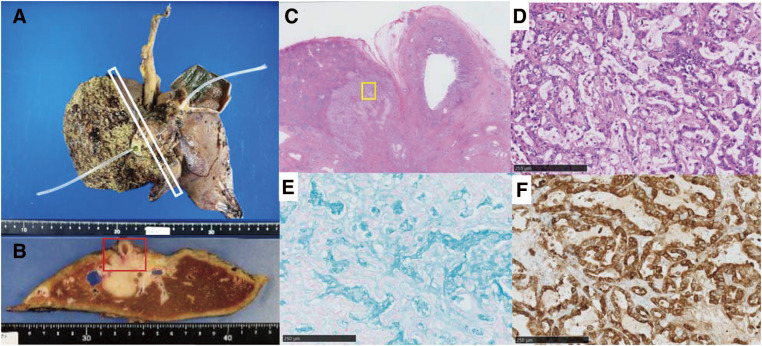 Fig. 7
Fig. 7| Author | Year | Sex | Disease | Operation | Portal anatomy | Biliary anatomy | Postoperative complication |
|---|---|---|---|---|---|---|---|
| Almodhaiberi et al. | 2015 | Male | CCC | Left hemihepatectomy | Ppost-i | Symmetrical type | None |
| Hai et al. | 2017 | Male | CCC | Extended left hemihepatectomy | Ppost-i | Total-left type | Bile leakage |
| Goto et al. | 2018 | Male | GBC | Right hemihepatectomy | Trifurcation | Independent right-lateral type | None |
| Terasaki et al. | 2019 | Male | CRLM | Lap-left lateral sectionectomy | Bifurcation | Symmetrical type | None |
| Ishida et al. | 2020 | Male | HCC | Partial hepatectomy | Ppost-i | NA | None |
| Ishida et al. | 2020 | Male | HCC | Partial hepatectomy | Ppost-i | NA | None |
| Ishida et al. | 2020 | Female | CRLM | Right hemihepatectomy | Bifurcation | NA | None |
| Ishida et al. | 2020 | Male | CCC | Left trisectionectomy | Ppost-i | Total-left type | None |
| Ishida et al. | 2020 | Male | HCC and CCC | Extended posterior sectionectomy | Bifurcation | Symmetrical type | None |
| Our previous case | 2022 | Female | GBC | Partial hepatectomy | Ppost-i | Symmetrical type | None |
| Our previous case | 2022 | Male | CRLM | Segmentectomy | Bifurcation | Total-left type | None |
| Our current case | 2024 | Male | ICC | Left trisectionectomy | Ppost-i | Total-left type | Abdominal abscess |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Biliary and Gastrointestinal Fistulas · Gallbladder and Bile Duct Disorders
Abbreviations
ant-PV anterior branch of the portal vein CT computed tomography PV portal vein post-PV posterior branch of the PV RSRL right-sided round ligament
INTRODUCTION
A right-sided round ligament (RSRL) is a rare congenital anomaly characterized by the connection of the umbilical vein to the right paramedian trunk, with a reported frequency of 0.1%–1.2%.^1,2)^ As it is associated with intrahepatic vascular anomalies, it causes special difficulties in hepatic resection, and an accurate understanding of those anomalies is indispensable. Here, we report a case of intrahepatic cholangiocarcinoma with an RSRL in which we performed left trisectionectomy.
CASE PRESENTATION
An 80-year-old man visited a health clinic with the chief complaint of jaundice. Hyperbilirubinemia and impaired liver function were detected upon laboratory examination. Therefore, the patient was referred to our hospital for further examination and treatment.
Laboratory examination revealed that the leukocyte and C-reactive protein levels were within the normal range but that serum levels of total bilirubin (9.3 mg/dL; normal range, 0.2–1.2 mg/dL), aspartate aminotransferase (111 U/L; normal range, 13–33 U/L), alanine aminotransferase (301 U/L; normal range, 8–42 U/L), alkaline phosphatase (232 U/L; normal range, 115–359 U/L), gamma-guanosine triphosphate (617 U/L; normal range, 11–58 U/L), carcinoembryonic antigen (17.8 ng/mL; normal range, 0–5 ng/mL), and carbohydrate antigen 19-9 (145.9 U/mL; normal range, 0–37 U/mL) were high. The indocyanine-green retention rate 15 min after injection was 7.3%. The patient’s Child–Pugh classification was class A. Test results for hepatitis B surface antigen and antibodies against hepatitis C virus were negative.
Contrast-enhanced computed tomography (CT) demonstrated dilatation of the intrahepatic bile ducts and the presence of a hypovascular tumor of 30 mm in size in the left lateral segment of the liver (Fig. 1). The posterior branch of the portal vein (post-PV) ramified independently from the main portal trunk (Ppost-i type), followed by ramification of the anterior branch of the PV (ant-PV) and the left PV (LPV) (Fig. 2). The ant-PV formed a right-sided umbilical portion of the PV and was connected to the round ligament (Fig. 2). The round ligament was located to the right of the gallbladder (Fig. 2). 3-D CT of the PV clearly illustrated the independent ramification of the posterior branch and the subsequent bifurcation of the ant-PV and LPV (Fig. 3). 3-D CT images were captured using a Synapse Vincent 3-dimensional volume analyzer (Fujifilm Holdings Corporation, Tokyo, Japan).
Contrast-enhanced computed tomographic images of the patient. (A) Axial section image. (B) Coronal section image. Dilatation of the intrahepatic bile ducts, a tumorous lesion, and a hypovascular tumor of 30 mm in size in the left lateral segment of the liver (arrowheads).
Contrast-enhanced computed tomographic images of the patient. The posterior branch of the PV (black arrowheads) is ramified independently (Ppost-i type, D), followed by the ramification of the anterior branch of the PV (white arrowheads) and the LPV (A–C). The ant-PV formed a right-sided umbilical portion of the PV and was connected to the round ligament (white arrows) (B, C). The RSRL (white arrows) was located to the right of the gallbladder (C, D).ant-PV, anterior branch of the portal vein; GB, gallbladder; LPV, left portal vein; PV, portal vein; RSRL, right-sided round ligament
3-D CT images of the patient. (A) The image clearly illustrates the independent ramification of the post-PV and the subsequent bifurcation of the ant-PV and LPV. (B) 3-D CT images were captured using a Synapse Vincent 3-D volume analyzer (Fujifilm Holdings Corporation, Tokyo, Japan).ant-PV, anterior branch of the portal vein; IRHV, inferior right hepatic vein; LPV, left portal vein; MHV, middle hepatic vein; post-PV, posterior branch of the portal vein; RSRL, right-sided round ligament; 3-D CT, 3-dimensional computed tomography
Endoscopic, nasogastric biliary drainage was performed to treat the patient for obstructive jaundice, and endoscopic retrograde cholangiopancreatography demonstrated severe stenosis of the hilar bile duct (Fig. 4). The stenotic portion extended from the hepatic hilum to the right, B2, and B3 bile ducts (Fig. 4). The preoperative schema of the perihilar anatomy and cancer progression is shown in Fig. 5. Biopsies of the stenotic bile ducts were suggestive of adenocarcinoma. The root of the posterior branch of the bile duct was not infiltrated by the cancer. According to CT volumetry, the volume of the posterior section of the liver was 610 mL (50.7% of the total liver volume). Positron emission tomography revealed focally increased glucose uptake in the tumor, suggesting malignancy. The preoperative diagnosis was intrahepatic cholangiocarcinoma (T4N0M0, stage III B).^3)^
Endoscopic cholangiopancreatography of the patient. Severe stenosis of hilar bile duct (arrowheads). The stenotic portion extended from the hepatic hilum to the right (the B2 and B3 bile ducts).P, posterior branch of hepatic bile duct
Preoperative schema of perihilar anatomy and cancer position.ant-HA, anterior branch of the hepatic artery; ant-PV, anterior branch of the portal vein; CHD, common hepatic duct; GB, gallbladder; LHA, left hepatic artery; P, posterior branch of the hepatic bile duct; post-HA, posterior branch of the hepatic artery; RSRL, right-sided round ligament
Operation
A left trisectionectomy with extrahepatic bile-duct resection and hepaticojejunostomy was performed (Fig. 6). The left, right anterior, and posterior arteries, the common hepatic duct, and the root of the LPV, ant-PV, post-PV were sequentially dissected and taped. After clamp testing to confirm inflow into the posterior lesion, the left and right anterior arteries and the root of the LPV and ant-PV were ligated and divided. Thereafter, the posterior branch of the bile duct was divided and taped. Hepatic parenchymal resection, guided by a demarcation line, was conducted along the right hepatic vein, and the common trunk of the middle and left hepatic vein was divided. Finally, the posterior branch of the bile duct was separated, and the specimen was removed. The result of the frozen section analysis of the bile-duct stump was negative for carcinoma (on both the duodenal and hepatic sides). Biliary reconstruction was performed using the Roux-en-Y method. The operation time was 7 h 30 min, and the intraoperative blood loss was 750 mL.
Operative observations. (A) The gallbladder is located to the left of the round ligament. (B) The hepatic hilum was dissected, and the vessels were wrapped with tape. (C) The dissected surface after left trisectionectomy. Liver resection was performed along the RHV. (D) Biliary reconstruction was performed using the Roux-en-Y method.IVC, inferior vena cava; post-HA, posterior branch of hepatic artery; post-PV, posterior branch of the portal vein; PV, portal vein; RHA, right hepatic artery; RHV, right hepatic vein
The histological diagnosis of the tumor was intrahepatic cholangiocarcinoma (large duct type, 5.5 × 4.5 cm) (Fig. 7). Metastasis was detected in 5/11 regional lymph nodes. The final pathological stage was T4N1M0, stage 3B, according to the 8th edition of the American Joint Committee on Cancer Staging System.^3)^ An intra-abdominal abscess developed after the operation. We treated the patient with drainage of the abscess cavity and with antibiotics, and he was discharged 25 days after surgery. He declined adjuvant chemotherapy. Three months after surgery, the patient was doing well without recurrence.
Histopathological examination. (A) Gross photograph of the resected specimen. (B) Cut surface in the white square of panel (A). It contained a solid whitish mass measuring 5.5 × 4.5 cm with irregular margins. (C) Hematoxylin and eosin staining of the area in the red square in panel (B). (D–F) The area in the yellow square in panel (C). (D) Hematoxylin and eosin staining. Columnar tumor cells, poorly differentiated and arranged in irregular glandular structures. (E) Alcian blue staining. The tissue stained positively, representing mucus-secreting cells or intraluminal mucus. (F) Epithelial membranous antigen staining. The tissue stained diffusely positive.
DISCUSSION
This is the first report to describe a major hepatectomy for curative resection of intrahepatic cholangiocarcinoma in a patient with an RSRL. An RSRL arises as a result of the diminishing of the left umbilical vein during the prenatal period. Consequently, the right umbilical vein forms the umbilical portion of the PV.^4)^ Anomalies associated with an RSRL may lead to several surgical problems during hepatectomy. Therefore, the type of anomaly should be determined during hepatectomy planning for patients with an RSRL.^4–6)^ Shindoh et al.^5)^ and Nishitai et al.^6)^ classified portal, arterial, and biliary ramifications, as discussed below.
PV ramifications of an RSRL can be classified into 3 types: the Ppost-i, P-bifurcation, and P-trifurcation types.^5)^ In the Ppost-i type, the posterior branch of the PV ramifies independently of the main portal trunk. In the P-bifurcation type, the main PV ramifies into the right PV and the LPV, similar to the normal anatomy, whereas, in the P-trifurcation type, the main PV ramifies concurrently into the left, anterior, and posterior branches. In the present case, the ramification pattern of the main portal branch was of the Ppost-i type.
Hepatic arterial ramifications of the RSRL are classified into 3 types: independent ramification of the left hepatic artery, common trunk formation between the left hepatic artery and the ventral branch of the right paramedian arteries, and replacement of the left hepatic artery by the left gastric artery.^6)^ The ramification in our case was classified as independent. Finally, intrahepatic bile-duct confluence patterns are classified into 4 types: symmetrical, independent right lateral, total left, and total right.^6)^ The pattern in our study corresponded to the total-left type. In this pattern, the entire right hemiliver is drained via a thick biliary branch that is connected to the left biliary branch and passes across the umbilical fissure towards the left and backward toward the right umbilical portions.^6)^
No specific relationship has been reported among the patterns of biliary, portal, and arterial ramifications in livers with an RSRL.^6)^ In patients with an RSRL, the proportions of the liver differ from those of a normal liver.^5,7)^ In livers with an RSRL, each side of the lateral sectors (the S2 and posterior sections) and the dorsal portion of the right paramedian sector are reportedly larger than those of typical livers, whereas the left paramedian sector (S3 + S4) and the ventral portion of the right paramedian sector are reportedly substantially smaller.^5)^ Ishida et al. proposed the following explanation for this observation: as the umbilical vein is connected to the right side of the liver, the right side of the liver may shift to the left and become enlarged, whereas the left side of the liver may shrink.^8)^
In one population of individuals with normal (left-sided) round ligaments, the posterior section of the Ppost-i type anatomy was significantly larger than that of patients with a P-bifurcation anatomy.^7)^ In the present case, the ramification pattern of the main portal branch was the Ppost-i type, and its posterior section was relatively large. Ishida et al. reported that left trisectionectomy has several surgical advantages, especially in patients with cholangiocarcinoma associated with a Ppost-i-type RSRL.^8)^ First, a large liver-remnant volume can be retained. Second, ligation and division of the ant-PV and LPV are easier in such cases. Third, bile-duct division and reconstruction can be performed in the usual manner because the biliary anatomy at the root of the posterior Glissonean pedicle is distant from the tumor, which is close to the complicated anatomy of the hepatic hilum associated with the RSRL. Although left trisectionectomy is a technically demanding operation with a relatively high mortality rate,^9,10)^ it has become one of the standard procedures for perihilar cholangiocarcinoma at high-volume centers.^11,12)^ Ishida et al. reported on a case of left trisectionectomy for perihilar cholangiocarcinoma with an RSRL and described that, in patients without invasion of the posterior section, left trisectionectomy may be favorable.^8)^ Therefore, left trisectionectomy may also be favorable for patients with intrahepatic cholangiocarcinoma close to the hilum with anomalous patterns of RSRL, as in our case, as long as the tumor does not extend into the posterior section.
Reports over the last decade on liver resection for malignant hepatobiliary tumors in patients with an RSRL are summarized in Table 1.^8,13–16)^ We summarized 12 cases, including our 3 cases (this case and 2 prior cases). In all cases, an RSRL and an anomaly of vascular ramification were observed upon preoperative CT. Modified hepatectomy was performed in all of those previous studies, according to the portal, arterial, and biliary ramifications, without major complications.
Preoperative liver simulations have demonstrated the characteristics of ideal simulation and navigation tools.^17)^ Simulations can accurately predict the liver volume to be resected and permit stereotactic measurement of the length of the surgical margin. In the present case, the most useful contribution of liver simulation was the visualization of the volume and 3-D structure of the intrahepatic vasculature. 3-D simulations based on precise intrahepatic vascular and biliary analyses enable accurate and oncologically curative hepatic resection, even in patients with rare anatomical anomalies.
CONCLUSIONS
The vascular and biliary anatomy of patients with an RSRL is complicated and should be evaluated in detail before surgery by using a hepatectomy simulation system, especially when curative hepatic resection is performed for intrahepatic or perihilar cholangiocarcinoma.
DECLARATIONS
Funding
The authors declare that they received no funding for this study.
Authors’ contributions
MU drafted the manuscript and provided the original figures.
MI critically reviewed and revised the manuscript.
KK and NT collected the clinical and radiological data.
KO, NO, KY, HO, RH, HM, YT, and SO reviewed the manuscript.
RO provided pathological data.
All authors read and approved the final manuscript.
Availability of data and materials
The data generated and/or analyzed in this study will be made available upon reasonable request.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Informed consent to publish the case details was obtained from the patient.
Conflicts interest
None of the authors have conflicts of interest to report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matsumoto T Aoki T Iso Y Successful right hemihepatectomy for a patient with right-sided round ligament. J Gastrointest Surg 2016; 20: 470–2.26501482 10.1007/s 11605-015-2992-z · doi ↗ · pubmed ↗
- 2Maetani Y Itoh K Kojima N Portal vein anomaly associated with deviation of the ligamentum teres to the right and malposition of the gallbladder. Radiology 1998; 207: 723–8.9609896 10.1148/radiology.207.3.9609896 · doi ↗ · pubmed ↗
- 3MB. A American Joint Committee on Cancer, American Cancer Society. AJCC cancer staging manual. Eighth Edition. IL American Joint Committee on Cancer, Chicago, Springer, 2017.
- 4Nagai M Kubota K Kawasaki S Are left-sided gallbladders really located on the left side? Ann Surg 1997; 225: 274–80.9060583 10.1097/00000658-199703000-00006 PMC 1190677 · doi ↗ · pubmed ↗
- 5Shindoh J Akahane M Satou S Vascular architecture in anomalous right-sided ligamentum teres: three-dimensional analyses in 35 patients. HPB (Oxford) 2012; 14: 32–41.22151449 10.1111/j.1477-2574.2011.00398.x PMC 3252989 · doi ↗ · pubmed ↗
- 6Nishitai R Shindoh J Yamaoka T Biliary architecture of livers exhibiting right-sided ligamentum teres: an indication for preoperative cholangiography prior to major hepatectomy. HPB (Oxford) 2016; 18: 929–35.27594117 10.1016/j.hpb.2016.08.002PMC 5094486 · doi ↗ · pubmed ↗
- 7Watanabe N Ebata T Yokoyama Y Anatomic features of independent right posterior portal vein variants: Implications for left hepatic trisectionectomy. Surgery 2017; 161: 347–54.27692569 10.1016/j.surg.2016.08.024 · doi ↗ · pubmed ↗
- 8Ishida T Nara S Akahoshi K Left hepatic trisectionectomy for perihilar cholangiocarcinoma with a right-sided round ligament: A case report. World J Gastrointest Surg 2020; 12: 68–76.32128030 10.4240/wjgs.v 12.i 2.68PMC 7044109 · doi ↗ · pubmed ↗