Diagnostic value of ratio of blood inflammation to coagulation markers in periprosthetic joint infection
Jincheng Huang, Xu Li, Yajun Chen, Meng Zhang, Zongyan Gao, Zhipeng Dai, Tao Liu, Yi Jin

TL;DR
This study explores using ratios of blood inflammation and coagulation markers to help diagnose joint infections after surgery.
Contribution
It introduces new diagnostic ratios combining inflammation and coagulation markers for periprosthetic joint infection detection.
Findings
PJI patients showed significantly higher levels of multiple inflammation and coagulation markers.
Ratios like CRP/fibrinogen and ESR/fibrinogen had diagnostic accuracy comparable to traditional markers.
Combining CRP with ratios improved diagnostic performance similar to combining CRP and ESR.
Abstract
Assess the feasibility of utilizing the ratio of blood inflammation to coagulation markers as a potential periprosthetic joint infection (PJI) diagnostic tool. A retrospective analysis was conducted, involving 133 PJI and 93 aseptic loosening patients. Levels of C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), platelet count, mean platelet volume, fibrinogen, D-dimer, and ratios of CRP to fibrinogen, ESR to fibrinogen, platelet count and mean platelet volume ratio (PC/MPV), and D-dimer were compared. Receiver operating characteristic curves and Youden’s index were employed to assess the diagnostic efficacy of these biomarkers. PJI patients had significantly higher levels of CRP, ESR, PC/MPV ratio, fibrinogen, D-dimer, CRP/(PC/MPV) ratio (CPR), CRP/D-dimer, CRP/fibrinogen (CFR), ESR/(PC/MPV) ratio, ESR/D-dimer, and ESR/fibrinogen. Area under the curve (AUC) values for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
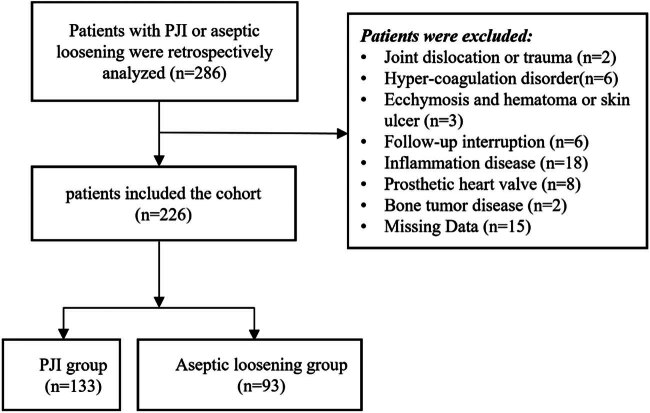 Figure 1
Figure 1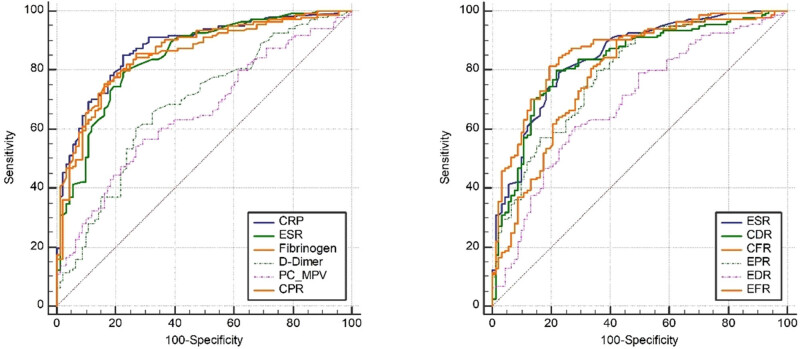 Figure 2
Figure 2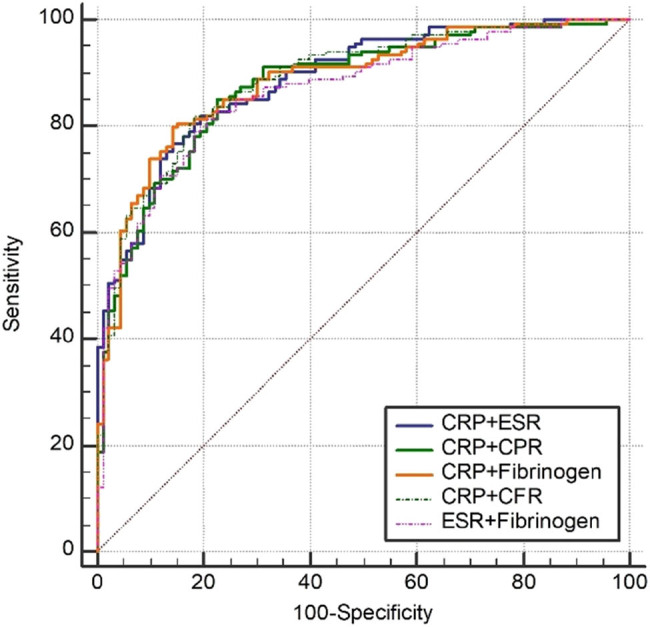 Figure 3
Figure 3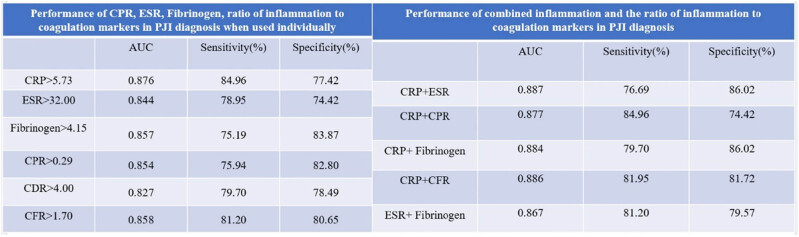 Figure 4
Figure 4| Parameters | PJI ( | Aseptic loosening ( |
|
|---|---|---|---|
|
| 0.181* | ||
| Male | 59 (44.36) | 33 (35.48) | |
| Female | 74 (55.64) | 60 (64.52) | |
| Affected joints, | <0.001* | ||
| Knee | 68 (51.13) | 19 (20.43) | |
| Hip | 65 (48.87) | 74 (79.57) | |
|
| 64.74 (12.09) | 65.94 (9.63) | 0.427† |
|
| 51.67 (14.33) | 49.57 (16.38) | 0.310† |
| Parameters | PJI group | Aseptic loosening group |
|
|---|---|---|---|
| CRP | 36.76 ± 41.89 mg/L | 4.85 ± 8.65 mg/L | <0.001* |
| ESR | 57.62 ± 30.97 mm/h | 22.08 ± 19.84 mm/h | <0.001* |
| PC/MPV ratio | 31.95 ± 15.59 | 24.41 ± 9.57 | <0.001* |
| Fibrinogen | 4.90 ± 1.66 μg/L | 3.21 ± 0.86 μg/L | <0.001* |
| D-dimer | 2.28 ± 2.53 μg/L | 1.26 ± 1.30 μg/L | <0.001* |
| CPR | Sum of rank 19,477 | Sum of rank 6,174 | <0.001# |
| Mean rank 46.44 | Mean rank 66.39 | ||
| CDR | 28.19 ± 47.07 | 6.35 ± 20.61 | <0.001* |
| CFR | 6.77 ± 6.66 | 1.30 ± 2.13 | <0.001* |
| EPR | Sum of rank 18,710 | Sum of rank 6,941 | <0.001* |
| Mean rank 140.68 | Mean rank 74.63 | ||
| EDR | 45.32 ± 39.20 | 25.57 ± 24.83 | <0.001* |
| EFR | 11.45 ± 5.11 | 6.24 ± 4.50 | <0.001* |
| AUC | 95% confidence interval | Associated criterion | Youden index | Sensitivity (%) | Specificity (%) | Significance level | |
|---|---|---|---|---|---|---|---|
| CRP | 0.876 | 0.826–0.916 | >5.73 | 0.6238 | 84.96 | 77.42 | <0.0001 |
| ESR | 0.844 | 0.790–0.889 | >32.00 | 0.5637 | 78.95 | 74.42 | <0.0001 |
| PC/MPV ratio | 0.652 | 0.586–0.714 | >26.77 | 0.2736 | 56.39 | 70.97 | <0.0001 |
| Fibrinogen | 0.857 | 0.805–0.900 | >4.15 | 0.5906 | 75.19 | 83.87 | <0.0001 |
| D-dimer | 0.682 | 0.617–0.743 | >1.26 | 0.3327 | 60.15 | 73.12 | <0.0001 |
| CPR | 0.854 | 0.801–0.898 | >0.29 | 0.5874 | 75.94 | 82.80 | <0.0001 |
| CDR | 0.827 | 0.771–0.874 | >4.00 | 0.5819 | 79.70 | 78.49 | <0.0001 |
| CFR | 0.858 | 0.806–0.901 | >1.70 | 0.6185 | 81.20 | 80.65 | <0.0001 |
| EPR | 0.792 | 0.733–0.843 | >0.97 | 0.4422 | 79.70 | 64.52 | <0.0001 |
| EDR | 0.688 | 0.624–0.748 | >25.71 | 0.3295 | 60.90 | 72.04 | <0.0001 |
| EFR | 0.788 | 0.729–0.839 | >5.90 | 0.4829 | 90.23 | 58.06 | <0.0001 |
| ESR | PC/MPV ratio | Fibrinogen | D-dimer | CPR | CDR | CFR | EPR | EDR | EFR | |
|---|---|---|---|---|---|---|---|---|---|---|
| CRP |
|
|
|
|
|
|
|
|
|
|
| ESR | — |
|
|
|
|
|
|
|
|
|
| PC/MPV ratio |
| — |
|
|
|
|
|
|
|
|
| Fibrinogen | — | — | — |
|
|
|
|
|
|
|
| D-dimer | — | — | — | — |
|
|
|
|
|
|
| CPR | — | — | — | — | — |
|
|
|
|
|
| CDR |
| — | — | — | — | — |
|
|
|
|
| CFR |
| — | — | — | — | — | — |
|
|
|
| EPR | — | — | — | — | — | — | — | — |
|
|
| EDR | — | — | — | — | — | — | — | — | — |
|
| EFR | — | — | — | — | — | — | — | — | — | — |
| AUC | 95% confidence interval | Youden index | Sensitivity (%) | Specificity (%) | Significance level | |
|---|---|---|---|---|---|---|
| CRP + ESR | 0.887 | 0.838–0.925 | 0.6271 | 76.69 | 86.02 | <0.0001 |
| CRP + CPR | 0.877 | 0.826–0.916 | 0.6238 | 84.96 | 74.42 | <0.0001 |
| CRP + fibrinogen | 0.884 | 0.835–0.923 | 0.6572 | 79.70 | 86.02 | <0.0001 |
| CRP + CFR | 0.886 | 0.838–0.925 | 0.6368 | 81.95 | 81.72 | <0.0001 |
| ESR+ fibrinogen | 0.867 | 0.815–0.908 | 0.6077 | 81.20 | 79.57 | <0.0001 |
| CRP + CPR | CRP + fibrinogen | CRP + CFR | ESR + FIB | |
|---|---|---|---|---|
| CRP + ESR |
|
|
|
|
| CRP + CPR | — |
|
|
|
| CRP + fibrinogen | — | — |
|
|
| CRP + CFR | — | — | — |
|
| ESR + fibrinogen | — | — | — | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Orthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes
Introduction
1
While C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are commonly recommended blood inflammation markers for diagnosing periprosthetic joint infection (PJI) according to several PJI diagnosis guidelines [1,2,3,4,5], their performance may be suboptimal in certain situations, such as in cases of low-grade virulence or chronic PJI [6]. Thus, the search for new adjunct markers for PJI diagnosis remains a critical focus in current orthopedic research [7,8,9,10,11]. Building on the coagulation and inflammation theory [12], various authors have investigated the roles of commonly used coagulation markers, such as D-dimer [7], fibrin degradation product (FDP) [13], platelet count and mean platelet volume ratio (PC/MPV) [14], and fibrinogen [8,15,16] in PJI diagnosis over the past few years. However, the significance of D-dimer and PC/MPV ratio in PJI diagnosis remains a topic of debate [14,17,18,19]. While individual inflammation or coagulation markers may contribute to PJI diagnosis, the utility of the ratio of inflammation to coagulation markers for this purpose has been underexplored [20]. Understanding the precise value of the ratio of inflammation to coagulation markers in PJI diagnosis may offer additional adjunct markers for PJI diagnosis. This study aims to: (1) evaluate the utility of traditional inflammation or coagulation markers in PJI diagnosis when used individually; (2) assess the significance of the ratio of inflammation to coagulation markers in PJI diagnosis; and (3) appraise the value of combined inflammation and the ratio of inflammation to coagulation markers in PJI diagnosis.
Materials and methods
2
Study design and settings
2.1
The retrospective study design consisted of patients diagnosed with PJI and aseptic loosening at our department from January 2017 to December 2022. This retrospective study received approval from the Ethics Board of Henan Provincial People’s Hospital and adhered to the principles of the Declaration of Helsinki. Given the retrospective design of the study, the requirement for informed consent was waived by the Ethics Board of Henan Provincial People’s Hospital.
Study protocol
2.2
After the ethics committee approval was received, the data on the hospital’s data network were retrospectively examined for patients diagnosed with PJI and aseptic loosening. Clinical data, including sex, age, duration of follow-up, type of affected joints, preoperative CRP, ESR, D-dimer, PC/MPV ratio, fibrinogen, CRP/D-dimer (CDR), CRP/(PC/MPV) ratio (CPR), CFR (CRP/fibrinogen), ESR/D-dimer (EDR), ESR/(PC/MPV) ratio (EPR), and ESR/fibrinogen (EFR) levels, were evaluated.
The exclusion criteria were defined as follows: (1) presence of visible ecchymosis; (2) history of recent dislocation or trauma (within 2 weeks); (3) presence of hematoma or any type of skin ulcer; (4) history of hypercoagulation disorder; (5) presence of a prosthetic heart valve; (6) diagnosis of a systemic inflammatory disease; and (7) history of tumor. Detailed information on these exclusion criteria can be found in our previously published paper [17].
PJI was defined in accordance with the criteria set forth by the Musculoskeletal Infection Society (MSIS) [21]. Aseptic loosening was defined based on the following criteria: (1) presence of thigh or hip region pain and knee pain; (2) radiological evidence of loosening (such as disintegration of prosthesis components with the bone, displacement of prosthesis components, or circumferential radiolucent line); and (3) absence of criteria indicative of PJI.
Data analysis
2.3
Quantitative data were presented as mean ± standard deviation, and comparisons between multiple groups were conducted using a single-factor analysis of variance. The Student–Newman–Keuls test was employed for normally distributed data, while Tamhane’s T2 test was utilized for non-normally distributed data when comparing two means. The chi-square test (χ ^2^) was used for comparing categorical data among groups. Statistical significance was set at P < 0.05. Statistical analyses were performed using IBM SPSS Statistics version 19 (IBM SPSS Software).
The performance of CRP, ESR, D-dimer, PC/MPV ratio, fibrinogen, CDR, CPR, CFR, EDR, EPR, EFR, as well as combinations of CRP or ESR with CDR, CPR, CFR, EDR, EPR, or EFR, was evaluated through receiver operating characteristic (ROC) analyses using MedCalc 19.0.4 (MedCalc Software, Ostend, Belgium). Parameters such as sensitivity, specificity, and the area under the curve (AUC) were assessed, with an AUC of >0.7 considered acceptable. Optimal thresholds were determined using Youden’s index. DeLong’s test was used to compare the AUC of different markers in PJI diagnosis.
Informed consent: Given the retrospective nature of the study and the use of de-identified patient data, the requirement for informed consent was waived by the Ethics Board of Henan Provincial People s Hospital. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments. Ethics approval: This retrospective study was approved by the Ethics Board of Henan Provincial People’s Hospital.
Results
3
Demographic characteristics of the enrolled patients
3.1
A total of 286 patients presenting with PJI or aseptic loosening at our department between January 2017 and December 2022 were included in this retrospective study. Fifteen cases were excluded due to incomplete demographic, clinical information, and laboratory results. Two cases were excluded due to a recent history of dislocation or trauma (within 2 weeks), while 6 cases were excluded due to a history of hypercoagulation disorder. Three cases were excluded due to visible ecchymosis, hematoma, or skin ulcer, and 18 cases were excluded due to a history of systemic inflammatory disease. Additionally, eight cases were excluded due to the presence of a prosthetic heart valve, six cases due to interrupted follow-up, and two cases due to primary joint arthroplasty for bone tumor disease. Ultimately, 226 patients met the inclusion and exclusion criteria for this study (Figure 1). All patients were followed up for at least 2 years. The patients’ demographic details were recorded in an electronic database (Table 1). There was no significant difference when compared with the sex, age, and duration of follow-up between patients from the two groups, while there was a significant difference when compared with the type of affected joints between patients from the two groups.
Flow diagram of included patients.
Value of fibrinogen, D-dimer, PC/MPV ratio, CPR, CDR, CFR, EPR, EDR, and EFR in PJI diagnosis
3.2
In the initial analysis, levels of CRP, ESR, PC/MPV ratio, fibrinogen, D-dimer, CPR, CDR, CFR, EPR, EDR, and EFR were compared between patients in the two groups. As depicted in Table 2, the PJI group exhibited significantly elevated levels of CRP, ESR, PC/MPV ratio, fibrinogen, D-dimer, CPR, CDR, CFR, EPR, EDR, and EFR compared to the aseptic loosening group. Tables 3 and 4 and Figure 2 illustrate that fibrinogen demonstrated diagnostic performance comparable to CRP and ESR in PJI diagnosis. Moreover, CPR and CFR exhibited diagnostic performance lower than CRP but similar to ESR in PJI diagnosis. These findings suggest that fibrinogen, CPR, and CFR could serve as supplementary markers for aiding in the diagnosis of PJI.
ROC curve of CRP, ESR, fibrinogen, and ratio of inflammation to coagulation markers in PJI diagnosis.
Performance of combine CRP or ESR with fibrinogen, CPR, or CFR in PJI diagnosis
3.3
While CRP and ESR are commonly recommended for PJI diagnosis based on the MSIS criteria [21] and the guidelines from the Infectious Diseases Society of America [22], our study suggests that fibrinogen, CPR, and CFR could also be valuable markers for diagnosing PJI. However, not all patients may have complete data available for all these inflammation and coagulation markers at the time of suspected PJI presentation. Therefore, we propose the use of combined CRP or ESR with fibrinogen, CPR, or CFR for PJI diagnosis in cases where all coagulation markers or both CRP and ESR results are not available. Utilizing the ROC curve and AUC, we determined the optimal threshold values, specificity, and sensitivity of these combined markers in PJI diagnosis. As demonstrated in Tables 5 and 6 and Figure 3, the diagnostic performance of combining CRP with CPR, fibrinogen, or CFR, as well as combining ESR with fibrinogen, was comparable to that of combining CRP with ESR. These findings support the use of combined CRP and CPR, combined CRP and fibrinogen, combined CRP and CFR, and combined ESR and fibrinogen for diagnosing PJI.
ROC curve of combined CRP or ESR with fibrinogen, CPR, or CFR in PJI diagnosis.
Discussion
4
While traditional inflammation markers such as CRP and ESR are commonly utilized for PJI diagnosis, and individual blood coagulation markers like D-dimer, PC/MPV ratio, and fibrinogen have shown promise in identifying PJI, accurately diagnosing PJI based solely on limited inflammation or coagulation markers during the initial consultation remains challenging. Enhancing PJI diagnostic precision with restricted inflammation or coagulation data necessitates further investigation. In our study, we not only established the utility of fibrinogen, CPR, and CFR as standalone markers for PJI diagnosis but also proposed that combining CRP with fibrinogen, CFR, or ESR could serve as novel auxiliary markers for enhancing PJI diagnosis accuracy.
Since Shahi et al. first highlighted the potential of D-dimer as a blood coagulation marker for diagnosing PJI in 2017 [7], there has been a surge of studies investigating the role of coagulation markers in PJI diagnosis over the past five years. While the significance of fibrinogen and FDP in PJI diagnosis has been widely acknowledged across various studies [8,13,15,16],the utility of D-dimer and PC/MPV ratio in PJI diagnosis remains a topic of debate [14,17,18,23–26]. In our study, we conducted a comparative analysis of D-dimer, PC/MPV ratio, and fibrinogen in PJI diagnosis against CRP and ESR. Our findings revealed that the AUC of fibrinogen in PJI diagnosis was comparable to that of CRP and ESR, whereas the AUC of D-dimer and PC/MPV ratio in PJI diagnosis was lower than that of CRP and ESR. These results suggest that fibrinogen could serve as a valuable new auxiliary marker for PJI diagnosis, while D-dimer and PC/MPV ratio may not be as effective in this regard.
Diagnosing PJI accurately can be challenging when patients with suspected PJI exhibit limited inflammation or coagulation markers. While individual inflammation or coagulation markers can aid in PJI diagnosis, the potential of the inflammation-to-coagulation marker ratio or combining CRP or ESR with fibrinogen, CPR, CDR, or CFR for PJI diagnosis remains underexplored [20]. In this study, we discovered that the performance of CPR and CFR in PJI diagnosis was similar to that of ESR, and CPR and CFR can be used as new auxiliary markers for PJI diagnosis. Then, we found that AUC of combined CRP and CPR, combined CRP and FIB, combined CRP and CDR, combined CRP and CFR, combined ESR and fibrinogen in PJI diagnosis were similar with combined CRP and ESR in PJI diagnosis, combined CRP and CPR, combined CRP and FIB, combined CRP and CDR, combined CRP and CFR, combined ESR and fibrinogen can be used as for PJI diagnosis.
Study limitations
5
However, our study has several limitations: (1) being retrospective, it may be subject to inherent recall and reporting biases; (2) being single-center, a multicenter study would be beneficial to validate our findings; (3) exclusion criteria such as visible ecchymosis, recent dislocation or trauma, hematoma, hypercoagulation disorder, prosthetic heart valve, systemic inflammatory disease, and tumor may have limited the generalizability of our conclusions; (4) the sample size of 226 patients in our study is relatively small, warranting further investigation with a larger cohort; and (5) this study proposes a methodology based on statistical analysis to further evaluate clinical data with the aim of providing new insights into the diagnosis of PJI. However, we recognize that the application of these methods requires some statistical background and skills, which may pose a challenge to some clinicians. While our methods are theoretically innovative and potentially clinically applicable, they may encounter operational complexity in practical application. Therefore, exploring collaboration with experts in the fields of computer science and biostatistics in future studies to develop an algorithm and corresponding application that can accurately predict the probability of a PJI diagnosis would greatly improve diagnostic accuracy and provide clinicians with stronger decision support.
Conclusions
6
In this study, our findings suggest the following: 1, fibrinogen, CPR, and CFR can be utilized individually for PJI diagnosis; 2, combined CRP and CPR, combined CRP and fibrinogen, combined CRP and CFR, as well as combined ESR and fibrinogen, demonstrate potential as novel auxiliary indicators for PJI diagnosis (Figure 4). Fibrinogen, CPR, CFR, combined CRP and CPR, combined CRP and fibrinogen, combined CRP and CDR (CRP/D-dimer), combined CRP and CFR, and combined ESR and fibrinogen are potential auxiliary markers that can be considered for PJI diagnosis.
Graphical representation of different markers in PJI diagnosis.
Abbreviations
PJIperiprosthetic joint infectionCRPC-reactive proteinESRerythrocyte sedimentation ratePC/MPVplatelet count and mean platelet volume ratioFDPfibrin degradation products