Minimal intervention dentistry for treating primary teeth: a survey study among members of the Israeli Society of Paediatric Dentistry
M. Moskovitz, T. Elkesslasy, A. Shmueli, E. Halperson, D. Ram, A. Fux-Noy

TL;DR
This study explores how Israeli pediatric dentists approach minimal intervention for treating decay in children's primary teeth.
Contribution
It provides insights into the clinical practices of Israeli dentists regarding minimal intervention in primary teeth treatment.
Findings
Most dentists intervene at later stages of caries in primary molars.
Conservative techniques are commonly used for restoring primary teeth.
Both specialists and non-specialists follow minimal intervention principles.
Abstract
To assess the attitudes of dentists in Israel to minimal intervention on primary teeth. For this cross-sectional study, data were accessed from questionnaires that were completed anonymously by members of the Israeli Society of Paediatric Dentistry. For four clinical scenarios, the respondents were asked to describe the stage at which they would intervene, the type of preparation they would utilize, and the restorative materials they would use. The scenarios included proximal and occlusal caries in the primary molar and buccal and proximal caries in the primary maxillary incisor. Forty-six dentists completed the questionnaire. Forty-one (89%) cited that they would intervene in stages 3 and 4 (of 6) of proximal caries in the primary molar; 34 of these stated that the cavity preparation would be of the proximal box type. For occlusal caries, 37 (80%) stated they would intervene in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
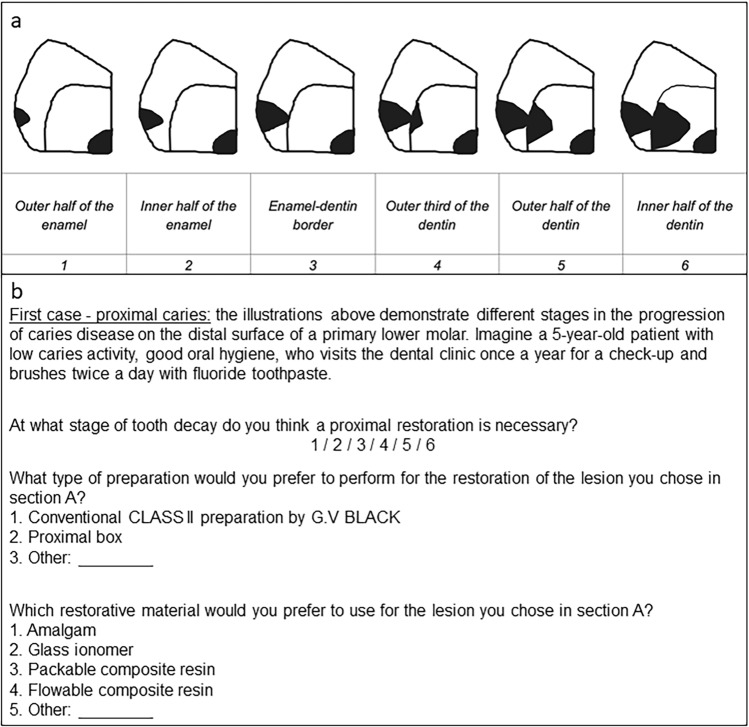 Figure 1
Figure 1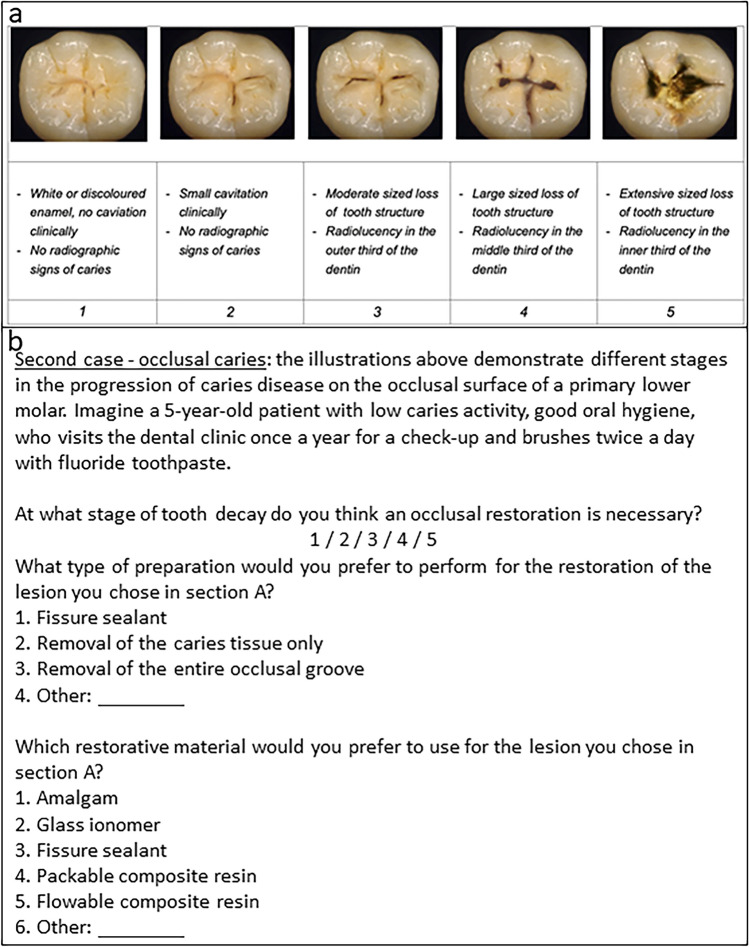 Figure 2
Figure 2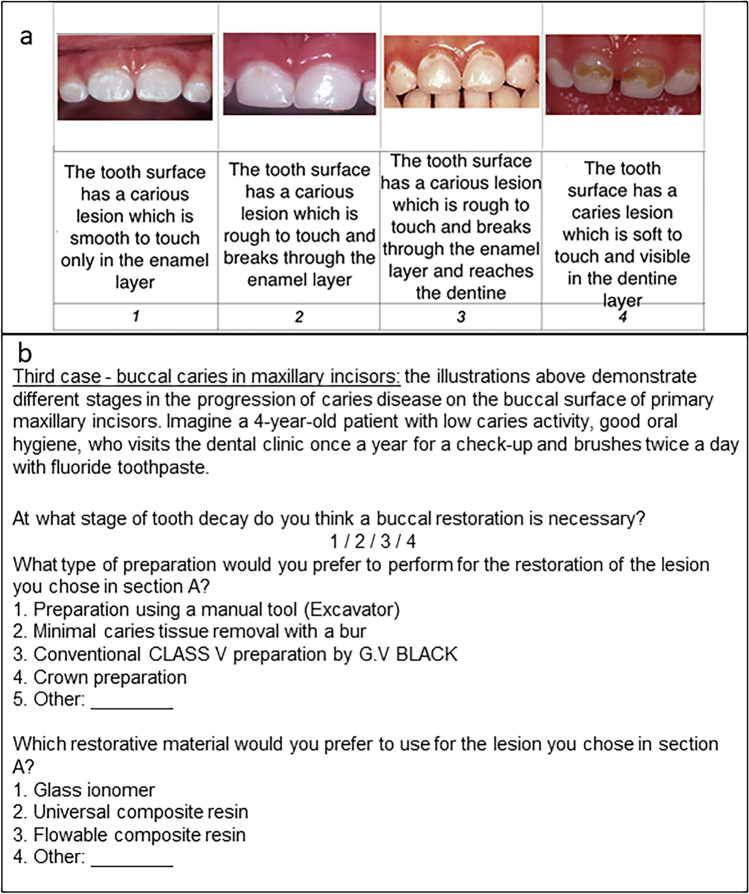 Figure 3
Figure 3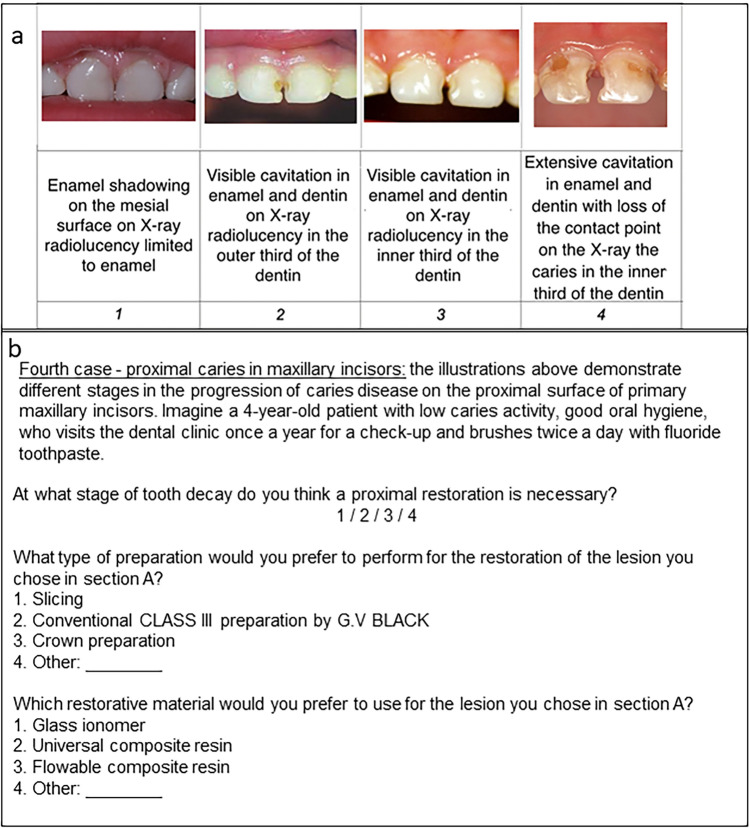 Figure 4
Figure 4- —Hebrew University of Jerusalem
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Oral microbiology and periodontitis research · Dental Research and COVID-19
Background
Early childhood caries (ECC) is still a prevalent disease among preschool-aged children, regardless of their country's level of development. However, worsening can be prevented by the provision of diet advice, the promotion of good oral hygiene practices, and the utilization of preventive measures such as topical fluoride. Management of ECC often requires restorative treatment at an early age (Berkowitz 2003; Anil and Anand 2017). Those treatments require local anesthesia and the use of a rotatory handpiece, which can initiate negative behavior in children (Santamaria et al. 2015). General anesthesia, deep sedation, or moderate sedation is sometimes required, due to the difficulty of young children to cope with the extensive treatment procedures (Berkowitz 2003; Anil and Anand 2017). Restorative dentistry has little to no long-term impact on oral bacteria like S. mutans. Hence, the clinical outcomes for treating ECC are poor. Many treated children experience new caries lesions within 6–24 months after initial dental treatment (Berkowitz 2003). The approach of restoring primary teeth has been questioned (Innes et al. 2013; Hansen and Nyvad 2017), as a large proportion of primary teeth with untreated carious lesions exfoliate without showing any symptoms (Hu et al. 2013). Minimal intervention dentistry is an alternative approach for managing dental caries, which focuses on prevention and early detection rather than surgical intervention. The core principles of minimal intervention dentistry can be summarized as Recognition of disease contributory factors; Re-orientation of contributory lifestyle factors; Remineralization of all lesions, visible and not visible, cavitated and non-cavitated; Repair, where no other solution is possible; and Review of the child, their oral health, and their life environment. These core principles of minimal intervention dentistry enable comprehensive patient/family assessment, with early diagnosis of carious lesions, reliable caries risk assessment, implementation of effective preventive measures, and minimally harmful restorative care (Innes and Manton 2017).
Carious lesions should be repaired when cavitation results in a non-cleanable lesion, weakens the tooth structure or compromises esthetics. In the sealing-in technique, the cariogenic biofilm is managed by its being sealed from the oral environment. Carious lesions isolated from the oral environment do not progress if the seal is effective and durable over time. Sealing-in strategies include the use of fissure sealants to arrest carious lesions in pits and fissures that did not progress past micro-cavitation, sealing with a preformed metal crown (Hall Technique) with no carious tissue removal, and sealing with an adhesive restorative material after selective (partial) carious tissue removal (Innes and Manton 2017). Based on a survey of dentists, Laske et al. (2019) concluded that a global shift toward less-invasive methods for treating caries lesions had not occurred, neither in the initiation of treatment nor in the preparation techniques used. However, in some countries, changes over time could be assessed, indicating that more dentists postpone interventions until lesions progress to a deeper level. The researchers found that dentists worldwide tend to intervene operatively too early for caries though this differs across countries. A worldwide shift was observed in the restorative material applied as the composite resin has almost completely replaced amalgam for restoring primary caries lesions.
Several studies (Espelid et al. 1985, 2001; Laske et al. 2019) described the conservative choices made by dentists regarding treatment thresholds and restorative techniques in permanent teeth. The current study aimed to investigate dentists' choices in treating primary teeth. The main objective was to assess the attitudes of dentists in Israel to minimal intervention on primary teeth. To this end, we inquired regarding the stage at which dentists would choose to intervene invasively, and the type of intervention and the material they would use. The secondary objective was to explore associations between the characteristics of dentists and their choices.
Materials and methods
Study population and design
This cross-sectional study was based on the analysis of data accessed from questionnaires that were distributed online to members of the Israeli Society of Dentistry for Children (ISDC). The members of ISDC are specialists and residents in pediatric dentistry and general practitioners who treat children. The study inclusion criteria were dentists who were members of ISDC in 2022, and who filled and submitted questionnaires.
Study tool
The research tool used was an anonymous pre-coded questionnaire that was developed by Laske et al. (2019) and modified by our research team for use in pediatric dentistry. The modifications included transforming presentations on permanent molars to primary molars and adding two presentations of caries lesions in primary maxillary incisors. The questionnaire consists of two parts. The first part collects demographic data while the second part contains four case presentations. These presentations include figures or photographs of several stages of proximal and occlusal lesions of primary molars, and buccal and proximal lesions of primary maxillary incisors. The questionnaire also includes items about restorative treatment criteria, preparation techniques, and the use of restorative materials.
The questionnaire was translated into Hebrew using the "forward–backward translation" method, from English to Hebrew and then into English; followed by a comparison of the English translation to the original version, to locate and bridge translation gaps. After formulating the questionnaire, a pilot study was conducted with five pediatric dentists. They were asked to fill out the questionnaire and answer follow-up questions regarding the clarity of the instructions, any difficulties in completing the items or unclear phrases, and related issues. Based on their feedback, the necessary changes were made to the questionnaire.
Ethics
The study was approved by the Institutional Human Subjects Ethics Committee (HMO-0345-22) and conforms to the declaration of Helsinki. The committee approved the waiver of a separate consent form. Participants provided informed consent by completing and submitting the questionnaire. Only questionnaires that were fully completed and submitted were included in the study.
Statistical analysis
Descriptive statistics were used to present the data numerically. Frequency distributions and percentages were used to describe qualitative variables. Means, standard deviations, and minimum and maximum values were calculated for quantitative variables. Chi-square tests were conducted to examine independence between pairs of categorical variables. When significance was achieved, tables of residuals were used to assess associations between the categories examined. If the residual value was positive, the association between the two categories was deemed positive. The larger the residual value, the more dominant the association. All the statistical tests were analyzed for a significance level of p-value < 0.05. Analyses were performed using R software version 4.1.3.
Results
Of 150 ISDC members who received the questionnaire, 106 opened the link and 46 completed and submitted the questionnaire. Accordingly, the response rate was 30.6%. For the distribution of demographic characteristics, see Table 1.Table 1. Distribution of sociodemographic variables in the sample (N = 46)VariableValuesIncidencePercentageMeanSDRangeGenderMale1533Female3065NA12Type of clinicPrivate2759Public1941Dentist's statusSpecialist2963Resident1226General practitioner511Age (years)54.711.230–76Years of experience18.011.91–50SD, standard deviation; NA, not applicable
For a proximal caries lesion in the primary molar (Fig. 1), 20 (43.5%) respondents stated they would intervene in stage 3 and 21 (45.5%) stated they would intervene in stage 4 of the lesion. Of these 41 participants, 34 stated that the cavity preparation would be a proximal box (Table 2). A significant association was found between the dentist's status and the type of preparation performed (χ^2^ = 7.3251, df = 2, p-value = 0.025); general practitioners preferring to perform a traditional Class II preparation (Table 3).Fig. 1. Case presentation of a proximal caries lesion in a primary molar: a illustration [from Laske et al 2019] b questionsTable 2Results of the chi-squared test for independence between the stage of the proximal caries lesion in the primary molar and the study variablesProximal lesion—primary molarThe stage of caries lesion in which restoration is necessaryTotalStatistical data12345Preparation techniqueProximal box111519238χ^2^ = 3.8225df = 4p-value = 0.430Conventional Class II preparation by G.V Black015208Total122021246The restorative materialGlass ionomer001113χ^2^ = 13.291df = 8p-value = 0.102Packable composite resin021716136Flowable composite resin102407Total122021246Table 3Table of residualsDentist's statusProximal boxConventional Class II preparationSpecialist0.4175016 − 0.90992363Resident0.02761841 − 0.06019293General practitioner − 1.048263252.28463678Results of the chi-squared test for independence between the type of proximal preparation in the primary molar and the dentist's status
For an occlusal caries lesion (Fig. 2), 19 (41.3%) respondents stated they would intervene in stage 2 and 18 (39.1%) stated they would intervene in stage 3. Of these 37 participants, 31 would remove only the carious lesion (Table 4). A significant association was found between the stage of caries lesion in which the dentists would intervene and the type of preparation they would perform (p-value = 0.004). Accordingly, in an early-stage intervention, preparation for fissure sealant would be performed; while in a later stage of intervention, conventional Class I preparation would be performed (Table 5). A significant association was also found between the stage of caries lesion in which the dentists stated they would intervene and the restorative material they would use (p-value = 0.004) (Table 4). At intervention in the early stage, more fissure sealants and flowable composite materials would be used. In the later stages, a packable composite would be applied (Table 6).Fig. 2. Case presentation of an occlusal caries lesion in a primary molar: a illustration [from Laske et al 2019] b questionsTable 4Results of the chi-squared test for independence between the stage of the occlusal caries lesion in the primary molar and the study variablesOcclusal lesion—primary molarThe stage of caries lesion in which restoration is necessaryTotalStatistical data1234Preparation techniqueFissure sealant15006χ^2^ = 18.653df = 6p-value = 0.004Removal of the caries tissue only01417637Conventional Class I preparation by G.V Black00123Total11918846The restorative materialOther material00011χ^2^ = 28.697df = 12p-value = 0.004Fissure sealant13004Glass ionomer046111Packable composite resin018211Flowable composite resin0114419Total11918846Table 5Table of residualsThe stage of caries lesion in which occlusal restoration is necessaryFissure sealantRemoval of the caries tissue onlyConventional Class I preparation12.407717 − 0.8968544 − 0.25537721.601868 − 0.3280918 − 1.11316243 − 1.5322620.6627381 − 0.16051454 − 1.021508 − 0.17139782.0465595Results of the chi-squared test for independence between the stage of occlusal caries lesion in the primary molar and the type of preparationTable 6Table of residualsThe stage of caries lesion in which occlusal restoration is necessaryOther materialFissure sealantGlass ionomerPackable composite resinFlowable composite resin1 − 0.1474423.0962811 − 0.48901 − 0.48900965 − 0.64268462 − 0.64268461.0485906 − 0.254969 − 1.662400061.12521493 − 0.6255432 − 1.25108650.8173031.7813014 − 1.259694241.9808869 − 0.8340577 − 0.6601290.062869460.3826919Results of the chi-squared test for independence between the stage of the occlusal caries lesion in the primary molar and restorative material
For buccal caries in the primary incisor (Fig. 3), 33 (72%) respondents stated they would intervene at stage 3 and remove minimal caries tissue (Table 7). A clear association was found between the stage of caries lesion in which dentists would intervene and the type of preparation they would choose (p-value < 0.001) (Table 7). Intervention at a later stage involves preparation for a crown (Table 8). The results also showed a significant association between the stage of caries lesion at which dentists stated they would intervene and the restorative material they would use (p-value < 0.001) (Table 7). Glass ionomer and universal composite resins were preferred for the later stages of the disease (Table 9).Fig. 3. Case presentation of a buccal caries lesion in a primary maxillary incisor: a illustration b questionsTable 7Results of the chi-squared test for independence between the stage of buccal caries lesion in the primary incisor and study variablesBuccal lesion—primary maxillary incisorThe stage of caries lesion in which restoration is necessaryTotalStatistical data1234Preparation techniqueOther preparation10001χ^2^ = 51.811df = 9p-value < 0.001Crown preparation00437Conventional Class V preparation by G.V Black00505Caries tissue removal with bur0424533Total1433846The restorative materialOther material10102χ^2^ = 33.507df = 9p-value < 0.001Glass ionomer00336Universal composite resin0112518Flowable composite resin0317020Total1433846Table 8Table of residualsThe stage of caries lesion in which buccal restoration is necessaryOther preparationCrown preparationConventional Class V preparationCaries tissue removal16.634888 − 0.3900947 − 0.3296902 − 0.846989552 − 0.2948839 − 0.7801895 − 0.65938050.66732513 − 0.8469896 − 0.45594550.74609210.067019074 − 0.41702881.6156263 − 0.9325048 − 0.30853045Results of the chi-square test for independence between the stage of buccal caries lesion in the primary incisor and preparation typeTable 9Table of residualsThe stage of caries lesion in which buccal restoration is necessaryOther materialGlass ionomerUniversal composite resinFlowable composite resin14.5873171 − 0.3611576 − 0.6255432 − 0.65938052 − 0.4170288 − 0.7223151 − 0.45178120.95610173 − 0.362977 − 0.6286946 − 0.25408390.70017884 − 0.58976781.91532721.0566674 − 1.8650096Results of the chi-square test for independence between the stage of buccal caries lesion in the primary incisor and restorative material
For a proximal lesion in the primary incisor (Fig. 4), 31 (67%) respondents stated they would intervene in stage 2 of caries. A significant association was found between the stage of caries lesion in which the dentist would intervene and the dentist's status (p-value = 0.026) (Table 10). Accordingly, pediatric dentistry residents would intervene in a later stage (Table 11).Fig. 4. Case presentation of proximal caries in primary maxillary incisors: a illustration b questionsTable 10Results of the chi-squared test for independence between proximal caries lesion stage in the primary incisor and the study variablesProximal lesion—primary maxillary incisorThe stage of caries lesion in which restoration is necessaryTotalStatistical data1234Preparation techniqueSlicing4103118χ^2^ = 10.195df = 6p-value = 0.116Conventional Class III preparation by G.V Black07007Crown preparation0145221Total4318346The restorative materialOther: slicing + fluoride483116χ^2^ = 9.6588df = 9p-value = 0.378Glass ionomer01001Universal composite resin0205227Flowable composite resin02002Total4318346Expertise statusSpecialist2242129χ^2^ = 14.316df = 6p-value = 0.026Resident235212General practitioner04105Total4318346Table 11Table of residualsThe stage of caries lesion in which proximal restoration is necessarySpecialistResidentGeneral practitioner1 − 0.32855140.9363822 − 0.659380521.0080802 − 1.78881520.34344193 − 1.35520542.0164630.13987574 − 0.64810491.3761249 − 0.5710402Results of the chi-squared test for independence between the stage of proximal caries lesion in primary incisors and dentists' status
Tables 12 and 13 are macro tables that present the stage of intervention depending on the type of lesion. A significant relation was found between the stage of caries lesion in which the dentist would intervene and the type of lesion (p-value < 0.001). For a proximal lesion in the primary molar and a buccal lesion in the primary maxillary incisor, intervention would likely be in the late stage. For an occlusal lesion in a primary molar and a proximal lesion in a primary maxillary incisor, intervention would likely be relatively early.Table 12. Macro tableThe stage of caries lesion in which restoration is necessaryProximal lesion in deciduous molarsOcclusal lesion in deciduous molarsA buccal lesion in deciduous maxillary incisorsProximal lesion in deciduous maxillary incisorsStatistical data11114χ^2^ = 83.552df = 12p-value < 0.00122194313201833842188352000Total46464646Results of the chi-square test for independence between the stage of caries lesion and the type of caries lesionTable 13Residuals table, macro tableThe stage of caries lesion in which restoration is necessaryProximal lesion in deciduous molarsOcclusal lesion in deciduous molarsBuccal lesion in deciduous maxillary incisorsProximal lesion in deciduous maxillary incisors1 − 0.5669467 − 0.5669467 − 0.56694671.70084012 − 3.20713491.3363062 − 2.67261244.543441130.0562544 − 0.39378082.9814829 − 2.643956643.4785054 − 0.6324555 − 0.6324555 − 2.213594452.1213203 − 0.7071068 − 0.7071068 − 0.7071068Results of the chi-square test for independence between the stage of caries lesion and the type of caries lesion
Discussion
Most of the participating dentists stated a preference for a minimal intervention approach, including invasive intervention only at a later stage for patients with a proximal carious lesion in the primary molar. Similarly, Laske et al. (2019) reported that the most common stage for intervention was stage 4. For occlusal lesions in primary molars, the results also collaborate with those of Laske et al.’s (2019), by which stage 3 was the stage most preferred for intervention. However, five (11%) of those who stated they would intervene in stage 2 chose a minimal approach, namely, fissure sealing. This finding illustrates the use of the sealing-in method described by Innes and Manton (2017). We report consensus among our respondents regarding the type of restorative material (flowable composite resin). Flowable composite resin restoration survives very well in shallow Class I lesions (Pinto et al. 2014). It is noteworthy that one participant indicated using a preformed metal crown (Hall Technique) to treat both a stage 4 proximal lesion and a stage 4 occlusal lesion.
Late-invasive intervention was also commonly chosen for buccal lesions in primary incisors, probably after exhausting more conservative and preventive options. The presence of Class V lesions is a main indication for flowable composite resin restorative material. This is mainly due to the mechanical properties of the material and its flow within the cavity, and the excellent level of finish and polish (Baroudi and Rodrigues 2015).
In contrast to the late stage of invasive intervention in the other types of caries lesions, for a proximal carious lesion in primary maxillary incisors, most dentists stated they would intervene invasively relatively early (the second of four stages). Nonetheless, about one-third of the dentists who chose to intervene at this stage chose a slicing type of preparation as a minimal intervention method (Fux-Noy et al. 2023).
The innovation of the current study was the adaptation of the questionnaire for pediatric dentistry. We incorporated specific questions about primary anterior dentition; these lesions are more common in primary than permanent teeth. Early childhood caries refers to caries in the primary teeth of children younger than age 6 years. This caries usually starts in the maxillary primary incisors and is followed sequentially in the first molars, the canines and the second molars, following the eruption pattern of the teeth. Strategies for ECC prevention include reducing Streptococcus mutans transmission from caregivers to infants, restricting dietary sugars, tooth brushing, topical fluoride applications and early dental visits (Seow 2018; AAPD 2022). Use of the developed questionnaire can discern attitudes toward more conservative and disease-specific treatment.
The study had several limitations. These include the low number of participants and the low response rate, of about 30%. However, the expected response to an online questionnaire has been described as 25–30% (Fincham 2008). The questionnaire comprised large images, making it difficult to view on mobile devices. Respondents were thus required to use stationary computer screens, and this may have affected the response rate. In addition, the study was conducted on a specific population of dentists, who were all members of ISDC. It therefore does not necessarily represent pediatric dentistry in Israel. Most ISDC members are specialists and residents, and the sample does not represent general practitioners who treat children but are not ISDC members. Finally, there may be a bias in the results due to non-response. Those who chose not to answer the questionnaire may be more likely not to implement a minimal intervention approach. A limitation of the questionnaire developed by Laske et al. (2019) for MID assessment is that it does not address all MID techniques and stages. Specifically, the questionnaire does not include re-orientation and remineralization stages (Innes and Manton 2017), nor repair methods, such as partial caries removal and the Hall technique.
Conclusions
While the present study has several limitations, it showed that specialists and non-specialists dentists in Israel who treat children tend to use techniques of minimally invasive dentistry. These involve either intervening at a later stage of tooth decay or using conservative methods to remove the caries tissue and restore the tooth. To confirm the results, additional studies on larger samples are needed.