Knowledge and management of Münchausen’s Syndrome by proxy: a survey conducted through the compilation of a questionnaire by pediatricians belonging to the Italian Society of Pediatrics
Rosaria Nardello, Giada Cordova, Corinne La Spina, Ettore Piro, Gregorio Serra, Giovanni Corsello, Antonina Argo

TL;DR
This study explores how well pediatricians in Italy recognize and manage Münchausen Syndrome by Proxy, highlighting gaps in proper reporting and the need for better protocols to protect children.
Contribution
The study provides insights into pediatricians' knowledge and management practices of Münchausen Syndrome by Proxy in Italy.
Findings
Most pediatricians are aware of Münchausen Syndrome by Proxy.
When suspicion is high, doctors often consult with parents or specialists rather than reporting to authorities.
The study emphasizes the need for improved recognition and timely reporting to protect children.
Abstract
Munchausen syndrome by proxy represent forms of abuse with long-term psychiatric outcomes. Since the prevalence of Munchausen Syndrome by proxy is uncertain and underestimated, this study aimed to investigate and analyze the phenomenon through the compilation of an anonymous questionnaire that explores the knowledge of the phenomenon and above all its management. the study was conducted by sending an anonymous questionnaire to pediatricians who are part of the Italian Society of Pediatrics. The questionnaire consists of 18 multiple choice questions and was completed by 511 professionals. The main results highlighted that the majority of doctors knows Münchausen Syndrome by proxy. However, when there is a strong suspicion of the syndrome, they mostly seek discussion with the parent or with another specialist instead of referring to the competent authorities. starting from the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
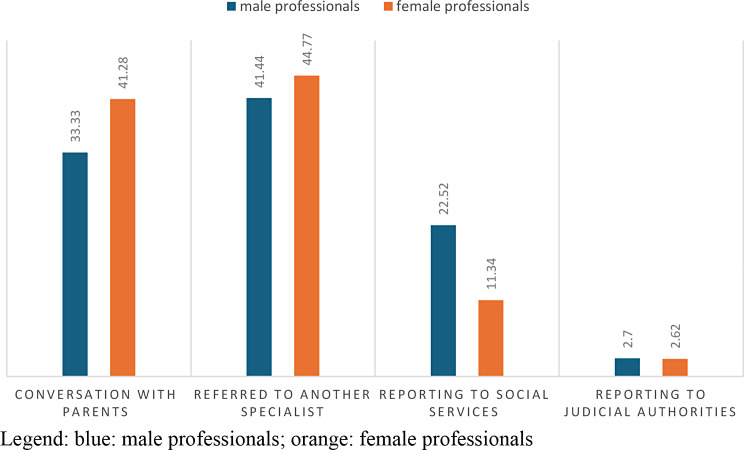 Figure 10
Figure 10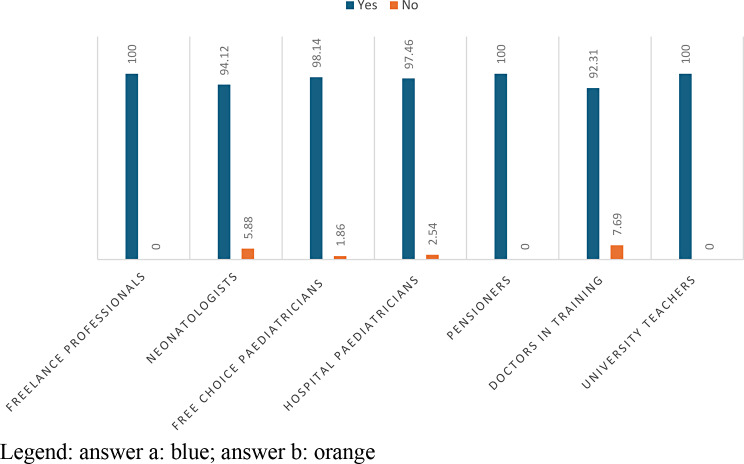 Figure 11
Figure 11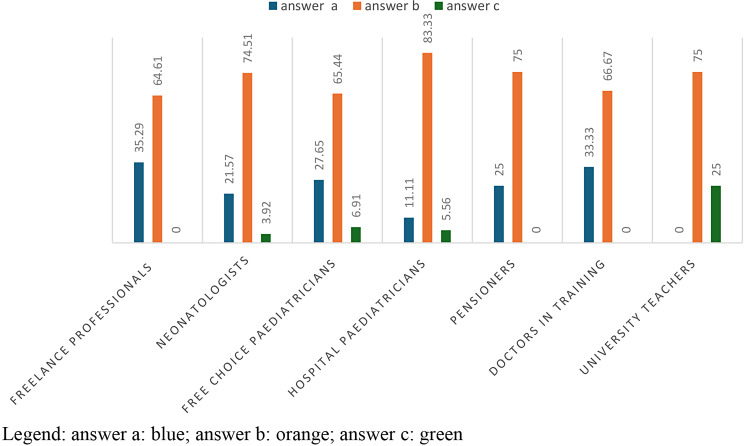 Figure 1
Figure 1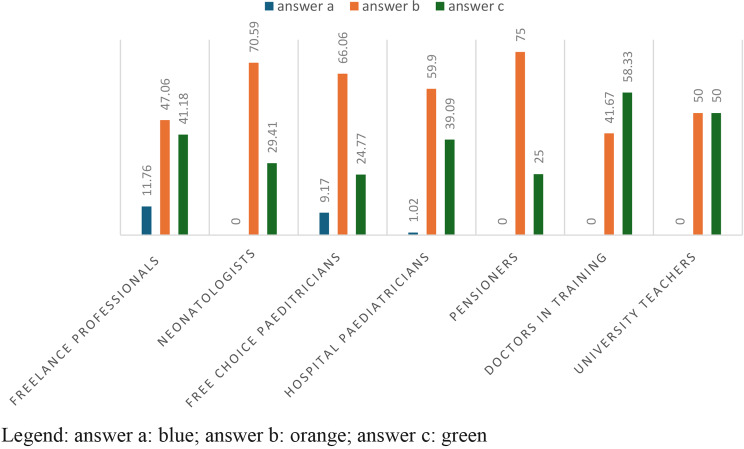 Figure 2
Figure 2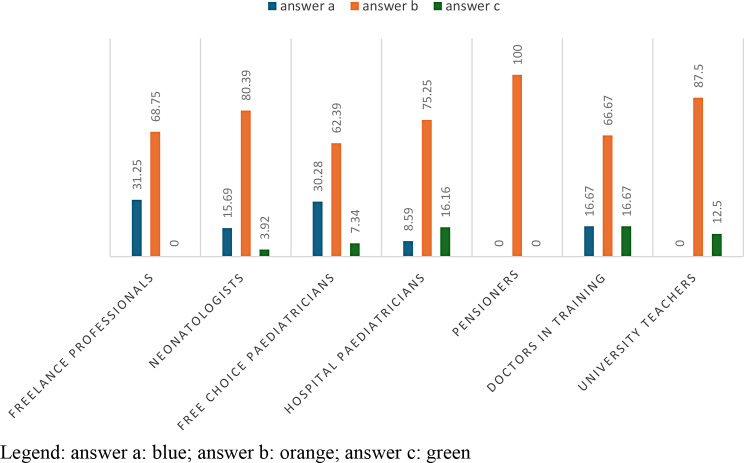 Figure 3
Figure 3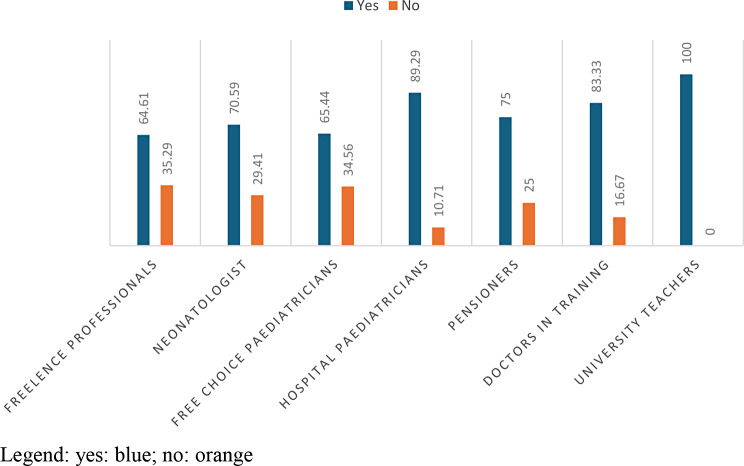 Figure 4
Figure 4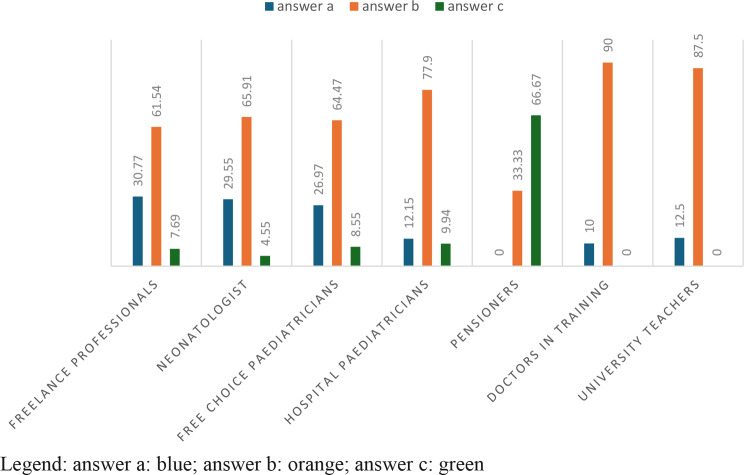 Figure 5
Figure 5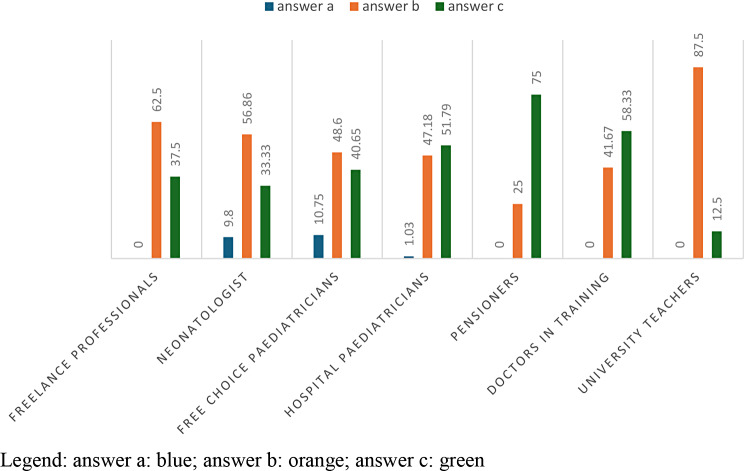 Figure 6
Figure 6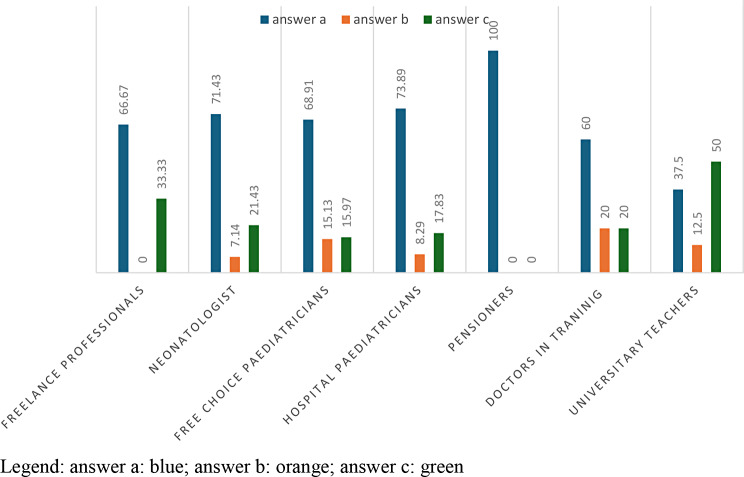 Figure 7
Figure 7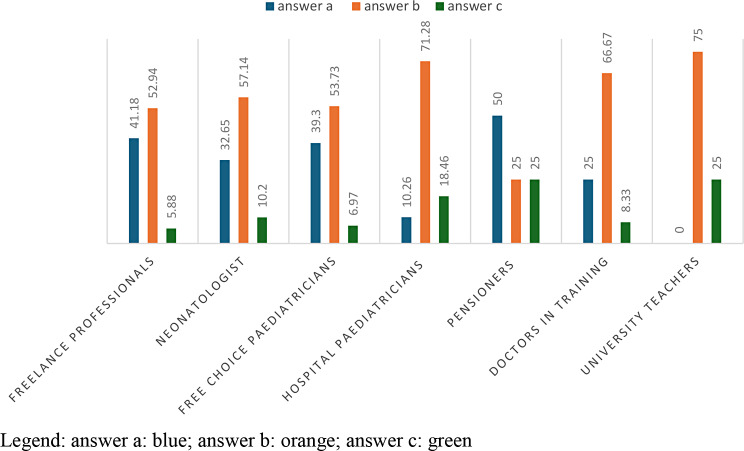 Figure 8
Figure 8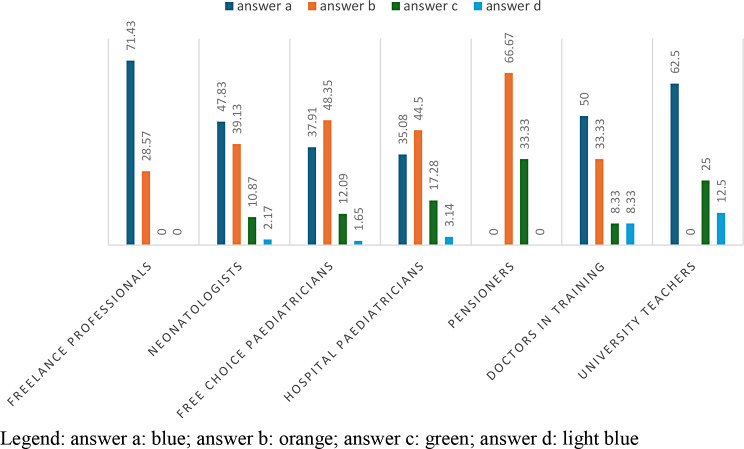 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Abuse and Related Trauma · Child Abuse and Trauma · Healthcare Decision-Making and Restraints
Background
Munchausen syndrome was first described in 1951 by Asher to define individuals who deliberately produce symptoms and signs who tend to seek medical or hospital care [1]. In 1977, Meadow adopted the term “Munchausen Syndrome by Proxy” (MBP) to describe children whose caregivers create histories of illness to their offspring and who support such histories by build physical signs and symptoms, or even by modify laboratory tests [2, 3]. The perpetrator are generally the mothers that are classified into three categories: active inducers, help seekers, and doctor addicts. Active inducers overemphasize the illnesses of their children; help seekers manipulate the children get round problems such as domestic violence and disfatisfied marriage; doctor addicts are overly suspicious [4–6].
MBP can present itself through various clinical cases including a form of systemic lupus erythematosus, induction of coma through the administration of benzodiazepines, catatonia, persistent hyperinsulinemic hypoglycemia, Avoidant Restrictive Food Intake Disorder [7–11]. MBP configures a child abuse. In particular, when considering the victim, the more appropriate term may be “pediatric condition falsification” or “medical child abuse“ [12–15]. The prevalence of MBP is uncertain and underestimated. It seems that there is no prevalence in the sex of the victim, however when the perpetrator is the mother, both sons and daughters are affected. However, when the abuser is the father, male children will be favoured. As regards the average age of diagnosis, this is around 48.6 months. Very young children tend to be affected because they are unable to defend themselves [16]. The incidence is around 0.4/100,000 children aged 2 to 16 years and 2/100,000 children under 12 months [17]. Given that the prevalence is underestimated and the great variability of the symptoms, we believe that pediatricians must know the problem to protect young patients but that they must also have the tools to act on how to behave to protect children. Furthermore, there is not always adequate awareness among health workers of the need to communicate suspected cases to the judicial authorities, and of the method of maintaining any evidence to testify to abuse in Court [14, 15].
For this reason, after having developed a questionnaire intended to explore these areas of interest, we decided to send an anonymous questionnaire to all pediatricians registered with the Italian Society of Paediatrics.
Materials and methods
The identification of the areas of exploration of this research topic, to prepare the questionnaire, was developed by a group of doctors of different specializations (paediatricians, child neuropsychiatrists, forensic doctors, urgencies and emergencies) of Policlinic Hospital, by using an multidisciplinary approach and convergence to selected items. An expert panel of paediatricians at regional level agreed with the questionnaire items, before presenting to Ethic Committee.
The study conducted involved the compilation of an anonymous questionnaire, where the professional must indicate their gender and profession. The questionnaire is made up of 11 questions, some of which are divided into sub-questions, for a total of 18 multiple choice questions.
The questionnaire was sent to the Italian Society of Paediatrics and was completed by 511 professionals divided into: Freelance professionals, Neonatologists, Free choice paediatricians, Hospital paediatricians, Pensioners, Doctors in Training and University Teachers.
The objective of our study was to verify the knowledge of MBP among the first professionals who are in contact with children, i.e. paediatricians, at various ages of development and above all to verify the management of cases in which there is a diagnosis of suspicion and/or a certainty. This study was approved by the ethics committee Palermo 1 of “Paolo Giaccone” University Hospital of Palermo, Italy. (Table 1)
Table 1. Description of the various professional figures who responded to the questionnaireProfessionn°%Freelance professionals173,33Neonatologists5110,00Free choice paediatricians21942,94Hospital paediatricians19838,82Pensioners40,78Doctors in Training132,55University Teachers81,57
Results
- The fact of resorting so frequently to the doctor/first aid was, in your opinion, due to: Excessive parental apprehension; particular severity of the child’s health condition; other causes.
From the analysis of the answers to this question, it was possible to find that 89.35% of the health professionals believed that such frequent recourse to the doctor/first aid was due to excessive parental apprehension. The main health professionals who supported this answer were free choice paediatricians and hospital paediatricians. 12% of the health professionals answered ‘particularly serious health condition of the child’, these were all doctors in training.
- 2.The parent takes the child to the doctor diagnosing diseases that are particularly rare, strange or with symptoms that cannot be detected by clinical investigations: a)never; b)sometimes; c) often.
Table 2. Answers to question number 2abcAnswers10437430%20,4773,625,91Legend: a)never; b)sometimes; c) often
In Table 2, with a p-value = 0,002104, the 73,62% of healthcare professionals ansewered “sometimes”; in particular 74% of neonatologists and 83.3% of hospital paediatrics. The answer ‘never’ is chosen in 35.29% of cases by free-lance paediatricians; the answer ‘often’, on the other hand, is given in 6.91% of cases by free-choice paediatricians. (Table 2; Fig. 1)
Fig. 1answers to question 2 divided according to profession
- 3.The child has already been taken to other doctors, has already undergone numerous clinical examinations, but these have failed to identify the cause of the illness: a)never; b)sometimes; c) often.
Table 3. Answers to question number 3abcAnswers24318166%4,7262,6032,68Legend: a)never; b)sometimes; c) often
In Table 3 with a p-value = 0,0007885, 62.6% of the answers concerned the option “sometimes”, 66% of free choice paediatricians and 59.9% of hospital paediatricians giving this answer. The answer “never” is given more by freelance professionists in 11.76% of cases. University teachers answer 50% “sometimes”, and 50% “often”. (Table 3; Fig. 2)
Fig. 2answers to question 3 divided according to profession
- The child appears to be apparently healthy, but the parents claim that he/she has some kind of illness, proving it with analyses and/or medical records and/or opinions of other doctors: a)never; b) sometimes; c)often.
Table 4. Answers to question number 4abcAnswers9835753%19,2970,2810,43Legend: a)never; b)sometimes; c) often
In Table 4 with a p-value = 6.134e-06, 70.28% is ‘sometimes’, given in 80.39% of cases by neonatologists; in 75.25% of cases by hospital paediatricians and 87.50% of cases by university teachers. The answer “never” is chosen in 31.25% by freelance professionists and in 30.28% by paediatricians of free choice. 8Table 4, Fig. 3)
Fig. 3answers to question 4 C divided according to profession
Had these children been admitted to hospital before? Yes; no.
Table 5. Answers to question number 5YesNoAnswers41197%76,0923,91
The answer “yes” is given in 76.09% of the cases and is given by 89.29% of the hospital paediatricians and 100% of the university paediatricians. The answer ‘no’ is given by 34.56% of free-choice paediatricians and 35.29% of freelancers. Therefore, by carrying out an analysis, the p-value that will emerge will be 1.493e-06. (Table 5; Fig. 4).
Fig. 4answers to question 5 divided according to profession
- 6.If the previous question (4 bis) is answered in the affermative, question 4 ter must also be answered: 4.(ter) If yes, how many? (a) One; (b) From one to five; (c) More than five.
Table 6. Answers to question number 6abcAnswers8229336%19,9571,298,76Legend: answer a: One; answer b: From one to five; answer c: More than five
The 71.29% of the professionals who answered the previous question (4 bis) with “Yes”, claim that the children have previously undergone between one and five hospitalizations.
In question 4 ter with a p-value = 0.001655, it is highlighted that for hospital paediatricians 77.9%, and for specialists with 90%, children have undergone from one to five hospitalizations, while freelancers with 30.77% and paediatricians of free choice with 26.97% instead support the response to (only one hospitalization). This also highlights the differences between intra- and extra-hospital settings. (Table 6; Fig. 5)
Fig. 5answers to the question 4 ter divided according to profession
- 7.The behaviour of these parents during the child’s visits was: normal; particularly anxious; calm, but they recounted in detail the previous examinations, the medical examinations carried out, the hospitalisations undergone by the child.
Table 7. Answers to question number 7abcAnswers30249222%5,9949,7044,31Legend: a: normal; b: anxious; c: quiet
To this question, 49.70% of health professionlas answered: Anxious; 44.31% of health workers answer Quiet.
In Figs. 6 and 62.40% of freelancers, 48.60% of self-employed paediatricians and 87.50% of university teaching provide the answer “Anxious” (answer b). The “quiet” option (answer c) is chosen by 51.79% of hospital paediatricians and by 58.33% of residents. Therefore, analyzing the various answers with a p-value = 0.001444, we will always notice this slight discrepancy between the perception of those who work in a hospital environment and those who do not. (Table 7; Fig. 6)
Fig. 6answers to question 7 divided according to profession
- 8.Among the parents of the type described above,* have you ever discovered lies hidden by them about the child’s health or mystifications such as: Induced provocation of disease symptoms; alteration of analyses and/or medical records; administration of non-prescribed drugs or different doses than prescribed; administration of commonly used substances (e.g. salt*,* water*,* sugar) in exaggerated quantities*,* such that they could still cause harm to the child.*
Table 8. Answers to question number 8abcAnswers2383663%70,6210,6818,69Legend: in 70.62% of cases health professionals answered “symptom provocation”
The answer most frequently given by health professionals in 70.62% of cases is the first one, i.e. symptom provocation. And there are no particular differences between the various categories of professionals. (Table 8; Fig. 7)
Fig. 7answers to question 8 divided according profession
Have you ever observed a worsening of symptoms upon discharge? A) never; b) sometimes; c)often.
Table 9. Answers to question number 9abcAnswers12730060%26,0861,6012,32Legend: A) never; b) sometimes; c)often
In Tables 9, 61.60% of the answers from health professionals are ‘sometimes’, and the majority of answers are given by academics (75%) and hospital paediatricians (71.28%). 41.18% of freelancers and 39.30% of paediatricians of free choice answered ‘never’. (Table 9; Fig. 8)
Fig. 8answers to question 9 divided according to profession
- 10.In the cases described above, what did you do? You have asked for an interview with the parents; you have referred the parents to a specialised colleague (psychiatrist, psychologist); you have reported the situation to the social services; you have reported the case to the judicial authorities.
Table 10. Answers to question number 10abcdAnswers1802016412%39,3943,98142,63Legend: answer a: You have asked for an interview with the parents; answer b: you have referred the parents to a specialised colleague (psychiatrist, psychologist); answer c: you have reported the situation to the social services; answer d: you have reported the case to the judicial authorities
43% of health professionals answered ‘you have referred the parents to a specialised colleague (psychiatrist, psychologist)’; 39.39% of health professionals answered ‘you have asked for an interview with the parents’; 14% of health professionals answered ‘you have reported the situation to the social services’ and finally 2.63% of health professionals answered ‘you have reported the case to the judicial authority’.
- 71.43% of the freelancers requested an interview with the parents and in no case reported the case to the judicial authority or social services.
- 48.35% of free-choice paediatricians requested an interview with medical specialists (psychiatrist, psychologist); 37.91% of free-choice paediatricians requested an interview with parents; 12.09% of free-choice paediatricians proceeded to report the case to the social services and only 1.65% of free-choice paediatricians reported the case to the judicial authorities.
- 44.50% of hospital paediatricians request an interview with medical specialists; 35.08% of hospital paediatricians request an interview with parents; 17.28% proceed to report the case to the social services and 3.14% of hospital paediatricians report the case to the judicial authorities. (Table 10; Fig. 9).
Fig. 9answers to question 10 divided according to profession
Analyzing the difference between male professionals and female professionals: with a p-value = 0.02896, we will notice a discrepancy in the type of attitude implemented, the professional women will tend more to interview the parents in 41.28% of cases, the specialist male will instead tend to report more to the social services with a 22.52%.
Have you ever heard of Munchausen syndrome by proxy? Yes; no.
Table 11. Answers to question number 11abAnswers49213%973Legend: answer a: yes; answer b: no
This result evidences that only 3% of professionists never heard to speak the term “Munchausen Syndrome”.
Analyzing the details of results of question number 11 we observe that 97.43% of health professionals answered in the affermative and 2.57% answered negatively. The 98.14% of free-choice paediatricians and 97.46% of hospital paediatricians answered in the affermative. Most neonatologists (5.88%) and doctor in training (7.69%) are not aware of Munchausen’s syndrome. (Table 11; Fig. 10).
Fig. 10answers to question 11 divided according to professional profiles
Discussion
Munchausen Syndrome by Proxy (MSBP) poses significant challenges to healthcare professionals due to its elusive nature and potential harm to victims. Despite its recognition for many years, the medical literature lacks consistent studies on its epidemiology, therapeutic approaches, and prognosis. This article aims to shed light on the critical importance of early diagnosis, effective management, and appropriate reporting to protect the welfare of those affected by MSBP.
The study conducted underlines that there are some discrepancies in response between the various professions, especially sectoral between those who work in hospitals and those who do not. Example, in question 4 A we notice a discrepancy between the answers and the perceptions that freelancers and hospital paediatricians have. Most doctors know Münchausen Syndrome by proxy. Finally, when there is a strong suspicion of the syndrome, however, in most cases a discussion is sought with the parent or with the specialist instead of referring to the competent authorities.
Recognizing and diagnosing MSBP in a clinical setting is fundamental for preventing further abuse and minimizing unnecessary medical or surgical interventions. When a case of MSBP is suspected, medical professionals must prioritize arriving at a clinical diagnosis. A comprehensive clinical examination of the child and an in-depth analysis of the family’s psycho-social relationship should be thoroughly conducted and documented. Healthcare professionals face complex ethical dilemmas in managing cases of MSBP. Balancing the child’s best interest with the principle of substituted judgment adds to the intricacy of decision-making. In such situations, doctors are called upon to collaborate with other professionals and law enforcement representatives when necessary, adhering to the Italian Deontological Medical Code (Article 32) to ensure total care of the vulnerable person.
From the results obtained from the administered questionnaire, it emerged that only 2% of pediatric professionals turned to the competent judicial authority through a mandatory report. This data requires many reflections. (Table 10; Figs. 9 and 11)
Fig. 11answers to question 10 divided according to gender
Prompt reporting of known or suspected cases of child abuse and neglect is a legal and ethical obligation for medical professionals [18–20]. Reporting duties have been enacted in child protection legislation in some jurisdictions, while organizational policies govern reporting in others. Training interventions should be employed to equip professionals with the knowledge, awareness, and attitudes required for effective reporting. Well-trained interdisciplinary child protection teams, using an evidence-based approach, play a crucial role in accurately identifying cases of maltreatment and making decisions that positively impact the well-being of affected children. Public policies, such as mandatory reporting laws, contribute to tertiary prevention interventions aimed at safeguarding maltreated children [21–25].
A very recent study published in the journal Child Abuse & Neglect highlighted through the description of a group of patients aged between 10 and 18 that the victims had had a major impact on the quality of their lives with a high rate of school dropout (96%). The average delay to the suspected diagnosis was 5.8 (2.6–9) years and, even when recognised, Munchausen syndrome by proxy was rarely the subject of social or judicial reporting (only in 42% of adolescents) [26].
It is important to highlight the limitations of this study; firstly, the answers in fact refer to a relatively limited number of paediatricians; furthermore, a training course was not implemented following the administration of the questionnaire, on the areas of uncertainty and lack of knowledge of health care professionals; however, the interest of this subject and duties related both to patients and referral to law authorities encourage to improve the guidelines and protocols to be applied in “ad hoc” hospital care pathways for suspected case of MBP.
Conclusions
We emphasize the urgency of enhancing the recognition and management of Munchausen Syndrome by Proxy. Early diagnosis, appropriate reporting, and collaboration with child protection authorities are essential in safeguarding the well-being of vulnerable individuals. Emphasizing the role of interdisciplinary teams and implementing evidence-based interventions is crucial for protecting the most marginalized members of society—maltreated children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sousa Filho D, Kanomata EY, Feldman RJ, et al. Munchausen syndrome and Munchausen syndrome by proxy: a narrative review. Einstein (Sao Paulo). 2017 Oct-Dec;15(4):516–21.10.1590/S 1679-45082017 MD 3746 PMC 587517329364370 · doi ↗ · pubmed ↗
- 2Unal EO, Unal V, Gul A et al. A serial Munchausen Syndrome by Proxy. Indian J Psychol Med 2017 Sep-Oct; 39(5):671–4.10.4103/0253-7176.217017 PMC 568889929200568 · doi ↗ · pubmed ↗
- 3Sheridan MS. The deceitcontinues: An updated literature review of Munchausen Syndrome by Proxy, in Child Abuse and Neglect, Apr. 2003, vol. 27, no. 4, pp. 431–451. 10.1016/S 0145-2134(03)00030-910.1016/s 0145-2134(03)00030-912686328 · doi ↗ · pubmed ↗