Unintentional Levothyroxine Ingestion by a Child: A Case Report
Dinesh V Hinge, Mukund Raizada, Shantanu Gomase, Swati Khapekar, Chaitanya Kumar Javvaji

TL;DR
A three-year-old child accidentally ingested levothyroxine and developed symptoms like tachycardia and high blood pressure, but recovered after treatment.
Contribution
This case report highlights the delayed onset of symptoms after levothyroxine ingestion in a child.
Findings
The child was asymptomatic initially but developed tachycardia and high blood pressure 24 hours after ingestion.
Treatment with propranolol and prednisolone led to recovery and normal thyroid function after one month.
The case emphasizes the need for monitoring even asymptomatic children after accidental ingestion.
Abstract
Hypothyroidism is a common endocrine condition in the adult and pediatric population. Levothyroxine, used for the treatment of hypothyroidism, is one of the easily available drugs in any household as either parents or sometimes children are on levothyroxine treatment. Accidental levothyroxine ingestion is increasing nowadays. Unintentional thyroxine ingestion in children may follow diverse manifestations, ranging from asymptomatic presentation to thyrotoxic crisis. While asymptomatic children can be monitored at home, children with severe symptoms need intensive care support. A child can develop convulsions, temperature instability, and arrhythmias, among others. Here, we present the case of a three-year-old male child with a history of accidental ingestion of 3.2 mg levothyroxine. He was initially asymptomatic and developed symptoms such as tachycardia and high blood pressure after 24…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
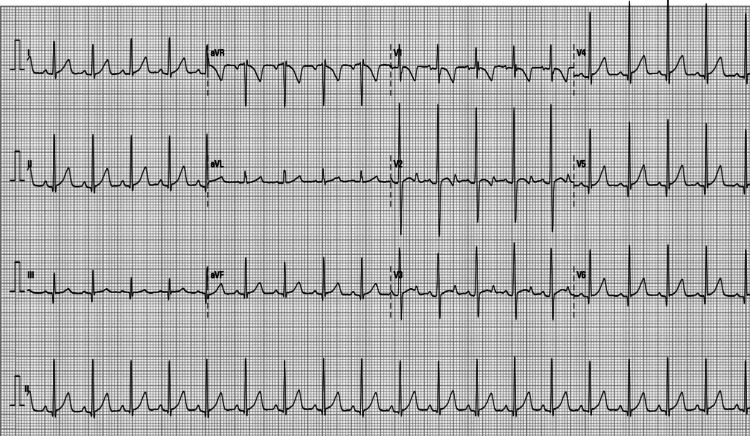 Figure 1
Figure 1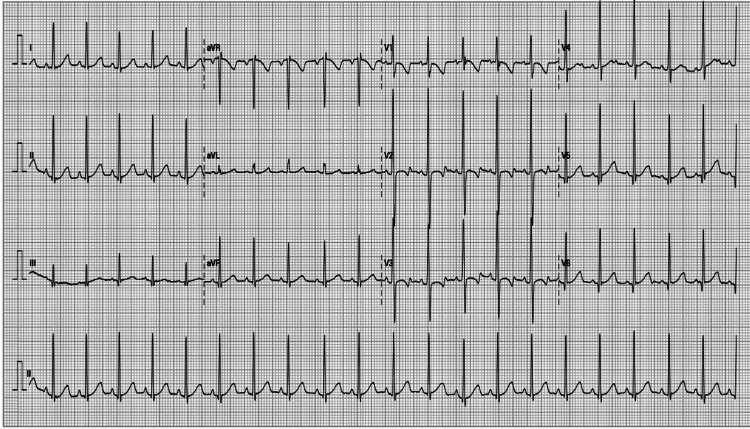 Figure 2
Figure 2| Thyroid parameter | Normal range for 3 years | After 4 hours (on admission) | After 24 hours | After 48 hours | After 72 hours | After 7 days | After 30 days |
| Total T3(ng/dL) | 105–269 | 171 | 310 | 250 | 178 | 180 | 170 |
| Total T4 (µg/dL) | 5.9–13.9 | >30 | >30 | >30 | 25.1 | 12.8 | 10 |
| TSH (mIU/L) | 0.70–5.97 | 1.483 | 0.093 | 0.039 | 0.034 | 0.1 | 1.2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Poisoning and overdose treatments · Restraint-Related Deaths
Introduction
Accidental drug ingestion is a common cause of morbidity and mortality in the pediatric age group. Common medication intoxications are reported to be due to paracetamol, antibiotics, and antidepressants, among others. Levothyroxine poisoning in children is rare but worrisome for treating doctors and caretakers. The toxic dose of levothyroxine in pediatric age groups is 3 mg/day [1]. Clinical manifestation is variable and is independent of the ingested levothyroxine dose [2]. As few pediatric cases of levothyroxine intoxication are published in the literature, limited information is available on its clinical manifestation and management [3]. Accidental ingestion of high-dose levothyroxine may remain asymptomatic or may present with symptoms such as fever, insomnia, irritability, tremors, tachycardia, hypertension, and convulsions [4]. Sometimes, it can lead to life-threatening complications such as arrhythmias, seizures, thyrotoxic storms, and coma [5]. Treatment of levothyroxine intoxication mainly depends on clinical manifestations in patients and needs close clinical monitoring supported by serial laboratory investigations to look for complications. Treatment options include gastric decontamination, propranolol, steroids, benzodiazepines, and antiepileptic drugs such as phenobarbital, depending on the clinical presentation. One may consider the use of propylthiouracil and occasionally plasmapheresis to remove excess levothyroxine in cases of severe life-threatening symptoms [6]. Here, we present the case of a three-year-old boy with unintentional levothyroxine ingestion (3.2 mg). He was documented to have tachycardia and high blood pressure and was managed successfully with gastric decontamination, steroids, and propranolol.
Case presentation
A three-year-old male child was admitted with a presumed history of accidental ingestion of levothyroxine tablets from his father’s medication box. His father was on levothyroxine 100 µg tablet once daily for hypothyroidism. An ingested dose of levothyroxine (3.2 mg) was calculated from the missing tablets in the container. He had ingested around 32 tablets of Thyronorm (100 µg) four hours before presentation to the hospital and was asymptomatic on presentation. The parents denied any vomiting, fever, pain in the abdomen, convulsions, or palpitations. The child was born full-term with a birth weight of 2.8 kg and had an uneventful perinatal period. His development was appropriate for his age in all domains. There was no significant past medical and surgical history. On presentation, he was afebrile (98.3°F), his heart rate (HR) was 110 beats/minute, with a normal respiratory rate (RR) (22/minute), normal blood pressure (BP) (94/68 mmHg), and saturating 98% on room air. His systemic examination, including cardiovascular and neurological examination, was within normal limits. After admission to the hospital, gastric lavage with normal saline was performed. His baseline investigations performed on hospitalization included a complete blood count, liver function test, renal function test, thyroid function test (TFT), lactate dehydrogenase (LDH), and creatine kinase-myoglobin binding (CKMB) which were within normal limits. An electrocardiogram (ECG) done on admission was documented as normal (Figure 1).
Electrocardiogram on admission to the hospital.
An ECG repeated after 24 hours of admission to look for arrhythmias revealed sinus tachycardia and age-appropriate changes (Figure 2).
Electrocardiogram changes after 24 hours of levothyroxine ingestion.
His TFT was done on admission and monitored serially, as shown in Table 1.
On admission, his T4 level was high, which was consistent with the history of levothyroxine ingestion. After 24 hours of admission, he developed tachycardia and higher blood pressure (>95th centile for age), and his TFT revealed raised T3, T4, and decreased thyroid-stimulating hormone. We commenced oral propranolol (2 mg/kg/day) and prednisolone (2 mg/kg/day). His HR and BP stabilized after three days. His HR, temperature, RR, BP, blood sugar, and weight were monitored during his hospital stay. All vital parameters, ECG, and blood sugar remained within the normal range for his age after commencing propranolol and prednisolone. The child was discharged on the fifth day of ingestion as T4 and T3 levels on day 4 showed a decreasing trend, and his HR and BP remained normal. He was discharged with safety advice to his parents and with a plan for clinical review and repeated TFT after two days (day 7 of ingestion) and 30 days.
Discussion
Thyrotoxicosis is an excess of circulating thyroid hormone that causes symptomatic overactivity with an increased metabolic rate [5]. The common causes of thyrotoxicosis include Graves’ disease, thyroiditis, multinodular goiter, and exogenous levothyroxine hormones. In our case, the cause of thyrotoxicosis was accidental ingestion of levothyroxine tablets. Overdose due to accidental ingestion is quite common in children. In adults, the overdose is extremely rare and can be intentional due to mental health issues [7]. Levothyroxine overdose may manifest with symptoms such as fever, increased sweating, flushing, tremors, loose stools, vomiting, convulsions, hypertension, and irregular heart rate [8]. Golightly et al. published a study of 41 children aged one to five years. Overdose of levothyroxine in children generally causes mild or no symptoms. Mild symptoms such as gastric upset, fever, tachycardia, and hyperactive behavior resolve within two weeks without treatment [3]. In a case report, a 2.5-year-old child developed fever, agitation, irritability, increased thirst, tachycardia, and hypertension after ingestion of a massive dose of levothyroxine (10.5 mg). He also developed delayed symptoms such as hair loss and desquamation of the palms and soles after 10 days which were managed symptomatically [7]. In another case report, a 21-year-old female developed transient loss of consciousness and atrial fibrillation after ingesting 10 mg of levothyroxine and was treated with propylthiouracil, steroids, and hemoperfusion to increase levothyroxine clearance. She recovered well and was discharged without any long-term sequel [6]. The onset or severity of symptoms is independent of the dosage of levothyroxine consumed and does not correlate with plasma thyroxin levels. Symptoms may last up to 6 to 11 days [7].
Conclusions
Children have easy access to levothyroxine tablets at home as they, or adults, may take them regularly as medication. It has a good color, smell, and taste which makes it attractive to children. If a child takes levothyroxine as prescribed medication, it should be given by a caretaker or directly supervised if the child is relatively older and self-administering it. Children should be taken to the hospital urgently if there is a suspicion of accidental ingestion. Children need hospitalization for clinical and laboratory monitoring for signs of toxicity and hyperthyroidism. Parents should be vigilant and should keep all medications out of reach of children to avoid accidental ingestion and intoxication, as consequences can be grave, with significant morbidity and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Levothyroxine poisoning in children - should we really be afraid?Anatolian Clin Ozturk B Bodur I Tekeli A 247251282023 https://doi.org/10.21673/anadoluklin.1240784
- 2Clinical toxicity of acute overdoses with L-thyroxin in children Pediatr Emerg Care Ergul AB Altuner Torun Y Serbetci MC Ozcan A Bas VN 7877903520192841902110.1097/PEC.0000000000001141 · doi ↗ · pubmed ↗
- 3Clinical effects of accidental levothyroxine ingestion in children Am J Dis Child Golightly LK Smolinske SC Kulig KW Wruk KM Gelman CJ Rumack BH Linden CH 102510271411987288710610.1001/archpedi.1987.04460090102039 · doi ↗ · pubmed ↗
- 4Accidental levothyroxine ingestion in children: review of four cases Thyroid Res Pract Ma Maddukuri HR Kalra P Karunakara BP Venugopal P 146148172020
- 5Thyrotoxicosis after a massive levothyroxine ingestion: a case report World J Clin Cases Du F Liu SW Yang H Duan RX Ren WX 362436291020223561121010.12998/wjcc.v 10.i 11.3624 PMC 9048560 · doi ↗ · pubmed ↗
- 6No obvious sympathetic excitation after massive levothyroxine overdose: a case report Medicine (Baltimore) Xue J Zhang L Qin Z 097201810.1097/MD.0000000000010909 PMC 599951329879029 · doi ↗ · pubmed ↗
- 7Massive levothyroxine ingestion in a pediatric patient: case report and discussion CJEM Ho J Jackson R Johnson D 1651681320112152437310.2310/8000.2011.110361 · doi ↗ · pubmed ↗
- 8Massive levothyroxine ingestion Indian Pediatr Pai G Jain V 840841512014 https://www.indianpediatrics.net/oct 2014/840-841.pdf 25362025 · pubmed ↗