The Effects of Pangenotypic Direct-Acting Antiviral Therapy on Lipid Profiles and Insulin Resistance in Chronic Hepatitis C Patients
Meng-Yu Ko, Yu-Chung Hsu, Hsu-Heng Yen, Siou-Ping Huang, Pei-Yuan Su

TL;DR
This study shows that pangenotypic DAA treatments for hepatitis C significantly raise LDL and TC levels but do not affect insulin resistance.
Contribution
The study compares the metabolic effects of two pangenotypic DAA regimens in chronic HCV patients.
Findings
Both GLE/PIB and SOF/VEL regimens significantly increased LDL and TC levels after treatment.
No significant changes were observed in triglycerides, HDL, HbA1C, or insulin resistance.
Baseline LDL/TC and glucose levels predict the degree of lipid increase after treatment.
Abstract
Hepatitis C virus (HCV) eradication is usually associated with dyslipidemia. Most studies in this field have focused on genotype-specific direct-acting antivirals (DAAs), with research on pangenotypic DAAs being limited. This study examined how two pangenotypic DAA regimens, glecaprevir/pibrentasvir (GLE/PIB) and sofosbuvir/velpatasvir (SOF/VEL), affect lipid profiles and insulin resistance after viral eradication in chronic HCV patients. A total of 100 patients (57 with GLE/PIB and 43 with SOF/VEL) treated between September 2020 and January 2022 were included in the retrospective analysis. This study found a significant increase in LDL and TC levels after treatment (p < 0.001), but no significant changes in triglycerides, high-density lipoprotein, HbA1C, or the Homeostatic Model Assessment of Insulin Resistance. According to a logistic regression analysis, higher baseline LDL or TC and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
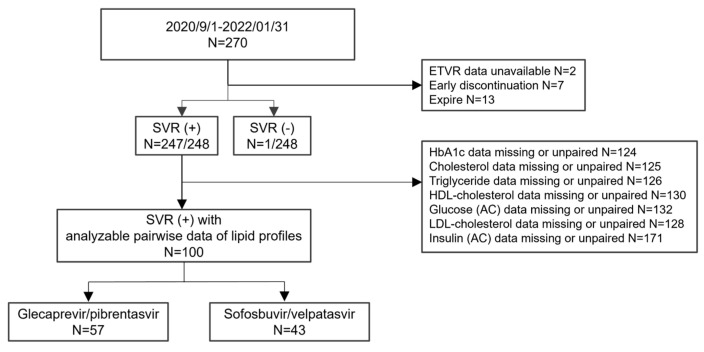 Figure 1
Figure 1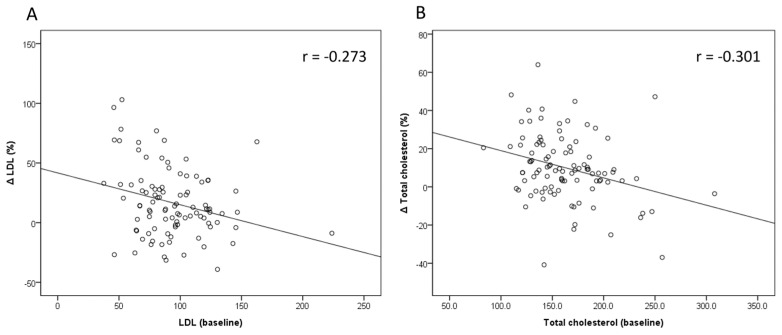 Figure 2
Figure 2- —Changhua Christian Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · Liver Disease Diagnosis and Treatment · Diabetes and associated disorders
1. Introduction
Hepatitis C virus (HCV) infection can cause chronic hepatitis, cirrhosis, and hepatocellular carcinoma (HCC), affecting approximately 50 million people worldwide. This infection is a major public health concern, putting a heavy disease burden on both individuals and healthcare systems [1]. HCV infection is frequently asymptomatic and progresses to a chronic condition in most patients, with diagnosis usually occurring only after the disease has advanced to more severe stages of fibrosis.
The treatment of chronic HCV infection has dramatically improved with the introduction of new direct-acting antivirals (DAAs). These DAAs have higher efficacy across all genotypes and fewer side effects than previous interferon (IFN)-based therapies. While HCV eradication significantly reduces the risk of cirrhosis and HCC, patients with advanced liver fibrosis or cirrhosis must continue to undergo regular HCC screenings even after achieving a sustained virologic response (SVR) [2,3].
Several studies have found that HCV infection causes metabolic changes such as insulin resistance (IR), metabolic syndrome, and diabetes via complex pathways [4,5]. Chronic HCV infections have been linked to hepatic steatosis and dyslipidemia [6]. According to research, eradicating HCV can improve fasting glucose, HbA1C, and IR [7]. Furthermore, studies have reported varying effects on lipid profiles: some found a decrease in total cholesterol (TC) and low-density lipoprotein (LDL) levels with an increase in triglycerides (TG) during treatment, while others found an increase in LDL and TC levels post treatment but no significant changes in TG levels [8].
Most studies exploring the effect of lipid homeostasis and IR following viral eradication have focused on genotype-specific DAAs, particularly between subgroups treated with sofosbuvir (SOF)-based versus non-SOF-based DAAs [9,10]. However, limited research has investigated the impact of lipid profiles after treatment with new pangenotypic DAAs. This study aimed to evaluate the impact of viral eradication on lipid levels and IR in HCV patients after receiving pangenotypic DAA antiviral therapy.
2. Materials and Methods
We retrospectively included patients with chronic HCV infection who received DAA therapy between September 2020 and January 2022 at Changhua Christian Hospital in Taiwan. All patients had routine outpatient follow-ups during the treatment and none were discontinued due to adverse events. Exclusion criteria included the following: (1) patients who did not complete the lipid profile or had insufficient clinical data before and after DAA therapy; and (2) incomplete DAA therapy or a lack of sustained virological response 12 weeks after treatment. The DAA regimens consisted of glecaprevir/pibrentasvir (GLE/PIB) and sofosbuvir/velpatasvir (SOF/VEL). (Figure 1).
Lipid profiles measured TC, LDL, and TG. HCV genotyping was performed on all patients. A complete blood count was taken, liver function tests were conducted, and HCV RNA levels were measured before and 12 weeks after treatment. The current study was authorized by the institutional review board (IRB No. 231011), and informed consent was waived due to the anonymization of all data.
Liver elastography, steatosis, lipid profile, fasting glucose, and insulin levels were measured before and 12 weeks after DAA therapy. The degree of liver fibrosis was determined using FibroScan^®^ 530 compact (Echosens, Franceand) and the FIB-4 index, which was calculated from indirect serum markers. Advanced fibrosis was defined as an FIB-4 score above 3.25 [11]. Liver stiffness and steatosis were determined via transient elastography, with a measurement range of 2.5 kPa to 75 kPa, and the controlled attenuation parameter (CAP), which ranges from 100 to 400 decibels per meter (dB/m), with the FibroScan^®^ compact 530 (Echosens, Paris, France). Insulin resistance was assessed using the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), which is calculated as (fasting glucose level × fasting serum insulin level)/405 [12]. The percentage change in LDL and TC was calculated by subtracting the pretreatment value from the post-treatment value and dividing by the pretreatment value.
Statistical Analysis
Demographic and other clinical data for continuous variables are given as mean ± standard deviation, while categorical variables are given as numbers and percentages. Baseline data comparisons between the GLE/PIB and SOF/VEL groups were made using the Chi-square test or Fisher’s exact test for categorical variables, and Student’s t-test for continuous variables. The paired samples t-test was used to compare the mean values of continuous data at two different time points: baseline (T0) and 12 weeks after the completion of DAA therapy (SVR). Pearson’s correlation coefficient was used for correlation analysis. Logistic regression models were used in both univariate and multivariate analyses. Factors that were significantly associated in univariate analyses were included in the multivariate model through backward elimination. All statistical analyses were carried out using PASW Statistics version 18 (formerly SPSS; IBM, Hong Kong). A p-value below 0.05 was deemed statistically significant.
3. Results
3.1. Baseline Characteristics of Total and Subgroup Patients
Our study included 100 patients: 57 treated with GLE/PIB and 43 treated with SOF/VEL. Table 1 shows the baseline characteristics in detail. Of the 100 patients, 50 (50%) were male, with an average age of 58.6 ± 12.7 years. The majority of patients (49%) had genotype 2 HCV. The average HCV RNA level was 5.53 ± 1.2 log10 IU/mL. Additionally, 36 patients (36%) had hypertension, 12 (12%) had diabetes mellitus, and 12 (12%) had cancer, including oral cancer (n = 3), colon cancer (n = 3), breast cancer (n = 2), lung cancer (n = 2), hepatoma (n = 1), and lymphoma (n = 1). Nineteen patients (19%) had an FIB-4 score ≥ 3.25. When comparing the two subgroups (GLE/PIB and SOF/VEL), the SOF/VEL group had a higher proportion of males, higher Aspartate Transaminase (AST) levels, lower LDL and TC levels, and greater liver stiffness.
3.2. Results Before and After DAA Treatment of the Total Patients
The laboratory tests and elastography results for the 100 patients before and after HCV treatment are shown in Table 2. Liver stiffness and FIB-4 scores significantly decreased (p < 0.001), whereas CAP increased after DAA therapy (p = 0.007). After treatment, LDL and TC levels were significantly higher than before (p < 0.001). There were no significant differences in fasting glucose, insulin, HOMA-IR, HbA1c, or HDL before and after treatment. The TG level was slightly higher after treatment than before, but the difference was not statistically significant (p = 0.088).
3.3. Results Before and After DAA Treatment for Subgroups of Two Pangenotypic DAAs
Table 3 shows the analysis of the two subgroups, separated by their DAA regimens: 57 patients received glecaprevir/pibrentasvir (GLE/PIB), while 43 received sofosbuvir/velpatasvir (SOF/VEL). TC and LDL levels were significantly higher after treatment in both subgroups than before treatment, with the GLE/PIB group showing a more pronounced increase. While liver stiffness measurements significantly decreased in both groups following treatment, the controlled CAP only increased in the GLE/PIB group.
3.4. Factors Associated with the Change in LDL and TC in Entire Population
Only pretreatment fasting glucose and LDL were found to be negatively associated with the percentage change in LDL after treatment in both univariate and multivariate analyses (p = 0.005 and p = 0.007, respectively). (Table 4) The findings were similar for TC, with pretreatment fasting glucose and TC being negatively associated with the percentage change in total cholesterol after treatment in both univariate and multivariate analyses (p = 0.001 and p = 0.009, respectively) (Table 5). Figure 2 shows a negative correlation between baseline LDL and the percentage change in LDL (r = −0.273), as well as between baseline TC and the percentage change in TC (r = −0.301).
4. Discussion
This is the first study to look at the effects of two different pangenotypic DAA regimens, GLE/PIB and SOF/VEL, on lipid profiles and IR. Our results show that LDL and TC levels were increased after viral eradication by two pangenotypic DAAs, but there were no significant changes in fasting glucose, HbA1c, HOMA-IR, TG, or HDL.
HCV can increase lipid biosynthesis and lower the export of apolipoproteins via multiple mechanisms of lipid metabolism. This phenomenon is reversed after HCV is eradicated using DAAs [13]. There is some debate about which lipid profiles are affected by HCV infection. Most studies show that LDL and TC are the most commonly affected lipids following HCV eradication [6,7,8]. However, some studies show that HCV eradication by DAA therapy lowers triglycerides and raises HDL levels [14,15]. Our study found that LDL and TC levels increased after HCV eradication, which is consistent with most previous studies. Furthermore, the effects of various DAA regimens on lipid profiles have yielded inconsistent results. Inoue Takako et al. and Endo Daisuke et al. found that patients treated with sofosbuvir plus ledipasvir had higher LDL and TC levels than those treated with daclatasvir plus asunaprevir [10,16]. A review by YW Wang et al. discovered that SOF-based DAAs cause more significant increases in LDL than non-SOF-based DAAs [17]. However, our findings indicated that SOF-based (SOF/VEL) and non-SOF-based (GLE/PIB) DAAs have similar effects on lipid profiles after viral eradication. LDL and TC levels significantly increased following DAA therapy, while TG and HDL levels remained unchanged. This could be explained by the strong and comparable efficacy of both pangenotypic DAAs in eliminating HCV, resulting in similar effects on lipid profiles.
Several factors have been linked to increased levels of LDL and TC [7]. These include the absence of cirrhosis, hyperlipidemia, and a larger baseline waist circumference [18]. Additionally, higher HOMA-IR, lower AST, higher triglycerides, and a higher BMI at baseline were linked to changes in LDL levels [15,16]. In our study, the predictors of the degree of change in LDL and TC included fasting glucose and baseline LDL and TC levels. These findings are consistent with those of previous research, but more studies are needed to confirm them.
Previous research has shown that IR is closely associated with chronic hepatitis C infection, particularly in genotypes 1 and 4 [5]. DAA therapy can reverse IR in patients with chronic hepatitis C infection and improve hyperglycemia [19]. One mechanism linking HCV and IR is that the HCV core protein induces serine phosphorylation of the insulin receptor substrate protein. This process inhibits phosphatidylinositol-4,5-bisphosphate 3-kinase signaling, which is followed by a decrease in protein kinase B and tuberous sclerosis complex 1/2 signaling [20,21]. Our study found no significant difference in fasting glucose, HbA1C, or HOMA-IR levels between baseline and post-treatment. However, there was a trend of mild decreases in HbA1C and HOMA-IR following DAA treatment. One possible explanation is that our study’s baseline levels of fasting glucose, HbA1C, and HOMA-IR were lower than those in other studies, resulting in no significant differences [19,22].
This study has several limitations. First, the sample size was small because we only included patients who had complete data on fasting glucose, insulin, HbA1C, and lipid profiles before and after DAA treatment. Because this was a real-world retrospective study, less than half of the patients who were initially included were analyzed. Consequently, some older patients or those with multiple comorbidities were excluded, which could explain why some parameters showed no significant differences. Second, the follow-up period in our study was brief. Researchers discovered that LDL and TC levels remained elevated even two years after DAA therapy. However, most studies observed a reduction in carotid atherosclerosis after HCV eradication [7]. In addition, previous studies have shown that HCV infection can increase the risk of cardiovascular disease, while antiviral therapy can lower this risk [23,24]. The possible mechanism is multifactorial, involving lipid disturbances, vascular injury, oxidative stress, and endothelial dysfunction. Therefore, more research is needed to understand the long-term impact of pangenotypic DAAs and their influence on clinical outcomes.
5. Conclusions
Treatment with the two pangenotypic DAAs increased LDL and TC levels. Our study found no significant differences in glucose, HbA1c, HOMA-IR, or TG levels before or after DAA therapy. The only significant predictors of an increase in LDL or TC levels at SVR12 were lower baseline fasting glucose and lower LDL or TC levels.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Hepatitis Report 2024: Action for Access in Low- and Middle-Income Countries World Health Organization Geneva, Switzerland 2024
- 2Morgan T.R. Ghany M.G. Kim H.Y. Snow K.K. Shiffman M.L. De Santo J.L. Lee W.M. Di Bisceglie A.M. Bonkovsky H.L. Dienstag J.L. Outcome of sustained virological responders with histologically advanced chronic hepatitis C Hepatology 20105283384410.1002/hep.2374420564351 PMC 2932862 · doi ↗ · pubmed ↗
- 3Morgan R.L. Baack B. Smith B.D. Yartel A. Pitasi M. Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: A meta-analysis of observational studies Ann. Intern. Med.201315832933710.7326/0003-4819-158-5-201303050-0000523460056 · doi ↗ · pubmed ↗
- 4Huang J.F. Yu M.L. Dai C.Y. Hsieh M.Y. Hwang S.J. Hsiao P.J. Lee L.P. Lin Z.Y. Chen S.C. Hsieh M.Y. Reappraisal of the characteristics of glucose abnormalities in patients with chronic hepatitis C infection Am. J. Gastroenterol.20081031933194010.1111/j.1572-0241.2008.01996.x 18637090 · doi ↗ · pubmed ↗
- 5Moucari R. Asselah T. Cazals-Hatem D. Voitot H. Boyer N. Ripault M.P. Sobesky R. Martinot-Peignoux M. Maylin S. Nicolas-Chanoine M. Insulin Resistance in Chronic Hepatitis C: Association With Genotypes 1 and 4, Serum HCV RNA Level, and Liver Fibrosis Gastroenterology 200813441642310.1053/j.gastro.2007.11.01018164296 · doi ↗ · pubmed ↗
- 6Villani R. Di Cosimo F. Romano A.D. Sangineto M. Serviddio G. Serum lipid profile in HCV patients treated with direct-acting antivirals: A systematic review and meta-analysis Sci. Rep.2021111394410.1038/s 41598-021-93251-334230541 PMC 8260657 · doi ↗ · pubmed ↗
- 7Cespiati A. Coelho Rodrigues I. Santos I. Policarpo S. Carvalhana S. Fracanzani A.L. Cortez-Pinto H. Effect of HCV eradication by DA As on liver steatosis, carotid atherosclerosis, and associated metabolic comorbidities: A systematic review Liver Int.2024441075109210.1111/liv.1587638385567 · doi ↗ · pubmed ↗
- 8Corey K.E. Kane E. Munroe C. Barlow L.L. Zheng H. Chung R.T. Hepatitis C virus infection and its clearance alter circulating lipids: Implications for long-term follow-up Hepatology 2009501030103710.1002/hep.2321919787818 PMC 4330996 · doi ↗ · pubmed ↗