Recognition, Diagnosis, and Treatment of Clostridioides difficile Enterocolitis Presenting Without Diarrhea: A Literature Review
Ezgi Yılmaz, Duygu Işıl Gencer, Mustafa Salih Akın, Meyha Şahin, Bahadır Ceylan, Ali Mert

TL;DR
This paper reviews cases of Clostridioides difficile infection without diarrhea, highlighting the risks of delayed diagnosis and poor outcomes.
Contribution
The study compiles 48 cases to emphasize the need for early recognition of CDI even when diarrhea is absent.
Findings
CDI cases without diarrhea had higher mortality and bowel resection rates.
Delayed diagnosis was linked to poor prognosis in these cases.
A high index of suspicion is crucial for early detection of CDI in atypical presentations.
Abstract
Diarrhea, as the well-known clinical feature of Clostridioides difficile infection (CDI), may be absent at the initial presentation, leading to delays in diagnosis. The delay is due to both underrecognition of such presentations and the dependence of CDI diagnosis on stool samples. This review was conducted to evaluate the literature for CDI cases presenting without diarrhea, raise awareness about the possibility of CDI in the differential diagnosis regardless of diarrhea, and assemble relevant data to harmonize clinical approaches. The PubMED Medline database was used to conduct this literature review, focusing on reported CDI cases presenting without diarrhea. After exclusions, 22 articles were included for analysis, providing data for 48 cases. This paper will present the selected clinical data of these 48 patients and follow a real-life case with a clinical course of CDI including…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
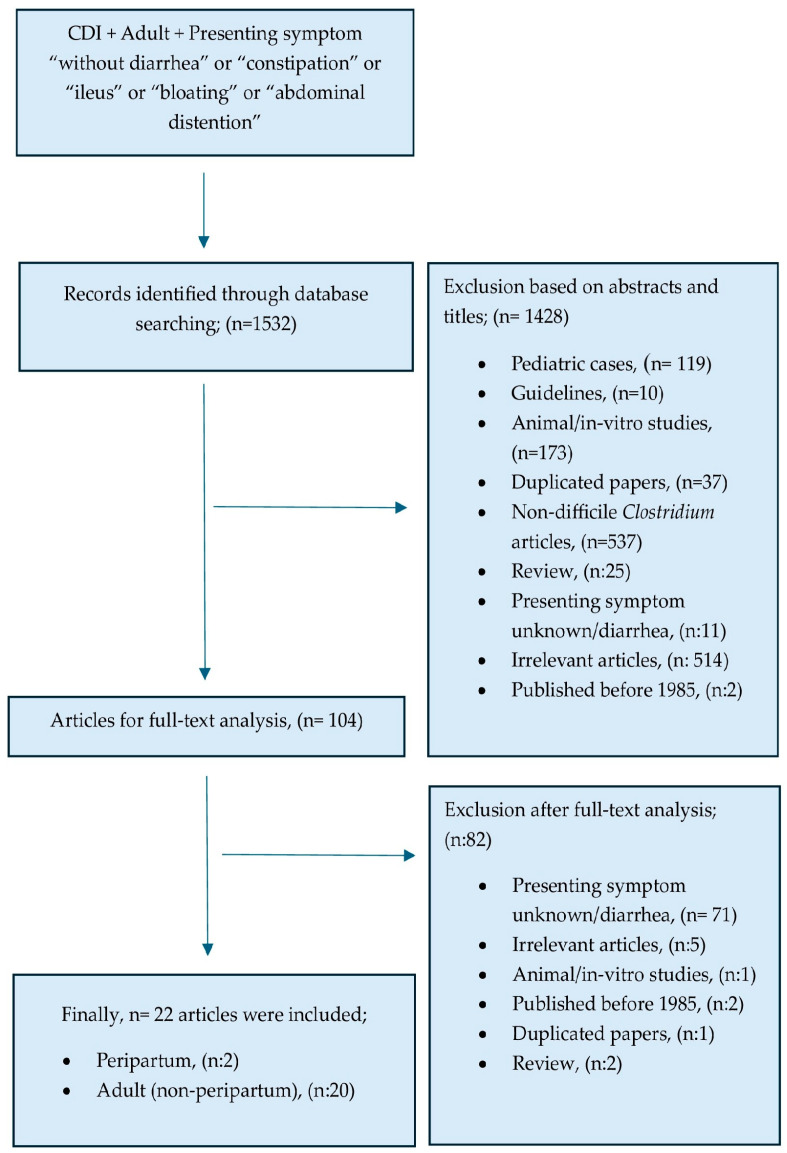 Figure 1
Figure 1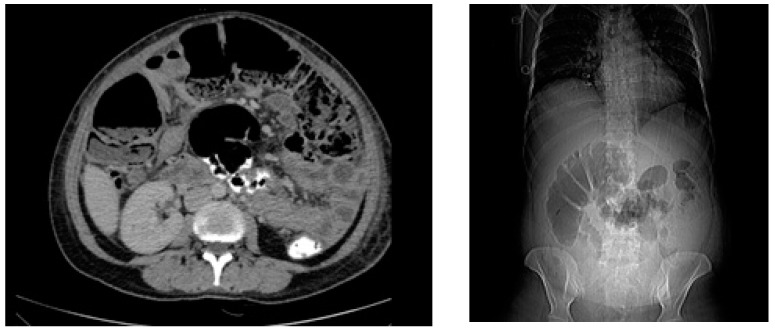 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Microscopic Colitis · Helicobacter pylori-related gastroenterology studies
1. Introduction
Clostridioides difficile infection (CDI) is defined by the presence of symptoms (usually diarrhea) and either a stool test positive for C. difficile toxins or detection of toxigenic C. difficile, or colonoscopic or histopathologic findings revealing pseudomembranous colitis in the Clinical Practice Guideline for CDI, by the Infectious Diseases Society of America (IDSA) [1]. Demonstration of the toxin or isolation of the C. difficile toxigenic strain from stool samples is diagnostic of CDI in appropriate clinical settings. Colonoscopic examination and biopsy can also provide evidence for the presence of CDI by visualizing the typical features described as pseudomembranous colitis [2]. CDI cases may range in clinical severity from asymptomatic carriage to profuse diarrhea, and occasionally to full-blown colitis complicated by toxic megacolon [3]. Rarely presented features of CDI include constipation, abdominal distension, isolated abdominal pain, or postoperative prolonged ileus, which have been sporadically reported in individual case descriptions or small case series. Reports suggesting an increasing CDI incidence in settings previously considered as low risk for CDIs (non-nosocomial, obstetric, etc.) have also been concerning. CDI diagnosis can be easily overlooked in practice with rare presentations due to their underrecognition and underrepresentation resulting in delayed or missed diagnosis, which may have serious consequences. To make matters worse, many laboratories only test stool for CDI in the presence of diarrhea, further reducing the probability of timely diagnosis when CDI presents with less familiar features [2]. Appreciating the current limitations in our understanding of CDI cases with rare presentations, the data from a laborious systematic literature review focusing on the recognition, diagnosis, and management of CDI presenting without diarrhea are displayed in this paper. The clinical course of a real-life case is described and discussed in relation to the literature. The aim was to raise awareness of rare CDI presentations by assembling relevant data and elaborating on ways to harmonize clinical approaches.
2. Material and Methods
We conducted a literature review using two different keyword sets to assemble all relevant data from the MEDLINE PubMED database (Figure 1). The first keyword set focused on CDIs presenting without diarrhea in adult patients (age > 18) using the combination “(((difficile) OR (pseudomembranous colitis) OR (clostiridium difficile)) AND ((ileus) OR (constipation) OR (obstipation) OR (bloating) OR (abdominal distention)))”. For the second search focusing on CDI in the obstetric setting, we used the following keyword combination,“(((pregnancy) OR (peripartum) OR (postpartum)) AND ((clostridium) OR (difficile) OR (pseudomembranous colitis) OR (pseudomembranous enterocolitis))). The search was conducted on the 3 of February 2025. Initial screening involved reviewing titles and abstracts to select relevant papers among all articles reached with the searched keyword combinations. Full texts were also reviewed during screening in cases where abstracts did not provide information regarding symptoms at presentation in the screening phase, and reported cases presenting with any severity of diarrhea were excluded only after full-text evaluation. Selected articles after screening were carefully analyzed and relevant data extracted. Papers not reporting novel information or providing case data regarding CDIs presenting without diarrhea were categorized as irrelevant and excluded from the analysis.
The case data described in the manuscript were retrieved retrospectively from institutional records. The patient signed an informed consent for the anonymous use of her clinical data for research purposes. The study was conducted and the manuscript prepared in accordance with the Declaration of Helsinki, strictly adhering to good clinical practice.
3. Results
3.1. Literature Overview
The two keyword combinations yielded a total number of 1532 articles. The flowchart of the screening, exclusion, and selection of these papers is shown in Figure 1. Full-text review was performed for 104 articles, and 22 articles were found relevant for the purposes of this review and included in the analysis. These 22 articles provided information about 48 patients who were diagnosed with and managed for CDI after presentation without diarrhea (Table 1 and Table 2). Adequate information on prior antibiotics, treatment, and diagnostic procedures was reported for 35 of these cases, whereas outcome data were available for 43 cases. Overall, 13 of these 43 cases (not including the clinical case discussed in this manuscript) succumbed to complications during CDI and surgery was needed in 13 cases, with most resulting in extensive bowel resection. Data regarding fever and leukocyte count at presentation were missing for about half of the patients (56% and 42%, respectively). Imaging modalities and data regarding inciting antibiotics were not available for 43.8% and 34% of the patients, respectively. Among the patients, about one-third had no medical treatment data available. Outcome data were missing for about 11% of them.
3.2. Clinical Case
3.2.1. Background and Presenting Symptoms
A 36-year-old, previously healthy, multiparous (G3/P2) pregnant woman underwent cesarean section (C/S) in the 36th week of pregnancy and was discharged from hospital two days after C/S. One week after the delivery, the patient presented to the emergency clinic with severe abdominal pain, lack of gas, stool discharge since C/S, and intractable vomiting.
3.2.2. Initial Evaluation and Recent History
The patient appeared critically ill, and she was febrile (38.4 °C); her blood pressure was 100/55 mmHg, and she was tachycardic (118 bpm). The physical examination was significant for diffuse pain on all four quadrants to palpation, hypoactive bowel sounds, and severe abdominal distension without rebound tenderness consistent with acute abdomen with prolonged postoperative ileus. There was no discharge from the site of incision. At presentation, laboratory tests were remarkable for anemia (Hgb = 7.7 g/dL) marked elevation in acute-phase reactants (CRP = 425 mg/L; procalcitonin = 0.33 ng/mL), and white blood cells with neutrophilic predominance (leukocytes: 14,100 cells/mm^3^; neutrophils: 85.4%). Abdominal CT was consistent with ileus without an obstructing mass or postoperative collection (Figure 2). Her recent obstetric history was unremarkable other than the administration of oral third-generation cephalosporin (cefdinir 600 mg q24h) for asymptomatic bacteriuria for five days on the 34th week of pregnancy. Postpartum, she had also used two days of cefdinir per oral as postoperative prophylaxis. After ruling out mechanical obstruction and surgical site infections, fulminant CDI was considered in the differential diagnosis based on the severity of the clinical picture, recent operation, hospitalization, and antibiotic use.
3.2.3. Diagnosis of CDI
After 24 h of admission, clinical status was not improved despite empirical wide-spectrum antibiotherapy (piperacillin–tazobactam) and supportive care. Abdominal discomfort was not relieved, and an urgent colonoscopy was performed on day 2, which demonstrated pseudomembranous patchy involvement and black ground ulcerative lesions in the cecum and ascending colonic mucosa. Highly suggestive features for CDI were observed, so fecal samples were collected via a rectally inserted tube and found positive for Clostridioides difficile toxin A/B by immunochromatographic methods along with positivity for glutamate dehydrogenase (Standard F C. difficile Toxin A/B FIA, SD Biosensor, India). Pathological examination of the colonic biopsy was consistent with pseudomembranous colitis by C. difficile.
3.2.4. Management of CDI
The patient was given vancomycin per oral(125 mg qid) plus metronidazole (500 mg tid) parenterally immediately after colonoscopy. Because of clinical instability, piperacillin–tazobactam was also continued. Two days after the onset of antibiotherapy, watery, non-bloody diarrhea of moderate severity was observed. On day 3, abdominal CT was repeated due to recurring abdominal pain, demonstrating a new fluid collection near the surgical incision. Specimens cultured from the drainage of this collection did not result in bacterial growth and the collection disappeared over the following days. On day 7, the clinical status was stabilized, and the diarrhea had resolved. The antibiotic combination was continued for 14 days, and the patient was discharged from the hospital in excellent health, maintaining her good condition in her outpatient visit after one year without recurrence.
3.3. Literature Review: CDI in the Obstetric Setting
The incidence of CDI in peripartum women has increased in the last 20 years [26,27]. Several risk factors for CDI have been described in the peripartum period such as cesarean section and antibiotherapy for asymptomatic bacteriuria, which is frequently administered in the last trimester. Prior antibiotherapy and cesarean delivery are recognized as predisposing factors for peripartum CDI, due to prolonged hospital stays and more frequent antibiotic use with C/S [27,28,29,30]. The risk of CDI increased with increasing numbers of antibiotics, cumulative doses, and the duration of antibiotherapy [29]. The most common antibiotic related to CDI was also cephalosporins in obstetric settings; all three patients including the case presented in this paper had used cephalosporin before the onset of CDI. Saha et al. stated that peripartum women diagnosed with CDI had a median of 2 days (range 1–6) of recent antibiotic use before the onset of symptoms [4]. The authors also emphasized that most of the CDI cases developed on days 4–9 of antibiotherapy, with the range extending up to 8 weeks after the end of antibiotic exposure.
3.4. Literature Review: CDI Presenting Without Diarrhea
CDI presenting without diarrhea is not uncommon in clinical practice. Experienced physicians commonly consider the possibility of CDI in the right clinical settings despite the absence of diarrhea [10,17,22]. However, these settings are underrepresented in the literature, and an earlier paper describing five cystic fibrosis (CF) patients with CDI argued that constipation during CDI could be attributed to CF [9]. Reported cases over time established that diarrhea was not an essential feature to suspect an ongoing CDI [10,20,22,24]. Between 1985 and 2024, forty-eight patients diagnosed with CDI in the absence of diarrhea were reported (Table 1 and Table 2). The median age was 59 years (range 21–82), and 58% were male. Previous medical history was available for 85% of the cases. Among them, eleven (26.8%) had hematologic or solid organ malignancy, six had cystic fibrosis, and two of them had a solid organ transplantation history. The predominant symptoms were constipation and/or abdominal distension in 38 of these 48 cases (79.1%). Body temperature was ≥38 °C in 61.9% (13/21) of patients at presentation, and 92.8% (26/28) had elevated white blood cell counts, with most of these being above 15,000 cells/microL. Previous antimicrobial use was documented in all but one of the reported patients (Table 1). Beta-lactams (two-thirds cephalosporins) were the most commonly prescribed antibiotics (n:19), followed by quinolones (n:8), cotrimoxazole (n:5), and clindamycin (n:4). Previous vancomycin use alone or with other antibiotics was also reported for eight cases. Data on abdominal radiography and/or computed tomography were available in 27 of the patients, and large bowel dilatation was the most consistent finding; colonic wall thickening suggestive of colitis was observed in 11 of these cases (Table 1).
3.5. Literature Review: Diagnosis of CDI in the Absence of Defecation
Rampling et al. and Triadafilopoulos et al. were among the earliest researchers to report CDI presenting with ileus in 1985 and 1991, respectively [4,5]. These papers document eight cases of CDI without diarrhea, among which six were diagnosed via urgent colonoscopy (Table 2). In 2001, Sheikh et al. reported a case of pseudomembranous colitis without diarrhea presenting clinically as acute intestinal pseudo-obstruction, who did not respond to conservative management and then underwent colonoscopic biopsy, which returned positive for C. difficile toxins despite stool samples being negative [11]. These earlier reports were pivotal in establishing that CDI could present without diarrhea and raising awareness of this phenomenon. These papers also emphasized the potential of stool testing in evaluating ileus. Despite the absence of diarrhea at the presentation, stool samples were obtained through various interventions in 43.7% (21/48) of cases reported in the literature (through digital disimpaction, n: 5; after lactulose laxative use, n: 3; via rectal tube, n: 3; after enema, n: 2; defecation after suppository use, n: 2; defecation after colonoscopic decompression, n: 2; sampling from ileostomy post-surgically, n: 2; stool sampling during colonoscopy, n: 2) (Table 2) [10,11,12,13,14,18,19,20,22,23,24,25]. The method was not specified for 12 patients from whom stool samples were obtained. Tests on stool samples included latex particle agglutination (n: 6), cytotoxicity assays (n: 3), C. difficile toxin assays (n: 12), C. difficile toxin PCR testing (n: 8), and stool cultures (n: 4). Testing for stool samples attained through various interventions was pivotal in reaching a CDI diagnosis and administering potentially life-saving treatments in these 21 cases. Urgent colonoscopy (or proctoscopy/sigmoidoscopy) was performed in 14 cases, demonstrating pseudomembranous colitis in 85.7% (12/14) of these cases, which established or confirmed CDI diagnosis (Table 2). No complication associated with colonoscopy was reported among these 14 cases. The in-hospital mortality was 1 in 14 among those undergoing emergency colonoscopy, while 12 of the remaining 34 cases succumbed to CDI. Although compelling, this comparison was statistically insignificant (Fischer’s exact test p = 0.07). Surgical exploration for diagnostic purposes was performed in five cases (Table 2). Two cases of CDIs presenting without diarrhea in the obstetric setting were also previously reported (Table 2) [15,25]. Both patients were exposed to beta-lactams, presented with ileus, and diagnosed with CDI by testing stool samples for C. difficile toxin.
3.6. Literature Review: Management of CDI Presenting Without Diarrhea
Information regarding antibiotherapy for CDI was available for 27 (56%) of the 48 patients in the literature (Table 2). Metronidazole (monotherapy or combination) was the most common antibiotic administered to patients with CDI who presented without diarrhea (88.8%), mostly by the intravenous route. Vancomycin was administered either orally or colloquially in 53.8% of patients, and 26.5% of patients received a combination of vancomycin and metronidazole (Table 2). Five of thirteen (38.4%) patients receiving metronidazole monotherapy died, while the outcomes of eight other patients receiving metronidazole therapy could not be clarified; four of these may have also succumbed to the disease. Twelve of fourteen patients (84.6%) receiving vancomycin (either alone or in combination with metronidazole) survived the event (Fischer’s exact test p = 0.36). Colonic resection was reported in 13 of these 48 patients (27.0%); however, surgical outcomes were not specified in detail consistently. Bowel resection was needed in six among twelve patients treated with metronidazole alone and two among ten patients receiving combination antibiotics. We did not detect any variable with statistical significance for mortality between antibiotics, surgery, and colonoscopic evaluation, mainly due to the small sample size. Thirteen of the forty-three CDI patients (30.2%) who presented without diarrhea succumbed to the disease and the outcomes for the remaining five cases were not reported. Among the 30 survivors, 7 (23.3%) had to undergo extensive bowel resection while 1 patient suffered persistent kidney failure starting on renal replacement therapy after the CDI episode (Table 2). Two of the three cases of CDIs presenting without diarrhea in the obstetric setting, including the case reported in this paper, received a combination of metronidazole and vancomycin and fully recovered. The other obstetric case was delayed in diagnosis due to confounding factors, received IV metronidazole monotherapy, and had to undergo extensive bowel resection.
4. Discussion
Deviation from the familiar patterns of presentation or evolution of diseases is confusing for clinicians. Delays in timely diagnosis as well as potentially life- or organ-saving treatments are common in such circumstances. Patients presenting with constipation or ileus are less likely to be considered and tested for CDI due to the underrecognition of this feature, and the difficulties and risks of attaining stool samples in such a setting. On the other hand, physicians should be aware of the concept of colonization with Clostridioides difficile in patients without abdominal symptoms (and make sure that incidental findings on stool tests correspond to relevant clinical manifestations of CDIs as outlined in the literature overview (Table 1) to avoid overdiagnosis [3]
CDI in general is a severe disease associated with high morbidity and mortality. The 30-day mortality ranged between 5 and 34% in the literature [31,32,33,34]. This literature review focused on CDI presenting without diarrhea documented a mortality rate at the higher end of this spectrum at 30.2% (13/43), confirming that such a presentation can be indicative of a severe form of CDI. Considering the difficulties in recognition and diagnosis of CDIs with such presentation as discussed above, an earlier report () suggested that many cases may have gone undiagnosed, and the actual incidence and mortality rate may be even higher [22]
Data assembled through this literature review highlighted some key features. First of all, most of the diagnoses reported in the literature were products of a high index of suspicion for CDI. This was mainly noticeable through efforts to obtain stool samples in various ways to test for CDI in 21 cases. It was hardly possible for most of these 21 patients to be diagnosed without careful recognition of the possibility of CDI. Another noteworthy observation was the performance of urgent colonoscopy and the accurate recognition of the colonoscopic appearance, which may have contributed to timely management since patients undergoing urgent colonoscopy mostly survived without a complication (mortality undergoing colonoscopy/sigmoidoscopy: 1/14 vs. 12/34; p = 0.07).
The other key feature was the high frequency of the presence of poorly prognostic variables for the commonly used Zar score [35] (leukocytosis, fever, older age) among cases of CDI presenting without diarrhea. Potentially high Zar scores coupled with the high mortality and resection rates documented in this study confirm the gravity of this setting. Observing that only 27 of the 48 patients survived without bowel resection, we can confirm the unmet needs in CDIs presenting without diarrhea.
There are currently insufficient data to generate unanimous recommendations for the diagnosis and management approaches specific to CDIs presenting with ileus, considering the limitations of the available literature presented in this paper. The key limitations of the literature include but are not limited to the low number of reported cases, unavailability of data for leukocyte counts, fever, imaging details, antibiotic durations, and outcomes in a proportion of patients, as well as heterogeneous practices across reporting centers. The high mortality and morbidity rates reported with this pooled analysis are rough estimates at best, due to the influence of both publication bias, which may contribute to the overestimation of morbidity, and the unknown outcomes of possible cases that were undiagnosed. The assembled cases make it clear that CDI can present with ileus and its timely diagnosis requires a high index of suspicion, whereas its true incidence among patients presenting with non-mechanical ileus is yet to be explored. Appreciating the possible complications of high-volume enemas or colonoscopy in the presence of ileus, a cautious approach to attaining stool samples by prioritizing the minimally invasive and safest methods is called for. To the best extent of our understanding, CDI should be considered more strongly in the differential diagnosis of ileus with recent antibiotic exposures, hospitalization, absence of mechanical obstruction in non-invasive imaging, and the absence of other common causes such as electrolyte anomalies or opioid use. The stronger the consideration, the more invasive methods such as higher-volume enemas or colonoscopies may be justified. A multi-disciplinary approach with the involvement of gastroenterology and general surgery would ensure patient safety. Regarding treatment, a tendency towards better outcomes (numerically fewer deaths and bowel resections) with vancomycin is in line with general principles in managing CDIs, and preference of vancomycin should be strongly considered (for fulminant CDI, strong recommendation, moderate quality of evidence) [1]. Although none of the 48 patients reviewed here received fidaxomicin, data from trials are encouraging (conditional recommendation, moderate quality of evidence) for patients with an initial episode of CDI, with costs and availability remaining as obstacles [36]. The addition of intravenous metronidazole, especially when ileus is documented, and considerations for surgical interventions need to be individualized as recommended for all CDI patients [1]. Fecal microbiota transplantation (FMT), another important treatment modality for recurring CDIs, is yet to be explored in the setting when CDI presents without diarrhea [36].
5. Conclusions
CDI presenting without diarrhea can be associated with high mortality and morbidity rates, potentially exceeding those of typical CDI cases. Delay in diagnosis due to unfamiliar presentation is a likely contributor to this poor prognosis. We encourage the consideration of CDI in the differential diagnosis of ileus or megacolon in the appropriate setting of previous antibiotic use or hospitalization, especially if imaging is not suggestive of mechanical obstruction. Increased awareness and prompt actions to reach diagnosis early in the course by attaining stool samples with the safest methods possible may allow timely CDI diagnosis and reverse the unfavorable prognosis. Vancomycin treatment, as recommended for all CDI cases, may be associated with improved outcomes.
6. Future Directions
We consider that the true incidence and mortality of CDIs presenting without diarrhea may be higher than that represented in the literature due to diagnostic challenges and underrecognition among clinicians as discussed throughout the manuscript. It may be worthwhile to formulate standardized reporting protocols for atypical CDI presentations as prospective registries incorporating data for presenting symptoms, vital signs, comorbidities, leukocyte counts, details of prior antibiotic use, recent hospitalizations, surgery, and diagnostic procedures, along with doses and duration of CDI-directed therapies and surgical interventions. Carefully collected data in the form of such standardized protocols will not only raise awareness but also allow us to better understand this challenging condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Donald L.C. Gerding D.N. Johnson S. Bakken J.S. Carroll K.C. Coffin S.E. Dubberke E.R. Garey K.W. Gould C.V. Kelly C. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)Clin. Infect. Dis.201866 e 1e 4810.1093/cid/cix 108529462280 PMC 6018983 · doi ↗ · pubmed ↗
- 2Bagdasarian N. Rao K. Malani P.N. Diagnosis and treatment of Clostridium difficile in adults: A systematic review JAMA 201531339840810.1001/jama.2014.1710325626036 PMC 6561347 · doi ↗ · pubmed ↗
- 3Schäffler H. Breitrück A. Clostridium difficile—From Colonization to Infection Front. Microbiol.2018964610.3389/fmicb.2018.0064629692762 PMC 5902504 · doi ↗ · pubmed ↗
- 4Rampling A. Warren R.E. Bevan P.C. Hoggarth C.E. Swirsky D. Hayhoe F.G. Clostridium difficile in haematological malignancy J. Clin. Pathol.19853844545110.1136/jcp.38.4.4453857233 PMC 499176 · doi ↗ · pubmed ↗
- 5Triadafilopoulos G. Hallstone A.E. Acute abdomen as the first presentation of pseudomembranous colitis Gastroenterology 199110168569110.1016/0016-5085(91)90526-Q 1860633 · doi ↗ · pubmed ↗
- 6Medich D.S. Lee K.K. Simmons R.L. Grubbs P.E. Yang H.C. Showalter D.P. Laparotomy for fulminant pseudomembranous colitis Arch. Surg.199212784785310.1001/archsurg.1992.014200701110201524485 · doi ↗ · pubmed ↗
- 7Cunney R.J. Magee C. Mc Namara E. Smyth E.G. Walshe J. Clostridium difficile colitis associated with chronic renal failure Nephrol. Dial. Transplant.1998132842284610.1093/ndt/13.11.28429829488 · doi ↗ · pubmed ↗
- 8Kovithavongs T. Clostridium difficile colitis associated with chronic renal failure Nephrol. Dial. Transplant.1999142256225710.1093/ndt/14.9.225610489247 · doi ↗ · pubmed ↗