Pituitary Spindle Cell Oncocytoma: More than a Grade 1 Tumor?
Jonathan Hammond, Zacharie Gagne, Bojana Mitrovic, Stefano M. Priola

TL;DR
Pituitary spindle cell oncocytomas are rare tumors that behave more aggressively than their grade suggests, requiring careful diagnosis, treatment, and follow-up.
Contribution
The paper highlights the need for adjuvant radiotherapy and close monitoring due to the tumor's high recurrence risk.
Findings
Pituitary SCOs have high vascularity and strong adherence to surrounding structures, leading to higher recurrence rates.
Adjuvant radiotherapy should be considered when complete resection is not achieved.
Diligent follow-up is essential to detect recurrence or progression.
Abstract
Background/Objectives: Spindle cell oncocytomas (SCOs) of the pituitary gland are rare tumors often misdiagnosed for nonfunctioning pituitary macroadenomas. Although classified as grade 1, they are often challenging in terms of diagnosis and treatment. Pituitary SCOs harbor peculiar features such as hypervascularity and stronger adherence to surrounding structures, with increased risk of hemorrhage, partial resection, and significantly higher recurrence rate. Almost 100 cases have been reported so far. The role of surgery is still crucial for the decompression of the optic chiasm as well as for achieving diagnosis. However, given the higher tendency of recurrence, the role of postoperative radiotherapy has been investigated over the last few years. Case presentation: Here, we reported a case of a 48-year-old female with a pituitary SCO treated at our institution, in which we focused on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1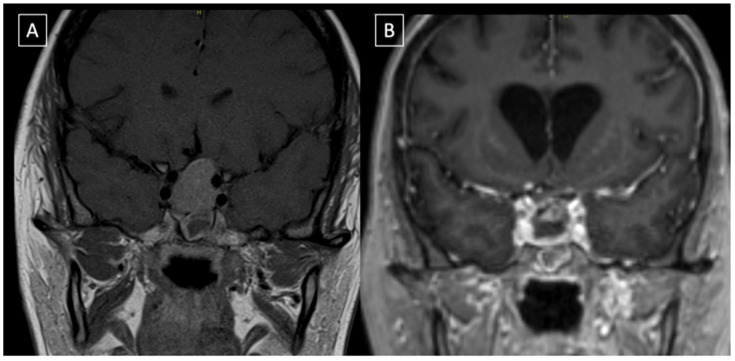 Figure 2
Figure 2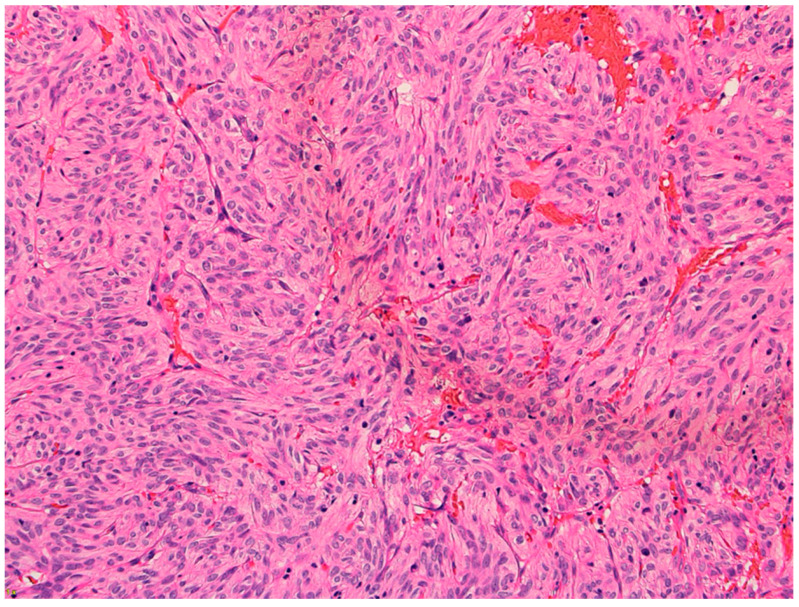 Figure 3
Figure 3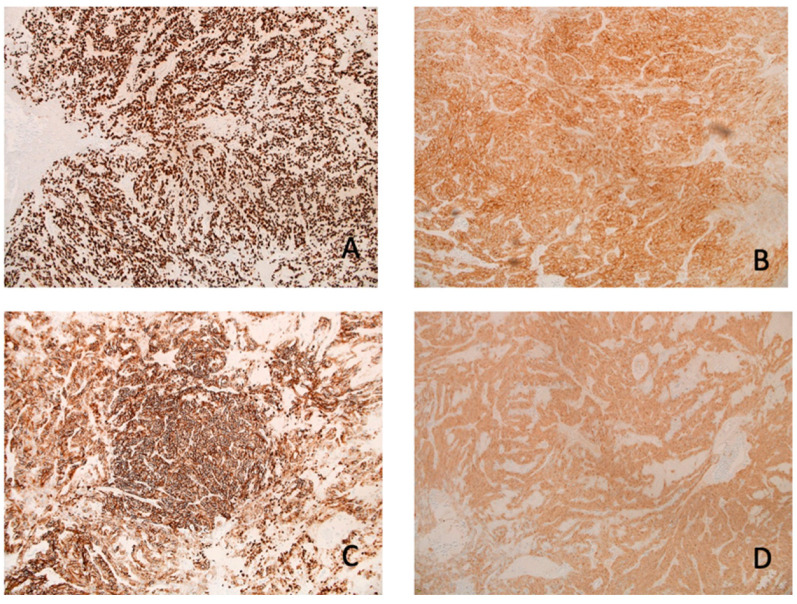 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPituitary Gland Disorders and Treatments · Glioma Diagnosis and Treatment · Adrenal and Paraganglionic Tumors
1. Introduction
Spindle cell oncocytomas (SCOs) are rare non-neuroendocrine tumors arising from the pituicytes of the posterior pituitary gland. They were included in the World Health Organization (WHO) classification of central nervous system tumors in 2007 after being first described by Roncaroli et al. in 2002 [1,2].
SCOs were previously thought to stem from the adenohypophysis; however, more recent research identified that SCOs are positive for thyroid transcription factor 1 (TTF1) which is only found in pituicytes and not in the folliculostellate cells of the adenohypophysis [3]. In our search from 2002 to 2024, there were only 98 cases published in the literature that highlight the rarity of this type of tumor.
SCOs are often misdiagnosed as pituitary adenomas; nevertheless, they are important to distinguish as they usually have higher vascularity as well as an increased tendency to invade the surrounding structures [4]. This results in a higher recurrence rate, thus requiring more frequent follow-ups. If gross total resection (GTR) is not achieved, 50% of tumors show significant progression requiring extra treatment by two years, recurrence occurs in 20% of people, and even distant metastasis has been reported [4].
Despite these factors, the WHO considers pituitary SCOs a grade 1 tumor with benign behavior [5]. Moreover, although this tumor is considered grade 1, it is important to understand these critical features as it guides treatment and follow-up and will improve patient outcomes.
Due to the low incidence of this neoplasm, the definitive knowledge of the unique clinical signs and symptoms, diagnostic imaging (DI), immunohistochemistry (IHC), and treatment is lacking. In this report and literature review, we aimed to provide further knowledge on these factors to improve the identification and treatment of individuals with SCO. In addition, the role of adjuvant radiotherapy is not fully understood in the treatment of pituitary SCO. However, recent literature demonstrated radiotherapy to be safe and effective for residual SCO after surgery [6]. Radiotherapy will be further assessed in our review of the literature to also help establish a comprehensive understanding of its potential role in the treatment of SCO.
2. Case Presentation
We present the case of a 48-year-old female with a two-month history of persistent headaches, mental and physical fatigue, and light sensitivity. Her past medical history includes chronic migraines, fibromyalgia, psoriasis, anxiety, obesity, and obstructive sleep apnea. When looking back, the patient realized that her headache symptoms had changed from her normal migraine symptoms to more frequent albeit less severe frontal pain and aching in the previous months.
Given the persistence of the above-mentioned symptoms, she was investigated with a head computed tomography (CT) scan, which showed a pituitary lesion with sellar and suprasellar extension. For further investigation, she underwent a brain magnetic resonance imaging (MRI) scan that demonstrated a homogenous mass in the pituitary gland (Figure 1). The MRI also showed that the mass was compressing the optic chiasm and was encasing both internal carotid arteries. These findings were thought to be compatible with pituitary macroadenoma.
On physical examination, the patient had no cranial nerve deficits, and her pupils were equal, round, and reactive to light and accommodation. She did not have any focal motor or sensory deficits. She also underwent an ophthalmological assessment that ruled-out papilledema and confirmed normal bilateral visual fields. Lastly, a thorough endocrinological assessment was completed, including a full hormonal panel that demonstrated only mild hyperprolactinemia.
Given the clinical and radiological findings, an elective surgical treatment was recommended and carried out using an endoscopic endonasal transsphenoidal approach. Intraoperatively, the tumor had the usual soft consistency, but it presented stronger adherence with what was thought to be the normal pituitary gland and, therefore, required extra work to separate it. Although no major bleeding was identified, an unusual constant tumor oozing made the procedure more challenging. An apparent GTR of the tumor was achieved and confirmed by the direct visualization of the suprasellar cistern coming down into the sella turcica. For this reason, no adjuvant radiotherapy was performed.
The patient had an uneventful postoperative period. She spent two days in the intensive care unit and was then transferred to the floor, where low levels of cortisol and mild diabetes insipidus were diagnosed and treated medically. Post-operative MRI ruled out intraoperative complications and confirmed the decompression of the optic chiasm (Figure 2). She was discharged home on postoperative day seven, neurologically intact.
She was reassessed in the follow-up four weeks after surgery, and no obvious focal deficits were identified. Her headache and light sensitivity had notably improved. A repeat MRI was completed three months postoperatively, and it confirmed the GTR of the SCO; the patient scheduled their next follow-up with repeat MRI at the sixth month mark.
The microscopy examination of the specimen demonstrated fascicles of spindle-cell tumor cells with eosinophilic cytoplasm and elongated nuclei showing moderate pleomorphism (Figure 3). Other areas of tumor cells showed more eosinophilic cytoplasm with clear borders and contained round to oval nuclei with mild pleomorphism. Granular cytoplasm was not seen; however, mitotic figures were present. No tumor necrosis was noted. The tumor cells were diffusely positive for TTF-1, S100, CD56, and synaptophysin (Figure 4). They were also focally positive for epithelial membrane antigen (EMA), glial fibrillary acidic protein (GFAP), CD68, and beta crystallin. There was no immunostaining for pituitary-specific transcription factor-1 (PIT-1) or steroidogenic factor-1 (SF-1).
3. Discussion
SCOs are very rare tumors of the posterior pituitary gland that originate from the pituicytes located in the neurohypophysis. They are called SCOs because their cells are spindle shaped under microscopic examination and contain many mitochondria in their cytoplasm [7]. Oncocytomas can occur in many different areas of the body, including kidney, breast, prostate gland, thyroid, and salivary glands [7]. However, they are often only called oncocytomas in these locations as they lack spindle-shaped cells, which are characteristic of the pituitary SCO [7,8].
Unfortunately, pituitary SCOs appear very similar to non-functioning pituitary adenomas in clinical presentation and diagnostic imaging. Yet, they require unique care because of two specific features: increased vascularity and increased fibrotic adherence to surrounding structures.
Additionally, SCOs’ increased vascularity has the potential to cause significant bleeding during surgery. Borges et al. described a case of recurring subclinical tumor bleeding that happened in a recurrent SCO [9,10]. In the same manuscript, Borges reported that nearly one-third of assessed cases showed significant intraoperative bleeding, and almost half of these cases demonstrated that the tumor was highly vascular [9,10]. Cases of spontaneous tumor hemorrhage were also described.
Careful tumor dissection and the strategic use of cottonoids with hemostatic agents is crucial when dealing with any tumor of the posterior pituitary gland, especially SCO. Also, SCOs have an elevated risk of progression or recurrence because of the adherent characteristics of the tumor. In a study by Hasegawa et al., it was found that GTR was only achieved in 24% of cases mainly because of those tumor features [5]. These characteristics make the recurrence of SCOs very likely, with 50% of tumors showing significant progression if GTR is not attained and radiotherapy is not added [5].
There are also case reports of SCOs managed transcranially. In fact, in cases with extensive suprasellar extension, this approach can allow for more intraoperative maneuverability to deal with significant bleeding and provide better accessibility to all areas of the tumor [10].
Oftentimes, partial resection is all that can be accomplished, leading to the growth of any residual tumor. In cases like this and with general tumor recurrence, interdisciplinary support should be pursued and thought given to both reoperation as well as adjuvant radiotherapy [10].
The role of preoperative radiotherapy is still being debated; Hasegawa et al. found in their meta-analysis that preoperative radiotherapy did not have an impact on those who achieved GTR [5]. There was also no statistical difference between the non-GTR group that received preoperative radiotherapy and the non-GTR group that did not receive preoperative radiotherapy. However, in patients who do not achieve GTR, postoperative radiotherapy should be considered as it has shown promising results in controlling tumor progression [11].
In our review of the literature (Table 1), we performed a search from 2002 to 2024 using databases such as PubMed, Google Scholar, and ScienceDirect to identify all published articles reporting pituitary SCO, which totaled 98 cases. Primary search terms included pituitary spindle cell oncocytoma, pituitary tumors, and posterior pituitary tumors. Case reports, case series, and original articles were included, whereas articles not presenting new cases or unpublished material were excluded. Article references were also hand searched to ensure no reports were missed. Each case was then analyzed for specific data points, including age, sex, clinical presentation, diagnostic imaging, IHC, surgical approach, use of adjuvant radiotherapy, and general outcomes. The data were then summarized into a structured table which was used to draw conclusions on significant topics like recurrence rates and the effectiveness of radiotherapy, as well as to present all cases reported in the literature thus far. All articles were screened for relevance by the authors, and any discrepancies were resolved through collaborative discussion.
The mean age of all the patients with pituitary SCO was found to be fifty-seven years. Regarding any difference between sex, forty-seven patients were female, and fifty-one patients were male. Of particular importance, we found that there was recurrence or tumor growth in 31% of patients with pituitary SCO who did not receive adjuvant radiotherapy. Meanwhile, only 18% of patients who did receive adjuvant radiotherapy experienced tumor recurrence or progression. This information on adjuvant radiotherapy shows that it has the potential to be very useful in achieving tumor stability and decreases the chances of progression and need for further operations. Akyoldas et al. reported five cases that utilized radiotherapy, all of which showed the tumors to be stable at follow-up. Also, in this study, gamma knife radiosurgery was used each time and reported a median tumor margin dose of 12Gy and a median maximal dose of 24Gy [6].
These rates of recurrence/progression underscore the importance of continued surveillance with these tumors. Many of the reports noted how partial resection was all that could be achieved due to the highly vascular nature of the tumor. However, recurrence was even found in cases that appeared to achieve GTR.
Our case specifically highlights the importance of being aware of the high vascularity of these tumors due to their increased risk of bleeding during surgical resection. If a SCO is suspected/identified, measures can be put into place to prepare for increased bleeding, such as careful tumor dissection and strategic use of cottonoids with hemostatic agents in addition to blood products typed and matched if they are needed. Special consideration is also needed regarding the follow-up plan for patients with SCO due to their increased rate of recurrence.
4. Conclusions
SCOs are rare tumors of the posterior pituitary gland that have many unique features that require specific treatment and follow-up. Although this tumor presents similarly to a pituitary adenoma, there are marked differences in the physical appearance of the tumor, IHC, and follow-up required. From a surgical perspective, the challenge is related to higher vascularity and stronger adherence to the surrounding structures. This makes the surgery itself more difficult and a GTR less likely, with a higher recurrence rate.
To date, the use of radiotherapy was not well established. However, our review does provide encouraging results that post-operative radiotherapy has the potential to minimize tumor progression and increase tumor stability. Only 18% of the patients who had a pituitary SCO and received adjuvant radiotherapy developed recurrence/progression compared to 31% of patients who did not receive adjuvant radiotherapy.
In our opinion, radiotherapy should definitely be considered, especially when GTR is not achieved. In our case, a GTR was achieved; thus, we decided to proceed without radiotherapy and with closer follow-up appointments to identify any early sign of recurrence. Closer follow-up appointments are also very necessary as many patients develop recurrence or tumor progression, sometimes despite GTR. These high rates of tumor recurrence/progression underscore the need for careful and frequent monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roncaroli F. Scheithauer B.W. Cenacchi G. Horvath E. Kovacs K. Lloyd R.V. Abell-Aleff P. Santi M. Yates A.J. Spindle cell oncocytoma of the adenohypophysis: A tumor of folliculostellate cells?Am. J. Pathol.2002261048105510.1097/00000478-200208000-0001012170092 · doi ↗ · pubmed ↗
- 2Joshi S. Krishnamurthy B. Mc Kelvie P. Dhillon R. Case report of pituitary spindle cell oncocytoma concurrent to growth-hormone secreting pituitary adenoma Interdiscip. Neurosurg. Adv. Tech. Case Manag.20243610197110.1016/j.inat.2024.101971 · doi ↗
- 3Guerrero-Pérez F. Vidal N. Marengo A.P. Del Pozo C. Blanco C. Rivero-Celada D. Díez J.J. Iglesias P. PicóA. Posterior pituitary tumours: The spectrum of a unique entity Endocrine 201963364310.1007/s 12020-018-1774-230276594 · doi ↗ · pubmed ↗
- 4Kunihiro J. Inoue A. Miyake T. Ohno T. Kitazawa R. Kunieda T. Clinicopathological features and endoscopic findings of spindle cell oncocytoma: A case report and review of the literature Int. J. Surg. Case Rep.202310910853610.1016/j.ijscr.2023.10853637487353 PMC 10369474 · doi ↗ · pubmed ↗
- 5Hasegawa H. Van Gompel J.J. Oushy S.H. Pollock B.E. Link M.J. Meyer F.B. Bancos I. Erickson D. Davidge-Pitts C.J. Little J.T. A Comprehensive Study of Spindle Cell Oncocytoma of the Pituitary Gland: Series of 6 Cases and Meta-Analysis of 85 Cases World Neurosurg.2021149 E 197E 21610.1016/j.wneu.2021.02.05133610869 · doi ↗ · pubmed ↗
- 6AkyoldaşG. Hergünsel B. Özdemir I.E. Şengöz M. Peker S. Gamma knife radiosurgery for pituitary spindle cell oncocytomas Clin. Neurol. Neurosurg.201918710556010.1016/j.clineuro.2019.10556031648114 · doi ↗ · pubmed ↗
- 7Hodzic Z. Rowan N.R. Kashiwazaki R. Willson T.J. Wang E.W. Lee S.E. A systematic review of sinonasal oncocytomas and oncocytic carcinomas: Diagnosis, management, and technical considerations Int. Forum Allergy Rhinol.2017751452410.1002/alr.2190228092140 · doi ↗ · pubmed ↗
- 8Hsieh Y.-Y. Chien S.-C. Tsai H.-C. Wei K.-C. Chuang C.-C. Jung S.-M. Pituitary spindle cell oncocytoma: Two cases report and literature review Int. J. Surg. Case Rep.202412411032810.1016/j.ijscr.2024.11032839353313 PMC 11472096 · doi ↗ · pubmed ↗