Echocardiographic Assessment of Cardiac Structure and Function of Centenarians: A Systematic Review
Andrea Sonaglioni, Gian Luigi Nicolosi, Giovanna Elsa Ute Muti-Schünemann, Alessio Polymeropoulos, Michele Lombardo, Paola Muti

TL;DR
This review summarizes echocardiographic findings in centenarians, showing heart structure changes and diastolic dysfunction despite normal systolic function.
Contribution
The study systematically compiles and analyzes echocardiographic data from centenarians to understand age-related cardiac changes.
Findings
Centenarians show LV concentric remodeling and diastolic dysfunction with normal systolic function.
Hospitalized centenarians exhibit more severe valvular heart disease and pulmonary hypertension.
HFpEF is a significant risk due to increased myocardial stiffness in this population.
Abstract
Background: During the last two decades, a limited number of studies have provided echocardiographic details regarding the cardiac structure and function of individuals aged ≥100 years. These studies analyzed limited sample sizes of centenarians using different methodologies. The present systematic review was primarily designed to summarize the main findings of these studies and to examine the overall influence of extremely advanced age on cardiac structure and function. Methods: All echocardiographic studies that evaluated the cardiac structure and function in individuals aged ≥100 years, selected from the PubMed, Embase, Scopus and Cochrane Central Register of Controlled Trials (CENTRAL) databases, were included. There was no limitation on the time period. The risk of bias was assessed by using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
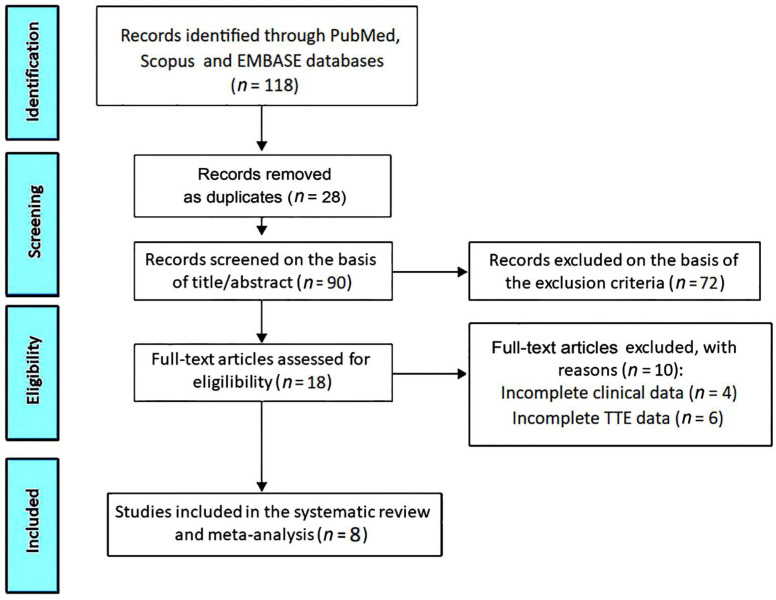 Figure 1
Figure 1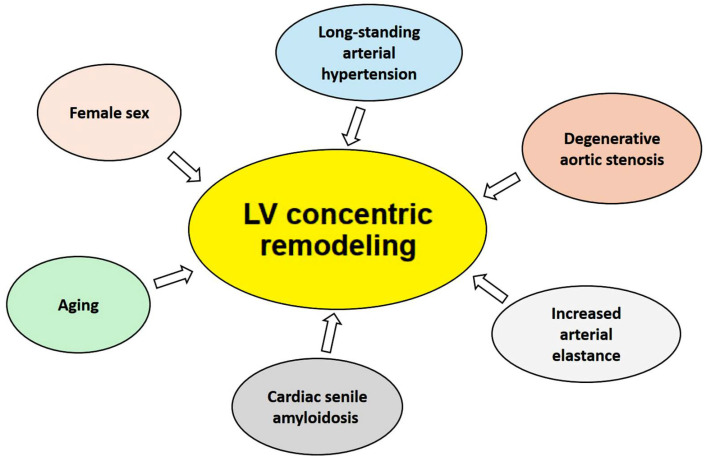 Figure 2
Figure 2- —Italian Ministry of Health, Ricerca Corrente IRCCS MultiMedica
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Mitochondrial Function and Pathology · Genetics, Aging, and Longevity in Model Organisms
1. Introduction
The mean age of the current global population is rapidly increasing. According to the World Health Organization (WHO), the number of people aged 80 years and older is expected to triple between 2020 and 2050, reaching 426 million [1]. More remarkably, the number of centenarians has doubled every decade since the 1950s and is estimated to increase five-fold by the year 2050 [2]. Due to the increase in prevalence of centenarians, they are regularly encountered in clinical practice [3]. Studies on longevity demonstrated that the interaction between genetic and environmental factors favors aging [4,5]. Among this particular population, cardiovascular disease is frequent and represents the most common cause of mortality [6,7,8]. Transthoracic echocardiography (TTE) is an essential tool for the evaluation of age-associated structural and functional cardiac alterations. This noninvasive imaging modality allows for obtaining useful information on cardiac chamber internal dimensions, left ventricular (LV) diastolic function, biventricular systolic function, morphology and function of the heart valves, and pulmonary hemodynamics. To date, cardiac remodeling has been poorly investigated in the “oldest-old” individuals [9]. During the last two decades, a few echocardiographic studies provided detailed assessments on the cardiac structure and function of individuals aged ≥100 years. These studies comprised limited sample sizes and used different methodologies. The present systematic review was primarily designed to summarize the main findings of these studies and examine the overall influence of extremely advanced age on cardiac structure and function. The pathophysiological mechanisms underpinning the cardiac remodeling that occurs in centenarians are discussed as well.
2. Methods
This systematic review was performed in accordance with the recommendations of the PRISMA guidelines [10] and was registered in the INPLASY database on 3 November 2024 (registration number INPLASY2024110010).
2.1. Search Strategy
A comprehensive search of all echocardiographic studies that evaluated the cardiac structure and function of individuals aged ≥100 years was carried out by two independent reviewers (A.S. and M.L.) up to November 2024 by using the PubMed, Embase, Scopus and Cochrane Central Register of Controlled Trials (CENTRAL) databases. The search was last updated on 11 November 2024. The search strategy included the following terms: “centenarians” AND “transthoracic echocardiography” AND “cardiac function” OR “left ventricular ejection fraction”. Published studies were sought after with the language restriction to English. Forward and backward citation searches were conducted.
2.2. Eligibility Criteria
Studies were included for review if they met the following criteria: they evaluated the echocardiographic characteristics of centenarians, regardless of the time frame. Studies were excluded based on predefined criteria: non-English language, if they were focused on centenarians without or with incomplete echocardiographic data, studies that involved individuals aged <100 years, non-clinical articles, animal studies, duplicate articles, systematic and narrative reviews, case reports, conference presentations, correspondences, editorials, letters without data and abstracts.
2.3. Study Selection and Data Extraction
Two reviewers (A.S. and M.L.) independently performed title and abstract and full text screenings of the aforementioned databases according to the inclusion criteria. Data extraction was independently performed for the following information concerning centenarians: (1) demographics (age and sex); (2) anthropometrics [body surface area (BSA) and body mass index (BMI)]; (3) prevalence of the most common cardiovascular risk factors (hypertension, smoking, type 2 diabetes and dyslipidemia); (4) previous history of coronary artery disease (CAD), heart failure and/or transient ischemic attack (TIA)/stroke; (5) comorbidity burden and comorbidity indexes, such as the Charlson comorbidity index (CCI) [11] and the Katz index [12]; (6) physical examination [systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate]; (7) electrocardiographic (ECG) data, such as the cardiac rhythm and the pattern of intraventricular conduction; (8) biochemical parameters, such as the serum levels of hemoglobin, creatinine, cholesterol and N-terminal pro-B-type natriuretic peptide (NT-proBNP) or brain natriuretic peptide (BNP); (9) TTE parameters, including the cardiac chambers’ cavity sizes, LV diastolic function and left ventricular filling pressures (LVFPs) (measured by the E/A ratio and E/e’ ratio, respectively), biventricular systolic function assessed by left ventricular ejection fraction (LVEF) and tricuspid annular plane systolic excursion (TAPSE), degree of concomitant valvular heart disease and pulmonary hemodynamics; (10) the current medical treatment; and (11) follow-up data (if any). Possible discrepancies between reviewers were resolved through a consensus discussion with the involvement of a third author (G.L.N.), who checked the extracted data to ensure accuracy, completeness and consistency.
2.4. Quality Assessment
Articles included in this systematic review were assessed for the risk of bias using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [13]. The quality rating was independently estimated by two authors (A.S. and G.L.N.). Cohen’s Kappa coefficient was used to measure the level of agreement between the two raters and was calculated using k = (p_o_ − p_e_)/(1 − p_e_), where p_o_ is the relative observed agreement between the raters and p_e_ is the probability of random agreement. Moreover, we used the GRADE methodology to assess the certainty of the body of evidence by outcome and produce an evidence profile and interactive summary of the findings [14].
The PRISMA flow diagram used for identifying the included studies is depicted in Figure 1.
2.5. Statistical Analysis
For continuous variables, summary statistics were calculated using the median (range [min–max]) or mean (SD), whereas for categorical variables, frequency counts (N) or percentages (%) were used as appropriate. Two subgroups of studies that assessed the clinical and echocardiographic data of inpatients vs. outpatients/in-home centenarians were summarized separately using standard descriptive statistics. In addition, in order to account for the heterogeneity of these two subgroups, we performed a two-step subgroup meta-analysis of the outcomes of interest. Specifically, the subgroup analysis was performed using a mixed-effects model (random-effects model within subgroups, fixed-effects model between subgroups). First, the standard errors (SEs) of the effect estimates were calculated using standard formulas for means or proportions. We then pooled effect estimates with their SEs for the inpatients and outpatients/in-home cohorts, and then compared using a z-test. Due to the incomplete data for several clinical and echocardiographic parameters, the comparison between the two subgroups of centenarians was performed for those continuous or categorical parameters that were collected by at least two studies for each sub-group. Two-sided p-values below 0.05 were considered statistically significant. The statistical analysis was performed using Comprehensive Meta-Analysis version 3.0 (Biostat, Englewood, NJ, USA), and the meta-analysis was performed using the R programming language, version 4.3.2 (www.r-project.org/), using the function rma of the (“metafor”) package version 4.6-0.
3. Results
3.1. Clinical Findings
The database searches were run from inception to 11 November 2024 and identified 118 references. The title and abstract phase, performed in duplicate by the screeners A.S. and M.L., saw the exclusion of 100 studies. At the full text stage, the number of studies assessed for eligibility was 18 (15.2%), of which 10 (8.5%) were excluded. The most common reasons for exclusion were the following: studies conducted on centenarians without echocardiographic data (61%), duplicates (15.2%), incomplete clinical data (3.4%) and incomplete TTE data (5.1%). A total of eight studies (6.8%) [15,16,17,18,19,20,21,22] were thus included in this systematic review, totaling 1340 centenarians. The included populations were composed of 37% (3/8) retrospective cohort studies [15,17,21] and 63% (5/8) prospective cohort studies [16,18,19,20,22]. Table 1 summarizes the main findings of the eight studies included in the present systematic review.
The included studies were published between 2007 and 2023. Three studies were performed in the USA; two in Italy; and one each in Spain, Denmark and China. The median age of the centenarians at the echocardiographic assessment was 101.4 years (IQR 100.1–103 years). Females comprised 76.3% of the centenarians (IQR 60–85%). Three studies [19,20,22] analyzed in-home centenarians, two studies [16,17] outpatients and two studies [15,18] inpatients, whereas the remaining study of Perez J et al. [21] analyzed an equal proportion of outpatients and inpatients. Three studies [18,19,22] performed echocardiography by using a Philips CX-50 portable echocardiograph, whereas Perez J et al. [21] used a General Electric (GE) cardiovascular ultrasound system; the remaining studies did not specify the ultrasound system employed for the echocardiographic evaluation of centenarians. Among the included studies, only two authors [16,17] provided follow-up data, whereas the great majority of studies (75% of the total) were primarily focused on the echocardiographic assessment of centenarian hearts at the baseline.
The baseline demographic, anthropometric, clinical and biochemical parameters concerning centenarians collected by the included studies are reported in Table 2.
Overall, the centenarians were predominantly females with a small BSA; with a moderate-to-high prevalence of hypertension; and with low prevalences of smoking, type 2 diabetes and dyslipidemia. The analysis of comorbidities revealed a high comorbidity burden [median CCI 3.7 (IQR 1.8–5.5)] and severe functional impairment [median Katz index 2.1 (IQR 1.1–3.1)]. The physical examinations showed normal median values of both the SBP and DBP and a normal median heart rate. The pooled prevalence of atrial fibrillation (AF) was 26.7%. Information concerning the biochemical parameters and current medical treatment were only provided in a limited number of studies, ranging from 12.5% to 36.5% of the total. Blood test results demonstrated a slightly impaired renal functional reserve, optimal lipid panel and increased serum levels of NT-proBNP/BNP. With regard to the current medical treatment, we commonly found angiotensin-converting enzyme inhibitors (ACEis) or angiotensin receptor blockers (ARBs), followed by diuretics and beta blockers, whereas antiplatelets, anticoagulants, digoxin and statins were administered in less than one-third of the centenarians.
3.2. Transthoracic Echocardiography Findings
Data regarding LV thickness/internal dimensions and LV systolic function were provided by a percentage of studies that ranged from 87.5% to 100% of the total, whereas the remaining echocardiographic parameters were assessed by a number of studies that ranged from 25% to 75% of the total.
Table 3 lists all the conventional echo Doppler parameters obtained by the included studies on the centenarians.
The TTE examination revealed moderate LV hypertrophy with concentric remodeling, mild left atrial (LA) dilatation and a normal right chamber cavity size. The impaired relaxation pattern of the transmitral flow [median E/A ratio 0.8 (IQR 0.7–0.9)] was the most common LV filling pattern detected in centenarians, whereas the LVFPs were moderately increased, as expressed by the E/e’ ratio [median value 16.8 (IQR 16.2–17)]. Seven studies (87.5%) measured the LVEF using the Simpson biplane method, while only Sadiq A et al. [15] used the Teichholz method for calculating the LVEF. Overall, the LVEF [median value 60.9% (IQR 55–84%)] was preserved, while LV systolic dysfunction, defined as LVEF < 50% [23], was detected in 15.8% of the centenarians. Moderate-to-severe aortic stenosis, mitral regurgitation and tricuspid regurgitation were detected in approximately one out of five centenarians. An analysis of the pulmonary hemodynamics showed mild-to-moderate pulmonary hypertension [median systolic pulmonary artery pressure (sPAP) 42.1 mmHg (IQR 37–54 mmHg)]. Finally, the aortic root diameter was slightly increased in comparison with the accepted reference values for healthy individuals aged ≥80 years [24].
In the MILANO study [18], our study group demonstrated a reduced prevalence of echocardiographic congestive signs among hospitalized centenarians. Interestingly, the centenarians were frequently diagnosed with an increased systolic midventricular pressure gradient, likely related to a chronically reduced preload due to chronic dehydration and/or hypovolemia with consequent supra-normal ventricular emptying. Moreover, we measured the arterial elastance index (EaI), LV end-systolic elastance index (EesI) and resultant EaI/EesI ratio (V-A coupling) in the centenarian cohort and compared the results with a group of sex-matched hospitalized octogenarians. The VAC parameters were significantly increased in centenarians vs. octogenarians.
3.3. Subgroup Analysis
Pooled estimates of the principal clinical and echocardiographic variables obtained by the included studies in the two cohorts of inpatients and outpatients/in-home centenarians are reported in Table 4.
The subgroup analysis suggested a slightly lower proportion of females among the hospitalized centenarians compared with the outpatients and in-home centenarians, although this difference was not statistically significant. Moreover, the inpatients showed a higher prevalence of smoking history. The burden of cardiovascular and noncardiovascular comorbidities was similar in the subgroups of centenarians.
Using TTE, the inpatients were diagnosed with a greater degree of LV hypertrophy and a significantly higher E/A ratio and sPAP magnitude compared with the outpatient/in-home cohorts. The LVEF tended to be higher in the hospitalized centenarians than in the non-hospitalized cohorts, even if this increase was not statistically different. Finally, moderate-to-severe aortic regurgitation, mitral regurgitation and tricuspid regurgitation were more frequently detected in the hospitalized centenarians.
3.4. Follow-Up Data
Concerning the follow-up data, Martínez-Sellés M et al. [16] found that roughly half of the population of centenarians had died during the first year of follow-up. Cox regression analysis revealed that age, the Charlson and Katz indexes, systolic dysfunction and severe aortic regurgitation were independent predictors of mortality. The study by Brenes-Salazar JA et al. [17] demonstrated 1-month and 1-year mortalities of 15% and 47%, respectively; the median survival after the echocardiogram was 13 months, independent of management. Accordingly, the authors concluded that echocardiography influenced the medical decision making and management only in a minority of cases, with a minimal impact on the overall care of the centenarians.
3.5. Risk of Bias Assessment
The quality of the included studies was judged to have a low risk of bias for the study of Martínez-Sellés M et al. [16] and fair for the remaining seven studies. The Cohen’s Kappa coefficient for the agreement between the reviewers in the risk of bias assessment was interpreted as a substantial agreement, with k = 0.80.
3.6. GRADE Assessment
The body of evidence regarding the echocardiographic features of centenarians was estimated to be of moderate certainty of the evidence (Table 5).
- Question: echocardiographic studies performed in cohorts of hospitalized and non-hospitalized centenarians for the detection of age-related cardiac remodeling.
- Setting: inpatients, outpatients and in-home centenarians.
4. Discussion
4.1. Main Findings of This Systematic Review
The present systematic review included eight echocardiographic studies conducted on individuals aged ≥100 years over a 16-year period. Our results reveal that the centenarians were mostly females with a small BSA, a long history of hypertension and a slightly impaired renal functional reserve. These had a reduced cardiovascular disease burden with an optimal blood pressure control and lipid profile, but an increased comorbidity burden. The TTE demonstrated LV hypertrophy with first-degree diastolic dysfunction, a moderate increase in LVFPs, normal LV systolic function and mild-to-moderate pulmonary hypertension. LV systolic dysfunction and moderate-to-severe valvular heart diseases were rarely detected. Additionally, our study group [18] demonstrated an increased prevalence of systolic midventricular pressure gradients associated with increased arterial and end-systolic stiffness in hospitalized centenarians.
Compared with the outpatient and in-home cohorts, the hospitalized centenarians were less commonly females and were more likely to be affected by significant LV hypertrophy with supra-normal LVEFs, higher degrees of valvulopathies and impaired pulmonary hemodynamics.
Based on the findings of the two studies that provided follow-up data [16,17], the centenarians had a mortality rate of about 50% over the 1-year follow-up. Advanced age, increased comorbidity burden, LV systolic dysfunction and moderate-to-severe valvular heart diseases were independently associated with mortality in the centenarians.
The included studies demonstrated the high feasibility of TTE, which allowed for a comprehensive evaluation of the centenarians’ cardiac chambers’ sizes, systolic and diastolic functions, valvular performance and hemodynamics. Both the hospitalized and non-hospitalized cohorts of centenarians were diagnosed with a common echocardiographic phenotype of LV hypertrophy, that is, the LV concentric remodeling.
4.2. Pathophysiological Mechanisms Underpinning LV Concentric Remodeling in Centenarians
The LV concentric remodeling detected in centenarians by echocardiography may be considered as the result of several pathophysiological mechanisms (Figure 2).
First, the aging process is itself associated with an increase in RWT and LV concentric remodeling, characterized by progressive myocyte dropout, myocyte hypertrophy and increased collagen concentration, as demonstrated by histomorphometric studies in animals and humans [25,26,27]. Second, female sex is associated with LV concentric remodeling in the general population, irrespective of the burden of cardiovascular risk factors [28,29]. The LV concentric remodeling observed in centenarians may also represent a cardiac adaptation to long-standing arterial hypertension [30] and/or degenerative aortic stenosis [31]. An increased arterial elastance secondary to degeneration and hyperplasia of the arterial wall may also be another cause of increased LV afterload, leading to LV hypertrophy [32,33]. LV concentric remodeling in elderly individuals may also be the phenotypic expression of cardiac senile amyloidosis, an infiltrative cardiomyopathy characterized by extracellular amyloid infiltration throughout the heart [34]. LV hypertrophy in centenarians is associated with a significant increase in myocardial stiffness and abnormalities in diastolic function, including impaired LV relaxation, increased LVFPs, LA remodeling and postcapillary pulmonary hypertension [35,36]. The combined increase in ventricular and arterial stiffening promotes load-induced impairment in LV relaxation, with a consequent increase in the serum levels of NT-proBNP/BNP [37,38].
An analysis of the LV systolic function by TTE showed that the pooled LVEF was preserved in centenarians. However, the subgroup analysis revealed that compared with the outpatient and in-home cohorts, the hospitalized cohorts were more likely to be diagnosed with a supra-normal LVEF (≥65%). The supra-normal LV contractile phenotype is a newly recognized state associated with an unfavorable prognosis, as reported by recent studies conducted on both chronic [39,40] and acute [41,42] heart failure patients. These studies highlighted significant pathophysiological differences between heart failure patients with LVEF 50% to 64% (the “normal” LVEF phenotype) in comparison with those with EF ≥ 65% (the “supra-normal” LVEF phenotype). However, these studies evaluated the prognostic role of a “supra-normal” LVEF, predominantly in middle-aged participants (aged <70 years), without including the “oldest-old” individuals. The results of the present systematic review would confirm that the “normal” LVEF phenotype, commonly detected in non-hospitalized centenarians, is an important clinical predictor of long-term survival. On the other hand, the “supra-normal” LVEF phenotype has been described in hospitalized centenarians with infectious disease related to pulmonary or non-pulmonary infections. The infective process associated with elevated body temperatures and fluid loss is responsible for dehydration, hypovolemia and a reduction in preload, thus causing a hypercontractile response [18]. In this clinical context, TTE generally shows severe LV hypertrophy, a small LV cavity size, severe diastolic dysfunction and a dynamic intraventricular obstruction. The “supra-normal” LVEF phenotype was also recently described in heart failure patients with the “cold-dry” hemodynamic phenotype, a negative prognostic indicator over the mid-term follow-up period [43].
4.3. Implications for Clinical Practice
The progressive increase in both arterial elastance and myocardial stiffness detected in centenarians may result in a decreased exercise tolerance and enhanced load sensitivity [44,45]. Indeed, in patients with stiff noncompliant ventricles, sudden changes in LV afterload or LV preload may cause uncontrolled increases in LVFPs, resulting in pulmonary edema [46]. For these reasons, centenarians are particularly susceptible to heart failure with apreserved ejection fraction (HFpEF) [47,48]. In this regard, TTE may help the clinicians to identify those who are at an increased risk of cardiovascular complications among the oldest-old patients. Additionally, as indicated by the literature data [49,50,51], a comprehensive echocardiographic assessment of cardiac chambers’ cavity sizes, systolic and diastolic function, valvular function and pulmonary hemodynamics might allow the clinicians to select a limited number of elderly individuals who could benefit from interventional procedures.
TTE may also guide the clinicians in selecting and/or uptitrating the most appropriate medical treatment for centenarians. In this regard, the echocardiographic findings of small and stiff cardiac chambers with an intraventricular pressure gradient might suggest the clinicians use beta blockers and ensure adequate volemic filling [52]. Moreover, due to the increased risk of fatal bleeding related to decreased renal function, several comorbidities, coexisting frailty and the risk of falls [53,54,55], antiplatelets and anticoagulants should be used with great caution in this special population.
4.4. Limitations of the Included Studies
The main limitations of the included studies were their monocentric nature, the limited sample size of centenarians examined, the retrospective design of 37% of the total and the lack of follow-up data for 75% of the studies. Moreover, the included studies assessed the cardiac structure and function of the centenarians by evaluating the echocardiographic characteristics of heterogeneous study populations, i.e., inpatients, outpatients and in-home centenarians. Most conventional echocardiographic parameters were measured by a limited number of studies, and innovative echocardiographic data were lacking. In particular, no study measured the myocardial strain parameters using speckle-tracking echocardiography (STE) in the centenarians. Due to the higher sensitivity of LV global longitudinal strain (GLS) than LVEF for detecting subclinical LV systolic dysfunction [56], STE analysis could have provided more information regarding the cardiac performance of the centenarians. Even if centenarians exhibit echocardiographic features suggestive of diastolic dysfunction and LV remodeling, which is commonly associated with susceptibility to HFpEF, a definitive diagnosis of HFpEF, including the presence of heart failure symptoms, was not assessed in the included studies. While diastolic dysfunction and LV remodeling indicate a potential predisposition to HFpEF in centenarians, further research incorporating clinical and longitudinal data is necessary to clarify its prevalence and clinical impact.
5. Conclusions
Centenarians have typical LV concentric remodeling with an increased myocardial stiffness and diastolic dysfunction, making them particularly susceptible to the development of HFpEF.
TTE may allow clinicians to obtain a comprehensive evaluation of both hospitalized and non-hospitalized centenarians by providing a detailed assessment of the cardiac chambers’ sizes, systolic and diastolic functions, valvular performance and hemodynamics.
Medical treatment should be considered for personalized implementation and uptitration in this special population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudnicka E. Napierała P. Podfigurna A. Męczekalski B. Smolarczyk R. Grymowicz M. The World Health Organization (WHO) approach to healthy ageing Maturitas 202013961110.1016/j.maturitas.2020.05.01832747042 PMC 7250103 · doi ↗ · pubmed ↗
- 2European Union Eurostat Ageing Europe—Looking at the Lives of Older People in the EU 2019 th ed.Publications Office Maastricht, The Netherlands 2019
- 3Rabuñal Rey R. Monte Secades R. Rigueiro Veloso M.T. Casariego Vales E.J. Ibáñez Alonso M.D. García Pais M.J. Centenarian patients attended at a general hospital Rev. Clin. Esp.200220232632810.1016/S 0014-2565(02)71067-912093397 · doi ↗ · pubmed ↗
- 4CannatàA. Camparini L. Sinagra G. Giacca M. Loffredo F.S. Pathways for salvage and protection of the heart under stress: Novel routes for cardiac rejuvenation Cardiovasc. Res.201611114215310.1093/cvr/cvw 10627371745 · doi ↗ · pubmed ↗
- 5Cannata A. Merlo M. Artico J. Gentile P. Camparini L. Cristallini J. Porcari A. Loffredo F. Sinagra G. Cardiovascular aging: The unveiled enigma from bench to bedside J. Cardiovasc. Med.20181951752610.2459/JCM.000000000000069430024423 · doi ↗ · pubmed ↗
- 6Klatt E.C. Meyer P.R. Geriatric autopsy pathology in centenarians Arch. Pathol. Lab. Med.19871113673693827543 · pubmed ↗
- 7Andersen-Ranberg K. Schroll M. Jeune B. Healthy centenarians do not exist, but autonomous centenarians do: A population-based study of morbidity among Danish centenarians J. Am. Geriatr. Soc.20014990090810.1046/j.1532-5415.2001.49180.x 11527481 · doi ↗ · pubmed ↗
- 8Berzlanovich A.M. Keil W. Waldhoer T. Sim E. Fasching P. Fazeny-Dörner B. Do centenarians die healthy? An autopsy study J. Gerontol. A Biol. Sci. Med. Sci.20056086286510.1093/gerona/60.7.86216079208 · doi ↗ · pubmed ↗