A retrospective study of zoonotic tuberculosis among livestock farmers of Lahore district using one health approach
Rubab Maqsood, Abdul Rehman, Farhat Nazir Awan, Hamad Bin Rashid, Shakera Sadiq Gill, Chanda Jabeen, Gulshan Umbreen, Rafia Akram, Mamoona Chaudhry

TL;DR
This study explores how tuberculosis spreads between humans and animals among Lahore's livestock farmers, identifying risk factors like keeping animals indoors and smoking.
Contribution
The study identifies specific risk factors for zoonotic TB transmission in Lahore using a One Health approach.
Findings
Keeping animals inside the home and smoking were significant predictors of TB in humans.
Animals of TB cases were more likely to test positive for bovine TB compared to controls.
Unmarried individuals and those over 35 were more likely to have TB.
Abstract
Tuberculosis (TB) affects humans and animals regardless of species type, causing huge economic losses and deaths worldwide. However, the mechanisms and risk factors of zoonotic transmission are not well known in Pakistan. The current study aimed to identify the potential risk factors associated with TB in farmers and their animals, particularly exposure to infected animals in Lahore District, Pakistan. The study consisted of two components utilizing the concept of One Health. In the first component, a retrospective case-control study of human subjects (cases = 25, control = 25) was conducted from December 2021 to July 2022. In the second component, a cross-sectional analysis of the cattle owned by selected participants (TB cases and healthy controls) was completed in the Lahore district. A single intradermal tuberculin skin test was used to determine TB infection in cattle. A total of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1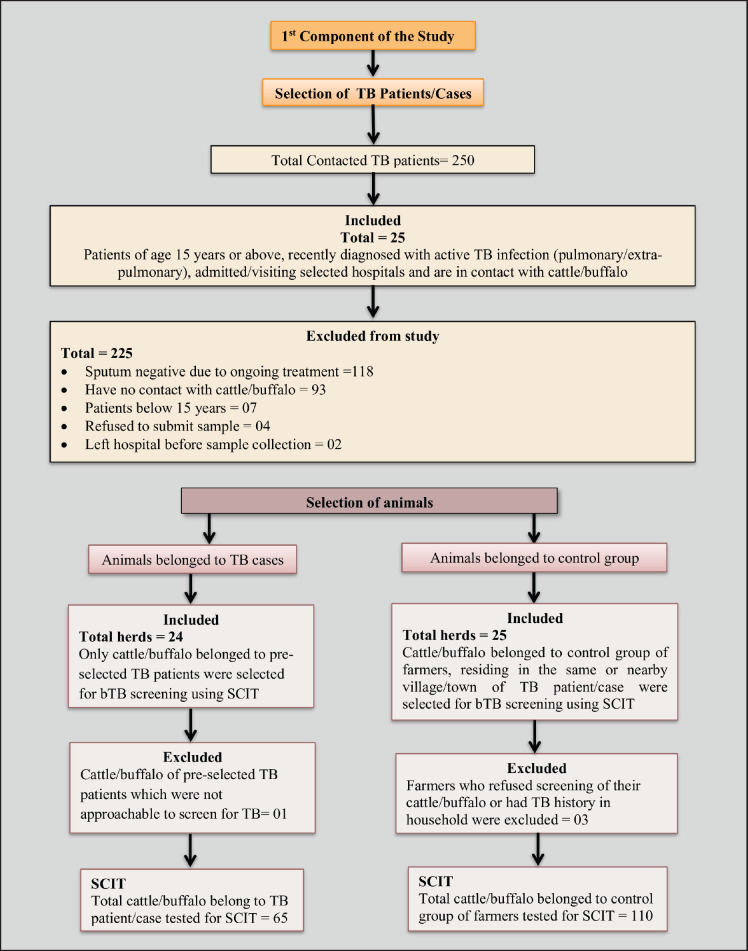 Figure 2
Figure 2| Primers | Amplicon |
|---|---|
| RD9 primers | M. tb: 209bp |
| Factors | Cases/TB patients | Controls/Healthy farmers | Total | OR (95%CI) | |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 20 (80) | 24 (96) | 44 | 0.115 | – |
| Female | 5 (20) | 1 (4) | 6 | ||
| Age | |||||
| ≤35 | 7 (28) | 13 (52) | 21 | 0.070 | – |
| >35 | 18 (72) | 12 (48) | 29 | ||
| Marital status | |||||
| Unmarried | 8 (32) | 2 (8) | 10 | 0.047 | 5.4 (1.18–39.00) |
| Married | 17 (68) | 23 (92) | 40 | ||
| Education | |||||
| Illiterate | 19 (76) | 12 (48) | 31 | 0.045 | 3.4 (1.06–12.16) |
| literate | 6 (24) | 13 (52) | 19 | ||
| livestock farming as an inherited occupation | |||||
| Yes | 18 (72) | 19 (76) | 37 | 0.747 | – |
| No | 7 (28) | 6 (24) | 13 | ||
| Years of farming experience if livestock farming is not an inherited occupation | |||||
| ≤5 years | 3 (42.8) | 3 (50) | 6 | 0.797 | – |
| Above 5 years | 4 (57.2) | 3 (50) | 7 | ||
| Residence | |||||
| Rural | 20 (80) | 19 (76) | 39 | 0.158 | – |
| Urban | 3 (12) | 1 (4) | 4 | ||
| Peri-urban | 2 (8) | 5 (20) | 7 | ||
| Monthly income | |||||
| ≤30 thousand PKR/- | 21 (84) | 12 (48) | 33 | 0.010 | 5.69 (1.61–23.98) |
| >30 thousand PKR/- | 4 (16) | 13 (52) | 17 | ||
| Family type | |||||
| Nuclear | 5 (20) | 4 (16) | 9 | 0.713 | – |
| Joint | 20 (80) | 21 (84) | 41 | ||
| Family size | |||||
| ≤6 | 9 (36) | 10 (40) | 19 | 0.771 | – |
| >6 | 16 (64) | 15 (60) | 31 | ||
| Number of rooms in the house | |||||
| ≤2 | 17 (60) | 14 (56) | 29 | 0.384 | – |
| >2 | 8 (40) | 11 (44) | 21 | ||
| Vaccinated (BCG) against TB in childhood | |||||
| Yes | 10 (40) | 22 (88) | 32 | 0.995 | – |
| No | 2 (8) | 0 | 2 | ||
| Don’t know | 13 (52) | 3 (12) | 16 | ||
| Smoker | |||||
| Yes | 19 (76) | 11 (44) | 30 | 0.024 | 4.03 (1.25–14.37) |
| No | 6 (24) | 14 (56) | 20 | ||
| Meat consumption per week | |||||
| Once and twice | 23 (92) | 19 (76) | 17 | – | – |
| Thrice or more | 2 (8) | 6 (24) | 8 | ||
| Chronic illness other than TB | |||||
| Yes | 4 (16) | 3 (12) | 7 | – | – |
| No | 19 (76) | 21 (84) | 40 | ||
| Don’t know | 2 (8) | 1 (4) | 3 | ||
| Do any of the family members or persons in contact have/had TB? | |||||
| Yes | 9 (36) | 2 (8) | 10 | 0.027 | 6.47 (1.43–46.31) |
| No | 16 (64) | 23 (92) | 40 | ||
| Diagnosed/suffered from TB before this time? | |||||
| Yes | 1 (4) | 0 | 1 | – | – |
| No | 24 (96) | 25 (100) | 49 | ||
| Animal keeping place | |||||
| Inside home | 10 (40) | 2 (8) | 12 | 0.015 | 7.67 (1.72–54.64) |
| Outside home | 15 (60) | 23 (92) | 38 | ||
| No. | Variables | Response | OR | CI (95%) | |
|---|---|---|---|---|---|
| 1 | Gender | Male | 0.01 | (0.0002–0.29) | 0.014 |
| Female | |||||
| 2 | Age | ≤35 | 1.13 | (1.05–1.24) | 0.004 |
| >35 | |||||
| 3 | Marital status | Unmarried | 32.20 | (2.92–819.03) | 0.014 |
| Married | |||||
| 4 | Smoker | Yes | 21.87 | (2.80–395.82) | 0.011 |
| No | |||||
| 5 | Animal keeping place | Inside home | 9.92 | (1.29–134.61) | 0.047 |
| Outside home |
| Factors | TB cases response | % |
|---|---|---|
| Type of TB identified | ||
| Drug sensitive | 24 | 96 |
| Drug-resistant | 1 | 4 |
| Perceived health status according to TB patient | ||
| Satisfactory | 18 | 72 |
| Unsatisfactory | 7 | 28 |
| Chronic cough for more than the last 3 weeks? | ||
| Yes | 24 | 96 |
| No | 1 | 4 |
| Since you feel sick do you have a fever? | ||
| Yes | 21 | 84 |
| No | 4 | 16 |
| Pain in the chest | ||
| Yes | 22 | 88 |
| No | 3 | 12 |
| Coughing up blood or sputum | ||
| Yes | 9 | 36 |
| No | 16 | 64 |
| Weakness or fatigue | ||
| Yes | 24 | 96 |
| No | 1 | 4 |
| Weight loss | ||
| Yes | 21 | 84 |
| No | 4 | 16 |
| Sweating at night | ||
| Yes | 10 | 40 |
| No | 15 | 60 |
| Diarrhea | ||
| Yes | 9 | 36 |
| No | 16 | 64 |
| No. | Variables | OR (95%CI) | |
|---|---|---|---|
| 1 | Animal belonging to | 7.76 (0.79–76.02) | 0.039 |
| TB case group | |||
| Control group | |||
| 2 | Animal age | 2.17 (0.17–116.03) | 0.86 |
| 1–5 years | |||
| >5 years | |||
| 3 | Source of animal in the herd | 0.76 (0.10–5.54) | 0.79 |
| Animal purchased from another herd | |||
| Raised in the same herd | |||
| 4 | Animal milking status | 0.61 (0.06–6.10) | 0.67 |
| Yes | |||
| No |
| Knowledge attitude and practices | TB cases | Controls (healthy farmers) | Total |
|---|---|---|---|
| Can TB affect animals? | |||
| Yes | 4 (16) | 2 (8) | 6 |
| No | 13 (52) | 12 (48) | 25 |
| Don’t know | 8 (32) | 11 (44) | 19 |
| Can you get TB from animals? | |||
| Yes | 4 (16) | 1 (4) | 5 |
| No | 13 (52) | 10 (40) | 23 |
| Don’t know | 8 (32) | 14 (56) | 22 |
| Can cough spray transmit TB? | |||
| Yes | 19 (76) | 18 (72) | 37 |
| No | 5 (20) | 4 (16) | 9 |
| Don’t know | 1 (4) | 3 (12) | 4 |
| Use of facemask or cover face while coughing? | |||
| Yes | 3 (12) | 7 (28) | 10 |
| No | 20 (80) | 7 (28) | 27 |
| Some times | 2 (8) | 11 (44) | 13 |
| Do you think, drinking raw milk can transmit TB? | |||
| Yes | 8 (32) | 10 (40) | 18 |
| No | 14 (56) | 15 (60) | 29 |
| Don’t know | 3 (12) | 0 | 3 |
| Sharing a room with animals can spread TB? | |||
| Yes | 1 (4) | 2 (8) | 3 |
| No | 14 (56) | 12 (48) | 26 |
| Don’t know | 10 (40) | 11 (44) | 21 |
| Do you consume unpasteurized/raw milk? | |||
| Yes | 2 (8) | 0 | 2 |
| No | 15 (60) | 22 (88) | 37 |
| Both | 8 (32) | 3 (12) | 11 |
| Do you wash your hands with soap after working with animals? | |||
| Always | 17 (68) | 18 (72) | 35 |
| No | 5 (20) | 1 (4) | 6 |
| Often | 3 (12) | 6 (24) | 9 |
| House/shed sharing with animals at night or sleeping in pen | |||
| Yes | 21 (84) | 15 (60) | 36 |
| No | 4 (16) | 10 (40) | 14 |
| Separation of sick animals from the rest of the herd | |||
| Yes | 1 (4) | 4 (16) | 5 |
| No | 24 (96) | 21 (84) | 45 |
| Presence of other livestock among bovines | |||
| Yes | 16 (64) | 14 (56) | 30 |
| No | 9 (36) | 11 (44) | 20 |
| Grazing | |||
| Yes | 11 (44) | 7 (28) | 18 |
| No | 14 (56) | 18 (72) | 32 |
| If grazing yes then mixing of animals with other herds during grazing and watering | |||
| Yes | 10 (90.91) | 4 (57.15) | 14 |
| No | 1 (9.09) | 3 (42.85) | 4 |
| Feed offered to animals | |||
| Green fodder | 21 (84) | 20 (80) | 41 |
| Green fodder + concentrate | 4 (16) | 5 (20) | 9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Zoonotic diseases and public health
Introduction
Tuberculosis (TB) has been known as a disease of poverty for decades [1] and is cited among the leading infectious causes of death in humans in the world [2]. Although Mycobacterium tuberculosis and Mycobacterium bovis are closely related members of the Mycobacterium tuberculosis complex (MTBC) and have different host preferences. Humans are assumed to be the reservoir for M. tuberculosis whereas *M. bovis *has a diverse host range but is usually encountered in cattle [3,4].
When TB due to M. bovis is communicated to humans, it is termed zoonotic TB. It is common in developing countries where bovine TB is maintained in domestic and wild animals. Transmission usually happens through inhalation of droplets and drinking of unpasteurized milk from an infected animal. Repeated isolation of M. tuberculosis from domestic animals accentuated its reverse zoonosis potential [5]. *Mycobacterium orygis *is also an MTBC subspecies, and it has been documented as an emergent cause of zoonotic and bovine TB in South Asia [6,7]. Recently, in Lahore, Pakistan, M. orygis and M. tuberculosis were isolated from cattle and buffalo. None of the tested animals had M. bovis [8]. In Lahore, Pakistan, the prevalence of MTBC was observed to be higher among occupationally exposed groups (abattoir workers, livestock farmers, animal handlers, veterinarians, and laboratory workers) [9]. Knowledge of zoonotic TB has evolved in South Asia and several other regions of the world. TB acquired from animals can be termed zoonotic TB [10].
The growing concept of One Health testified to the zoonotic blight of bovine TB. Under end TB strategy, focusing on the diagnosis and treatment of each TB patient, the policy was recently devised as a roadmap for zoonotic TB [11].
The public health system in low- and middle-income countries lacks the differential diagnostic facilities between TB of human or bovine origin due to accessibility and expensive testing techniques [12]. The top five countries with the highest burden of human TB are located in South Asia, and Pakistan is ranked fifth among these [13]. The COVID-19 pandemic has damaged, stalled, or even reversed the End TB program accomplishments, especially in high TB burden countries [14].
This study attempted to determine the risk factors that contribute to the transmission of TB from animals to humans (livestock farmers) and from TB patients to their animals in the Lahore District, Pakistan. The study also seeks knowledge, attitudes, and practices of TB patients and healthy farmers about zoonotic TB.
Materials and Methods
Ethical approval
Office of Research Innovation and Commercialization, University of Veterinary and Animal Sciences, Lahore, found the study per the scientific and ethical requirements and approved with reference No. DR: 56, dated 03-01-2020. Informed consent was obtained from all study participants.
Study site
Lahore is a cosmopolitan city and provincial capital of Punjab with a rapidly growing population of 13 million [15]. About a century old, Mayo Hospital, Gulab Devi Chest Hospital, and Infectious Disease Hospital, located in Lahore city, were selected for the current study (Fig. 1). These hospitals receive referrals for TB and other pulmonary diseases from all over the Punjab province of Pakistan. These hospitals are also implementing the National TB Control Program under the End TB strategy of World Health Organization. Before the COVID-19 pandemic, Mayo and Gulab Devi hospitals were receiving about 40 new TB patients per day, including referrals. While at the infectious disease hospital, the average daily patient number was 5. During the COVID-19 pandemic, the count declined drastically to only 1 or 2 patients per day. During some days of lockdown, hospitals received no patients for TB. We initiated this study in December 2021, when the COVID-19 pandemic impact was waning and the average per-day patient count increased up to 10.
Study design
Ensuring the One Health concept, a case-control study design opted to identify determinants associated with the transmission of TB between humans and their animals in the study area. This study comprised the following components:
A case-control study of TB patients associated with livestock farming;Screening of animals (cattle/buffalo) belonging to TB cases and the control group of farmers;Knowledge attitude and practices (KAP) survey on zoonotic TB.
TB patients admitted to TB wards of the above-mentioned hospitals were contacted from December 2021 to July 2022. The inclusion criteria for TB patients were those aged 15 years or above with active TB (pulmonary/extra-pulmonary) and in contact with cattle or buffalo, admitted to any of the selected hospitals for treatment were selected as cases for this study. The study excluded participants who were under 15 years old, had no contact with livestock, refused to provide sputum samples, or were receiving TB treatment and had a negative sputum test. Every participant in the control group was selected from the same or a nearby village or town where the case group participants were from. The control group participants were also livestock farmers with no prior history of TB diagnosis. Controls were approached with the help of respective Livestock and Dairy Development veterinarians or veterinary assistants. The livestock farmer who consented and volunteered first for sputum submission and animal screening for bovine tuberculosis (bTB) was selected from each locality (Fig. 2).
Only 25 TB patients met the inclusion criteria for cases, i.e., being 15 years old or above, positive with active TB (pulmonary/extra-pulmonary), and in contact with cattle or buffalo. All visits were made to the hospitals during the early hours of the day due to a higher influx of patients for sample submission and admission registration. Upon contacting TB patients, they were explained about the study and acquired consent. Socio-demographic, occupational, and other information related to disease symptoms were collected from all participants who gave consent and met the inclusion criteria of the study. The questionnaire was designed in English and then translated into the national language, Urdu. During formal pre-testing, it was revealed that most of the respondents were illiterate and unable to understand the questions when explained in the Urdu language. To overcome this, the Urdu format was further explicated in the local language, Punjabi.
Location map of hospitals selected for study.
After information was collected, participants were requested to submit a sputum sample the following morning, before eating breakfast. Hospital laboratory staff were requested to carry out the collection of extra-pulmonary samples. All samples were immediately shifted to the Disease Surveillance Laboratory Biosafety level-II in the Department of Epidemiology and Public Health, University of Veterinary and Animal Sciences Lahore, Pakistan, and stored at refrigerated temperature. Matched on a 1:1 ratio, we selected a total of 25 livestock farmers as controls. Information and sputum samples were also collected from control participants.
For the KAP survey, information was collected about knowledge, attitudes, and practices regarding zoonotic TB from all 50 participants (25 = TB cases, 25 = controls) selected for the study. This survey consisted of fourteen questions in total, with six focused on assessing knowledge and four each regarding attitudes and practices.
Selection of risk factors
The risk factors were selected by reviewing the literature [16–18] and were categorized as socio-demographic factors (gender, age, marital status, family size, joint or nuclear families, family sizes, urban or rural residences, educational level, occupation other than livestock farming, and herd size), knowledge about zoonotic TB and livestock farming practices (can farmers get TB from animals, drinking raw milk, sharing the room with the animal at night).
Selection of animals and testing for the second component of the study
To accomplish the second component of this study, all selected TB cases were traced to their villages/towns for tuberculin tests of their animals (cattle and/or buffalo). The animals belonging to the control group were also tested for bTB. A trained veterinarian was designated to administer tuberculin to all animals and measure skin enduration after 72 h following the guidelines of World Organization for Animal Health [19]. A total of 175 animals were subjected to a tuberculin skin test; 65 of these animals were from cases, and 110 belonged to control group members. Animal owners/workers were asked about husbandry practices (grazing, mixing with herds, history of bTB in the herd, separation of sick animals) (Fig. 2).
Flow diagram for study design.
Laboratory testing of human samples
All collected sputum and extra-pulmonary samples were subjected to DNA isolation for molecular detection of mycobacterium. The DNA isolation was performed using the phenol-chloroform-isoamyl alcohol and ethanol precipitation method [20]. A polymerase chain reaction (PCR) was performed to diagnose and differentiate between *M. tuberculosis, M. bovis/M. bovis *bacillus calmette-guerin (BCG), and M. orygis. This assay is a 3-primer PCR that detects the presence or absence of region of difference 9. A ~200 bp fragment is amplified if RD9 is present, and a ~400 bp fragment is amplified if it is absent. *M. tuberculosis *has RD9, and *M. bovis/M. bovis *BCG and *M. orygis *do not [6] (Table 1).
Data analysis
Epidata version 3.1 (available via http://www.epidata.dk) was used to input the questionnaire data. This information was exported to Microsoft Excel (version 2013, Microsoft Office) for statistical processing. Validation of digital data was done by random checking for errors with the hard records. R software (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria) was used for statistical analysis. Farmers who tested positive or negative for TB were the outcome variable in all univariate and multivariate analyses. To investigate the association of various risk factors with the occurrence of zoonotic TB in humans, we conducted a case-control study involving 25 cases and 25 controls. The study employed an unmatched design. The analysis began with a univariate evaluation of each risk factor using logistic regression models, estimating the odds of zoonotic TB based on individual predictors. Variables with a p-value of less than 0.2 were considered for inclusion in the multivariable model.
Subsequently, a multivariable logistic regression model was constructed using a forward selection strategy. The process began with a simple model including one variable and iteratively added predictors based on theoretical relevance and statistical significance. Variables that were not statistically significant in the model were excluded before moving to the next step. This iterative process continued until the most parsimonious model was achieved, capturing the significant predictors of TB occurrence. This systematic approach ensured robustness in identifying associations while minimizing overfitting in the presence of a small sample size. The multicollinearity of predictors in the final model was assessed using the Generalized Variance Inflation Factor (GVIF). GVIF values below 5 are generally considered acceptable. After the model was fitted, the odds ratio and associated 95% confidence intervals (CIs) were calculated. The data collected about the animals’ characteristics were analyzed using Fisher’s exact test. The prevalence of bTB was calculated by using the appropriate formula [21]. For the KAP survey, percentages and crosstabulation were calculated.
Results
Retrospective study
In the first part of the study, 25 out of 250 contacted persons met the inclusion criteria. The control group consisted of 25 individuals. A total of 50 samples (49 sputum samples from TB cases and the control group and 01 extrapulmonary samples) were processed through PCR assays. All 25 samples (TB case group) were PCR positives for M. tuberculosis, but negative for M. bovis and M. orygis. Similarly, none of the sputum samples from the control group of livestock farmers was found positive for any of MTBC.
Among all study subjects (*n = *50), there were only five (10%) females (cases: 4/25, controls: 1/25) and 45 (90%) males. A total of 20 (40%) of participants (cases: 7/25, controls: 13/25) were in the age group of ≤35, while those above 35 years of age were 30 (60%), with 18 in the case and 12 in the control group. Of the participants, 40 (80%) were married, with 17 individuals (68%) in the case group and 23 (92%) in the control group; the remaining 10 (20%) were unmarried. Overall, 31 (62%) participants (cases: 19/25, controls: 14/25) were illiterate without any formal education. Livestock farming was an inherited occupation for 37 (74%) (cases: 18/25, controls: 19/25) of study subjects. About 39 (78%) farmers were living in rural (cases: 20/25, controls: 19/25), seven (14%) in peri-urban (cases: 2/25, controls: 5/25), and four (8%) in urban (cases: 3/25, controls: 1/25) settings (Table 2.).
The average monthly earnings of 33 (66%) participating farmers were ≤30 thousand Pakistani rupees (PKR)/- with a disproportionate distribution among cases (84%, 21/25) and controls (48%, 12/25). Of the participants, 41 (82%) lived in joint family settings, with a comparable distribution to the cases (80%, 20/25) and control farmers (84%, 21/25). Family size of 31 (62%) study participants consisted of >6 individuals (cases: 64%, controls: 60%). The home unit consisted of ≤2 rooms according to 29 (58%) (cases: 17/25, controls: 14/25) participants. Regarding the childhood BCG vaccine, 32 (64 %) (cases: 10/25, controls: 22/25) of subjects responded having been vaccinated, while 16 (32%) (cases: 13/25, controls: 2/25) were non-vaccinated, and two (4%) did not know about their vaccination status. Among the cases, 19 (76%) were smokers, compared to 13 (44% ) in the control group. Compared to the cases (8%, 2/25), the control group had a higher rate of meat availability (three times per week; 24%, 6/25). Four cases had chronic conditions (HIV: 1/25, Hepatitis: 1/25, Diabetes: 2/25) other than TB, while three control individuals also reported having diabetes and hypertension, among other chronic ailments (Table 2).
Among selected participants of the study, nine (36%) TB cases were previously in contact with TB patients in their family/friends, whereas only two (8%) persons in the control group reported contact with TB patients in their family/friends. One individual in the TB case group was suffering from a reoccurrence of TB.
Univariable analysis results for retrospective study on TB cases and controls
In the univariable analysis, several variables demonstrated significant associations with TB in occurrence in cases. Odds ratios greater than one, indicated an increased likelihood of disease occurrence in cases with the presence of these factors. Marital status was significantly associated with TB in cases. Unmarried individuals in the case group were 5.41 (95% CI: 1.18–39.00, *p = *0.047) times more likely to get TB than controls. Education level also showed a significant association, with illiterate participants in cases having a 3.43 (95% CI: 1.06–12.16, *p = *0.045) times higher likelihood of TB than controls. Livestock farmers in the case group with a monthly income of ≤30,000 PKR were 5.69 (95% CI: 1.61–23.98, *p = *0.010) times more likely to have TB compared to those earning more than 30,000 PKR. Cases having a history of contact with TB patients in family/friends were 6.47 (95% CI: 1.43–46.31, *p = *0.027) more likely to have TB than controls. Smokers in the TB case group had times 4.03 (95% CI: 1.25, 14.37, *p = *0.024) higher likelihood of having TB among cases compared to non-smokers. Livestock farmers with TB were 7.67 (95% CI: 1.72–54.64, *p = *0.047) times more likely to keep animals inside the home compared to farmers without TB (controls) (Table 2).
Multivariable analysis
The multivariable logistic regression model identified five significant risk factors for TB among cases. Males in the cases group had substantially lower odds of contracting TB than females, with an odds ratio of 0.01 (95% CI: 0.0002–0.29, *p = *0.014). Participants with ages more than 35 years in the case group were 1.13 (95% CI: 1.05–1.24, *p = *0.004) times more likely to have TB compared to the healthy livestock farmers (controls). Unmarried individuals in the cases were 32.20 (95% CI: 2.92–819.03, *p = *0.014) times more likely to have TB compared to the controls. Smokers in the case group had 21.87 (95% CI: 2.80–395.82, *p = *0.011) times higher likelihood of TB than non-smokers. Livestock farmers with TB were 9.92 times (95% CI: 1.29–134.61, *p = *0.047) more likely to keep animals inside homes than the control (Table 3).
Multicollinearity was checked, and all predictors had GVIF values below 2, with their corresponding adjusted values (GVIF^(1/(2*df))) ranging from 1.10 to 1.42. These results indicate low multicollinearity among the variables included in the model, as GVIF values below 2 indicate minimal concern. Therefore, the stability of the regression coefficients is unlikely to be compromised by collinearity, supporting the reliability of the model’s estimates.
Wider CIs observed in our model likely resulted from a smaller sample size. Further studies with balanced and larger sample sizes can increase the precision.
Characteristics of the TB cases enrolled in the study from the selected TB hospitals
According to the patient history file, one out of the 25 TB cases had a diagnosis of rifampicin-resistant TB. Seven (28%) TB cases had unsatisfactory health status. Chronic cough (96%, 24/25) for more than 3 weeks, fever (84%, (21/25), pain in the chest (88%, 22/25), coughing up blood or sputum (36%, 9/25), weakness or fatigue (96%, 24/25), weight loss (84%, 21/25), sweating at night (40%, 10/25), and diarrhea (36%, 9/25) were the main clinical indications that TB patients narrated (Table 4).
Prevalence of bTB in animals
A total of 172 animals were tested for bTB using the single comparative intradermal tuberculin test (SCIT) test. The number of animals belonging to TB cases was smaller (65) than the number of animals (110) in the control group. There were 3 animals in the case group and one in the control group that tested positive for SCIT. The prevalence of bTB in animals belonging to the case group was 4.6% (95% CI, 1.26–12.58) compared to 0.9% (95% CI, 0.04–4.67) in animals of the control group. Overall prevalence among a total of 175 tested animals was 2.28% (95% CI, 0.77–5.53). The results suggest a higher prevalence of bTB among animals belonging to the TB case group than the animals of the control group.
Risk factors for SCIT-positive test results
The animals belonging to the TB case group were 7.76 (95% CI; 0.79–76.02) times more likely to have positive SCIT tests compared to the animals belonging to the control group of livestock farmers. Animal age, source of animal in the herd, animal milking status, animal pregnancy, and gestation number showed no association with the SCIT-positive status of all the tested animals (Table 5). Further studies with larger sample sizes and molecular diagnostic techniques are needed to draw a definitive conclusion.
KAP survey
Out of 50 farmers surveyed (25 = cases, 25 = controls), 6 (12%) responded that TB affects animals, 25 (50%) said that TB does not affect animals, and 19 (38%) stated that they were unaware of any impact of TB on animals. Of all, 23 (46%) said they cannot get TB from animals; 22 (44%) said they do not know, and 5 (10%) said they can get it from animals. Cough spray can transmit TB, according to 37 (74%) study participants, nine (18%) individuals said no, and four (8%) responded that they did not know. About 20 (80%) of the TB cases were not wearing face masks during coughing and talking to their attendants. Farmers’ response to raw milk consumption and transmission of TB from animals to humans could not be analyzed due to zero cell value in cross tabulation. Of the 50, 35 (70%) (No = 06, ofte*n = *09) stated that they wash their hands with soap after handling animals. Most of the farmers (41; 82%) were offering green fodder to the animals as feed (Table 6). No significant association was found for actors included in the KAP survey.
Discussion
In Pakistan, M. bovis has been reported as the main cause of zoonotic and bTB [22]. Recent studies from Pakistan and South Asia highlighted the changing landscape of bovine and human TB [6,8]. Keeping that in view, the present study aimed to identify the risk factors contributing to TB transmission between animals and humans, specifically among livestock farmers, and from TB patients to their animals in the Lahore District, Pakistan.
The final multivariable logistic regression model identified that males in the cases group were substantially less likely (OR = 0.01, *p = *0.014) to contract TB than females. It has been reported that females were 2.06 times more likely to contract TB in Pakistan [23]. A higher prevalence of TB in females compared to males has been reported in Khyber Pakhtunkhaw, Bajaur and Islamabad, Pakistan [24-26]. Although other studies from different countries reported higher odds ratios and prevalence of TB in males [27,28]. Participants with ages more than 35 years in the case group were more (OR = 1.13, *p = *0.004) likely to have TB compared to the healthy controls. The highest TB notification rates worldwide occur among those aged 45–55, with a marked increase in the age group of >65 years [29,30]. There could be some underlying factors like age-related changes in immunity, comorbidity, and lifestyle that can contribute to the development of TB [31].
Unmarried individuals in the cases were (OR = 32.20, *p = *0.014) more likely to have TB compared to the controls. TB is viewed as a social stigma in Pakistan; TB patients of both genders perceive this disease can compromise their marriageability [32]. In some other countries in South Asia, TB has been a social stigma and a hurdle in getting married and also impacts married life [33]. A study from Pakistan reported that subjects with single marital status are 11.1 times more likely to have multi-drug-resistant TB [34]. Smokers in the case group had (OR = 21.87, *p = *0.011) a higher likelihood of TB than non-smokers. A study in Indonesia reported that smokers are 3.34 times more likely to get TB [35]. Smokers are twice as likely to develop TB than nonsmokers. Smoking over time can alter lung function, increasing the risk of developing TB [36]. Livestock farmers with TB were (OR = 9.92, *p = *0.047) more likely to keep animals inside their homes than the control group. Univariable analysis showed that TB cases had less income (OR = 5.69, *p = *0.010) than controls. They might not have enough money and land to build a separate animal shed.
Data analysis showed that the animals belonging to TB cases were 7.76 (*p = *0.039) times more likely to have a positive tuberculin test than the animals belonging to the control group. It has been reported that cattle owned by TB farmers had three times higher tuberculin positivity compared to cattle owned by farmers without active TB [37]. The presence of TB patients and keeping animals inside the household was reported as a risk factor for animals getting infected with M. tuberculosis [38]. Different studies have documented that cattle can contract M. tuberculosis from farmers and farm workers due to close contact [39–41]. A recent study on cattle and buffalos slaughtered in a slaughterhouse in Lahore reported *M. orygis *and M. tuberculosis as the primary cause of bTB. No animal was found positive for *M. bovis *[8].
In this study, differential PCR testing showed that none of the TB cases were found positive for *M. bovis *or M. orygis. Keeping in view all statistical results, TB among cases due to *M. tuberculosis *might have occurred due to other predisposing factors. Though spillover of M. tuberculosis from active TB cases to their animals could be a plausible event, this study could not provide strong evidence for direct transmission of TB from the cases to their animals and vice versa.
Observed symptoms among TB cases were cough for more than 3 weeks (96%), fatigue (96%), fever, and weight loss (84%), which were aligned with the commonly reported symptoms associated with pulmonary TB [42].
This study’s cases were only selected from government hospitals, which might not be representative, as people with high socioeconomic status prefer to visit private hospitals and clinics. Other limitations of this study are the small sample size and unmeasured confounding. Contrary to the human subjects in the study, we had to rely only on tuberculin tests to diagnose TB in animals.
Conclusion
Gender, age, marital status, illiteracy, low income, smoking, and keeping animals indoors were significant risk factors for TB among farmers, suggesting socioeconomic status plays a crucial role in TB transmission. While no evidence of zoonotic transmission was found, high tuberculin positivity in animals exposed to TB patients raises concerns about potential reverse zoonosis. A study with an increased sample size using molecular diagnosis in both animals and humans can help in a better understanding of the transmission of TB in humans and animals and their relatedness to the host. The study also underscores the role of livestock management practices, such as keeping animals inside households, as a potential risk factor for TB transmission. These findings emphasize the need for integrated human-animal health programs to address zoonotic TB.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shete PB Reid M Goosby E Message to world leaders: we cannot end tuberculosis without addressing the social and economic burden of the disease Lancet Glob Health 2018612 e 12723 https://doi.org/10.1016/S 2214-109X(18)30378-43022428810.1016/S 2214-109X(18)30378-4 · doi ↗ · pubmed ↗
- 2Mac Neil A Global epidemiology of tuberculosis and progress toward achieving global targets — 2017 Morb Mortal Wkly Rep 201968112636 https://doi.org/10.15585/mmwr.mm 6811 a 310.15585/mmwr.mm 6811 a 3PMC 647806030897077 · doi ↗ · pubmed ↗
- 3Allen AR One bacillus to rule them all? – investigating broad range host adaptation in Mycobacterium bovis J Mol Epidemiol Evol Genet Infect Dis 2017536876 https://doi.org/10.1016/j.meegid.2017.04.01810.1016/j.meegid.2017.04.01828434972 · doi ↗ · pubmed ↗
- 4Kanipe C Palmer MV Mycobacterium bovis and you: a comprehensive look at the bacteria, its similarities to Mycobacterium tuberculosis, and its relationship with human disease Tuberculosis (Edinburgh, Scotland)2020125102006 https://doi.org/10.1016/j.tube.2020.1020063303209310.1016/j.tube.2020.102006 · doi ↗ · pubmed ↗
- 5Refaya AK Bhargavi G Mathew NC Rajendran A Krishnamoorthy R Swaminathan S A review on bovine tuberculosis in India Tuberculosis (Edinburgh, Scotland)2020122101923 https://doi.org/10.1016/j.tube.2020.1019233227523410.1016/j.tube.2020.101923 · doi ↗ · pubmed ↗
- 6Duffy SC Srinivasan S Schilling MA Stuber T Danchuk SN Michael JS Reconsidering Mycobacterium bovis as a proxy for zoonotic tuberculosis: a molecular epidemiological surveillance study Lancet Microbe 202012 e 66e 73https://doi.org/10.1016/S 2666-5247(20)30038-03264274210.1016/S 2666-5247(20)30038-0PMC 7325494 · doi ↗ · pubmed ↗
- 7Kock R Michel AL Yeboah-Manu D Azhar EI Torrelles JB Cadmus SI Zoonotic tuberculosis - the changing landscape Int J Infect Dis 2021113 S 6872 https://doi.org/10.1016/j.ijid.2021.02.0913371381210.1016/j.ijid.2021.02.091PMC 8672060 · doi ↗ · pubmed ↗
- 8Maqsood R Duffy SC Bin Rashid H Gill SS Jabeen C Arshad N Molecular detection and characterization of the Mycobacterium tuberculosis complex subspecies responsible for bovine tuberculosis in Punjab, Pakistan Microbiol Spect 2024122 e 0269223 https://doi.org/10.1128/spectrum.02692-2310.1128/spectrum.02692-23PMC 1084616738226805 · doi ↗ · pubmed ↗