Lower Levels of TAZ Expression Associated with Post-Surgical Wound Healing Complications in Soft Tissue Sarcoma Patients Treated with Preoperative Radiation
Jacob D. Gylten, Jane E. Persons, Benjamin J. Miller, Qiang An, Munir R. Tanas, Stephanie J. T. Chen

TL;DR
Lower TAZ levels in irradiated skin of soft tissue sarcoma patients may be linked to wound healing complications after surgery.
Contribution
The study identifies TAZ as a potential biomarker for predicting wound healing complications in patients receiving preoperative radiation.
Findings
Irradiated skin showed lower vessel density and absence of hair follicles and sebaceous glands.
Patients with wound healing complications had lower TAZ levels in irradiated skin compared to those without complications.
Higher TAZ levels in irradiated skin may represent an injury response, but lower levels could contribute to complications.
Abstract
Background/Objectives: Pre-operative radiation (Pre-RT) decreases local recurrence following soft tissue sarcoma (STS) resection but carries the risk of wound healing complications (WHCs). This study evaluated skin specimens and clinical characteristics of STS patients to (1) compare patients with and without Pre-RT, (2) compare Pre-RT patients with and without WHCs, and (3) explore associations between clinical characteristics and WHCs. Methods: This retrospective study included 54 adults who underwent STS resection with primary closure (Pre-RT n = 30). A pathologist who was blinded to the clinical outcomes evaluated the skin specimens microscopically. Results: Irradiated skin had lower vessel density and was more likely to lack hair follicles and sebaceous glands, consistent with the effects of radiation. Irradiated skin was also more likely to include plasma cells. Irradiated skin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
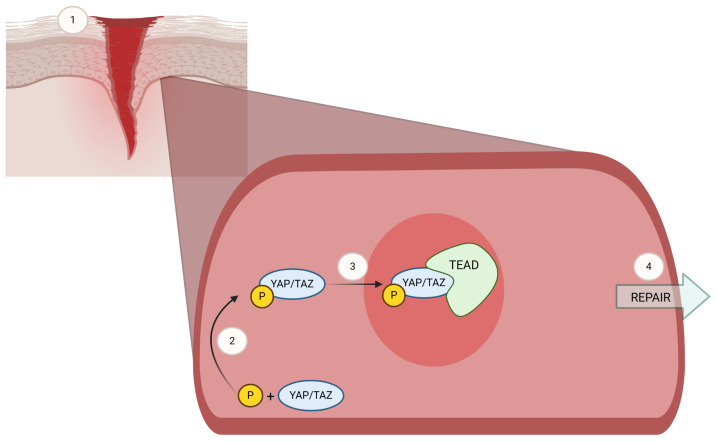 Figure 1
Figure 1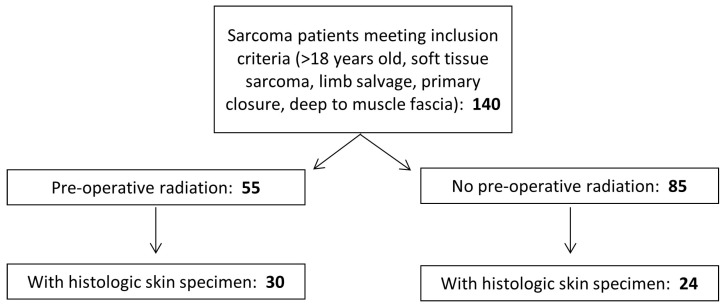 Figure 2
Figure 2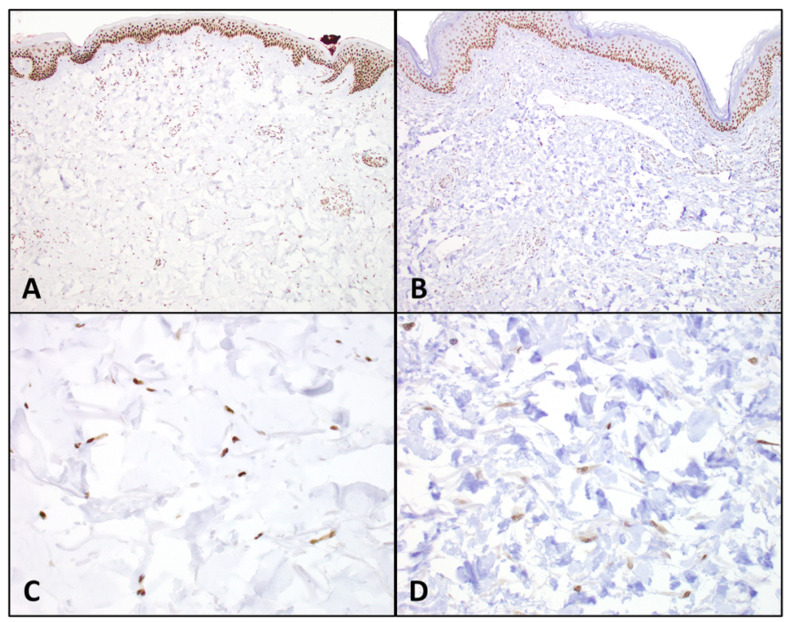 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHippo pathway signaling and YAP/TAZ · Wound Healing and Treatments · Sarcoma Diagnosis and Treatment
1. Introduction
Soft tissue sarcoma (STS) includes a heterogeneous group of mesenchymal malignancies defined by the tissue of origin. STS frequently presents in the extremities as a slow-growing, painless mass [1]. Although STS accounts for only 1% of adult cancers [2], it is of concern due to its propensity for metastasis, local invasion, and recurrence. Due to its rarity and harmless progression, detection can often be delayed until patients present to specialty sarcoma centers after the tumor has already become large and invasive. STS resection morbidity, due to large incisions, postoperative dead space, thin skin-flaps, and resection of neighboring structures invaded by tumors, contributes to a high incidence of acute postoperative wound healing complications (WHCs), including infection, necrosis, dehiscence, and hematoma [3,4]. Acute WHCs represent a significant burden on the healthcare system and can require more intensive wound care, repeat surgeries, and even hospital admissions in some cases.
Previously, amputation was the mainstay of extremity STS management; today, limbs can often be salvaged due to advances in systemic therapy and, primarily, radiation. The addition of radiation is associated with improved long-term survival and decreased tumor recurrence in high-grade STS [5]. The ideal timing of preoperative or postoperative radiation therapy has been somewhat controversial [6]. Preoperative radiation therapy (Pre-RT) is the preferred radiation supplement to STS resection in the US [7]. It improves the chance of achieving negative resection margins by inducing tumor necrosis (particularly at the tumor edges) and enables the administration of lower doses of radiation, which limits exposure of healthy tissue and decreases the long-term side effects of radiation when compared to postoperative delivery.
While limb-salvage surgery with either Pre-RT or Post-RT results in improved survival rates compared to amputation or limb-sparing surgery alone [8], considerable side effects and postoperative complications remain with perioperative radiation treatment. One third of patients undergoing Pre-RT develop acute WHCs, nearly double the rate of patients treated with Post-RT [9]. In contrast, Post-RT patients are more likely to experience chronic complications, including joint fibrosis, immobility, fracture, and edema [10]. The decision between Pre-RT and Post-RT is highly nuanced, requiring consideration of multiple patient characteristics, including patient age, tumor location, tumor size, and patient comorbidities. Although acute WHCs following Pre-RT are treatable and more likely to resolve than the chronic complications that accompany Post-RT, acute WHCs are a frequent burden and thus an important focus of investigation.
In STS, patients treated with Pre-RT tend to develop WHCs associated with diabetes, tumor size, proximity to skin surface, lower-extremity tumor location, increased age, and higher BMI [11,12], which are mostly unavoidable factors. Multiple studies have attempted to identify and address modifiable risk factors to prevent WHCs for STS patients. These include prophylactic antibiotic administration [13], the use of vacuum-assisted closure devices [14], measuring the transcutaneous oxygen levels during the Pre-RT to surgery interval to guide the timing of surgical intervention [15], and adjustments of the NCCN-preferred 3- to 6-week interval between Pre-RT and surgery [7,16,17]. Although these efforts have been valuable, investigations into approaches to prevent WHCs for STS patients have overall been limited, too varied among studies, or yet to translate clinically.
Skin changes following radiation are an important focal point in the STS population treated with Pre-RT because of the potential implications for wound healing. In general, cutaneous repair and healing are attained through the complex and continuous steps of hemostasis, inflammation, proliferation, and remodeling [18,19]. WHCs result when these steps malfunction or fail to transition smoothly. While radiation-induced cutaneous changes including dermatitis, fibrosis, prolonged inflammation, and increased pro-inflammatory mediators are expected obstacles to healing in STS patients, the body of orthopedic and sarcoma literature contains few studies on derangements in these processes at the cellular level [20,21]. It is reasonable to conclude that more detailed analysis of the skin itself and the changes it undergoes following Pre-RT could highlight underlying pathologic processes in wound healing, in turn offering insight into the efforts to decrease WHCs.
A molecular marker of recent interest in both wound healing and STS is the transcriptional coactivator with PDZ-binding motif (TAZ). TAZ and its paralog Yes-associated-protein (YAP) independently combine with the TEAD (TEA domain) family of transcription factors to function as transcriptional regulators of the cell cycle. This is one of the final steps in the complex and only partially understood Hippo pathway, which is responsible for regulating cellular proliferation and tissue regeneration [22]. Walko et al. demonstrated nuclear localization of YAP–TEAD at the leading edge of migrating fibroblasts and basal cells of the epidermis during wound healing [23]. TAZ migration from the cytoplasm of non-injured tissue to the nucleus of injured tissue (Figure 1) is apparent in the epidermis, dermis, and hair follicles [22]. While the role of TAZ has been studied in normal tissue homeostasis, growth, and cutaneous wound healing, its behavior following radiation in STS patients is not yet fully understood. Moreover, YAP and TAZ activation have also been demonstrated in sarcomas [24,25,26,27]. Nuclear staining (activation) has been demonstrated in various sarcomas for both TAZ (33–66% of examined sarcomas) and YAP (50–53% of examined sarcomas) [24,28]. The activation of TAZ and YAP in these diseases has made these proteins an exploitable therapeutic target, with prior studies demonstrating efficacy in pharmacological inhibition of this pathway [26,29,30]. Thus, in STS patients, YAP and TAZ have multiple conflicting roles, being involved in oncogenesis, wound healing, and therapeutics.
To our knowledge, histologic examination and TAZ immunohistochemical analysis of skin following Pre-RT have yet to be evaluated in the context of WHCs following STS resection. Studying these features could provide an avenue to predict WHCs in this patient population, highlight the underlying processes of wound healing disorders, and potentially generate new opportunities for intervention.
The purpose of this study was to evaluate the histologic and clinical characteristics in patients who underwent surgical treatment for STS. First, the effects of Pre-RT were assessed by comparing the histologic and immunohistochemical findings in skin from patients with and without Pre-RT. Second, within the Pre-RT cohort, the histologic and immunohistochemical findings were compared between those patients who did and did not develop WHCs. Third, associations between the WHCs and clinical characteristics related to the patient, tumor, and treatment modality were explored.
2. Materials and Methods
This University of Iowa Institutional Review Board (IRB # 201403755)-approved retrospective study includes 54 adult patients with STS following limb-salvage resection with primary closure. The exposed group was defined as patients who received Pre-RT (n = 30) and the comparison group was defined as patients who did not receive Pre-RT prior to resection (n = 24).
2.1. Selection Criteria
Patients were identified from a pool of 140 patients who underwent resection of pelvic or extremity STS at the University of Iowa Hospitals and Clinics (UIHC) from 2011 to 2019 and met inclusion criteria (>18 years old, primary STS, limb-salvage resection, primary closure, and tumor deep to muscle fascia) (Figure 2). Tissue was obtained through the usual course of diagnosis and treatment.
2.2. Histologic Analysis
When available, archived hematoxylin and eosin (H&E)-stained slides from surgical resection specimens were reviewed for patients meeting initial inclusion criteria. These 4-micron-thick tissue sections were cut from formalin-fixed paraffin-embedded (FFPE) tissue blocks prepared using standard protocols in the UIHC clinical pathology laboratory during routine diagnosis. Skin was included with surgical resection specimens from 61 of the initial 140 patients who met inclusion criteria. Full-thickness skin specimens adequate for study inclusion were those possessing a complete epidermis, dermis, and at least a focally identifiable hypodermis (to ensure proper assessment of dermal thickness). Skin with biopsy site changes or scar was excluded from analysis. When H&E-stained slides were unavailable, archived FFPE tissue blocks were used to prepare 4-micron-thick H&E-stained sections in the Histology Research Laboratory (HRL) at the UIHC using standard protocols. Of the 61 resections with skin, FFPE tissue blocks were available for 54 patients, who comprise the final study sample.
Histopathologic examination was performed by a board-certified pathologist with fellowship training in dermatopathology, who was blinded to all clinical parameters. Tissue specimens were histologically evaluated for inflammation, dermal thickness, vessel density, elastin organization, and dermal fibroblast expression of TAZ.
Inflammation, dermal thickness, and vessel density were evaluated using H&E-stained slides. Inflammation was assessed via multiple modalities: location, percent involvement, cell type, and cell count. Location of the inflammation was captured as perivascular, periadnexal, interstitial, intraepidermal, and/or interface. Percent involvement was defined as the estimated percent of the total epidermal and dermal area involved regarding inflammation. Cell type was noted as the presence or absence of lymphocytes, histiocytes, neutrophils, plasma cells, eosinophils, and multinucleated giant cells. Inflammatory cell count was defined as the number of inflammatory cells within the most cellular field at 400× magnification. Representative dermal thickness was measured microscopically to the nearest 0.5 mm, from the dermal–epidermal junction to the superficial-most aspect of the hypodermis (adipose). Vessel density was captured as the number of vessels in cross-section per ten random fields at 400× magnification.
Elastin fiber organization was evaluated using elastic trichrome staining. Elastic trichrome stains for each specimen were prepared in the HRL using standard protocols and FFPE tissue blocks. Elastin fiber organization was evaluated as previously described by Kung et al., who used the Verhoeff–van Gieson stain (a comparable elastic tissue fiber stain) to evaluate skin in a cohort of patients treated with post-mastectomy radiation [32]. These authors described scoring elastin fiber disorganization on a scale of 0 to 3 as follows: 0 for normal elastin fiber organization, 1 for mild disorganization (>0 to ≤25% disorganized), 2 for moderate disorganization (>25 to ≤50% disorganized), and 3 for severe disorganization (>50% disorganized).
2.3. Immunohistochemical Staining
Immunohistochemical staining for TAZ was also performed for each specimen using FFPE tissue blocks and anti-TAZ antibody (mouse monoclonal 1H9; catalog #LS-C173295; 1:50 primary dilution) obtained from LifeSpan BioSciences (Seattle, WA, USA). Dermal fibroblast nuclei were evaluated for TAZ expression using endothelial cells in dermal blood vessels as an internal control. Staining intensity was classified as 3+ (strong, equivalent to endothelial cell intensity), 2+ (moderate), or 1+ (weak) (Figure 3). The percentages of fibroblast staining at primary and secondary intensities were recorded. TAZ expression was quantified using H-scores (intensity * percentages of fibroblast staining at that intensity). H-scores were determined for the primary and secondary staining intensities. The sum of these primary and secondary H-scores represented the total H-score for each patient.
2.4. Clinical Data Abstraction
Lastly, clinical characteristics relating to patient (age and sex), tumor (size, grade, and location), and treatment (radiation and neoadjuvant chemotherapy) were evaluated in relation to WHCs. A WHC was defined as any skin condition requiring an invasive secondary surgery, readmission, or complex wound management directly related to the primary resection. This included infection, necrosis, hematoma, and prolonged dressing changes occurring within 4 months of the primary surgery. Skin grafts, but not rotational muscle flaps, were an exclusion criterion as to isolate native skin healing after surgery.
2.5. Statistical Analysis
Comparisons were performed using chi-squared and Fisher’s Exact tests for categorical bivariate measures of association and Wilcoxon Rank Sum for continuous variables in group comparison. In primary models, logistic regression analysis was used to (1) compare patients with and without Pre-RT, (2) compare patients with and without WHCs within the subset of patients who received Pre-RT, and (3) explore associations between clinical characteristics and the development of WHCs. Haldane–Anscombe correction was used for calculating odds ratios. Significance was set at the alpha = 0.05 level. All statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
3. Results
The first aim was to compare patients with and without Pre-RT (Table 1). The mean TAZ H-scores were significantly higher among the patients with Pre-RT (276.5 ± 38.8 vs. 253.9 ± 48.5; p = 0.017). In addition, plasma cells were more frequently present in radiated skin than non-radiated skin (p = 0.026). Radiated skin was also more likely to have an absence of hair follicles (p = 0.015) and sebaceous glands (p = 0.016), and to demonstrate lower vessel density (p = 0.041). Logistic regression was performed to calculate the odds of these statistically significant features occurring in patients with and without Pre-RT. Those patients who received Pre-RT had increased odds of having a skin specimen that included plasma cells (OR 28.9, 95% CI 1.5–553.4), lacked sebaceous glands (OR 11.9, 95% CI 1.4–105.3), lacked hair follicles (OR 4.3, 95% CI 1.1–31.0), and had lower blood vessel density (OR 5.8, 95% CI 1.3–14.7).
The second aim was to compare patients with and without WHCs within the subset of patients who received Pre-RT (Table 2). Those patients with WHCs had significantly lower mean TAZ H-scores than the patients without WHCs (260.0 ± 57.3 versus 282.5 ± 29.0; p = 0.040). The Pre-RT patients with WHCs also trended toward more organized elastin, more frequent presence of neutrophils and hair follicles, and lower concentrations of inflammatory cells; however, none of these findings were statistically significant.
The third aim was to explore potential associations between the clinical characteristics and WHCs. The clinical characteristics of patient, tumor, and treatment details were not significantly associated with WHCs within the full cohort (Table 3) or within the subset of patients who received Pre-RT (Table 4).
4. Discussion
The primary goal of this study was to assess an extensive panel of histologic characteristics and TAZ immunohistochemical expression in STS patient skin treated with Pre-RT given their predisposition toward WHCs. The results demonstrate an association between Pre-RT and the absence of hair follicles and sebaceous glands, decreased vessel density, and presence of cutaneous plasma cells. The adnexal and vascular changes are consistent with what would be expected following radiation. The most novel findings, however, center around TAZ expression.
The current study demonstrates increased TAZ expression in irradiated skin overall, with lower levels of TAZ expression in irradiated skin associated with the development of WHCs. Previous animal models and human cell cultures display TAZ nuclear localization in early cutaneous wound healing and suggest that loss of TAZ may impair wound healing [22,31]. The removal of YAP and TAZ via siRNA interference in mice with full-thickness dermal wounds resulted in lowered expression of TGF-beta-1 signaling pathway components, which implies that YAP and TAZ may modulate their expression and subsequently influence wound healing [22]. The modulation of TGF-beta is important for fibroblast migration, extracellular matrix deposition (e.g., elastin), epithelial healing, and the recruitment of inflammatory cells such as neutrophils and macrophages [33]. Radiation-induced fibrosis has also been shown to be mediated by TGF-beta-1 [34]. It seems that altered expression of TGF-beta-1 may interfere with wound healing since modulating the TAZ–TEAD complex has been shown to have an impact on its expression and wound healing. In the Pre-RT patient cohort, the increased TAZ expression may reflect a healing response to radiation injury. Furthermore, in the irradiated patients who later developed WHCs, the healing response may have been inadequate, as represented by their lower TAZ H-scores relative to those irradiated patients who did not develop WHCs.
TAZ is also involved in proper angiogenesis. Kim and colleagues showed that mouse endothelial cell knockdown of both YAP and TAZ together resulted in phenotypic endothelial cell alterations, disrupted barrier function, and delayed sprouting angiogenesis. The knockdown of YAP or TAZ alone in the retina showed much less affected endothelial cell development, suggesting somewhat redundant roles of YAP and TAZ in angiogenesis and vessel integrity [35]. In the current study, the patients with Pre-RT demonstrated both increased TAZ expression and decreased vascularity. It is possible that, in this group, any TAZ-associated increase in vascularity may have been obscured by accompanying decreases in vascularity that are characteristically expected in irradiated skin. The demonstration of higher TAZ H-scores among the patients with Pre-RT supports the reported importance of this protein in healing, but it alone may be inadequate for angiogenesis in the context of irradiated skin.
A trend toward increased neutrophil frequency was observed in those patients with WHCs, but it was not statistically significant. This supports a connection between prolonged inflammation and WHCs despite the lack of this trend in the overall inflammatory cell count. Although neutrophils are helpful in early wound healing, their persistence can contribute to non-healing wounds through continued release of reactive oxygen species, degradative enzymes, and pro-inflammatory mediators, which are risk factors for skin damage [18,36].
The decreased hair follicles and sebaceous glands in the skin of irradiated patients in this study are consistent with previous descriptions of irradiated skin and radiation dermatitis [37]. Keratinocytes from the pilosebaceous units, along with eccrine glands, contribute to re-epithelialization in skin wounds [18,38], but their decrease in the irradiated patients of this study did not translate to an association with more WHCs. This may suggest that factors other than a reduced capacity for re-epithelialization play a significant role in WHCs.
Two findings in the current study appear to be contrary to the limited applicable published literature. First, the skin samples in the patients who received Pre-RT did not demonstrate greater elastin disorganization than those who had no Pre-RT, in contrast to what has been reported previously by Kung et al. However, those authors reported peak elastin fiber disorganization at around 4 months [32]. The shorter interval of less than 6 weeks from the last radiation dose to surgery in the current study may not have allowed time for elastin fiber disorganization to completely develop and reproduce this finding. Further, the results of this study of patients with breast radiation may not be generalizable to skin of other anatomic sites. Secondly, although an irradiated mouse model showed significantly increased dermal thickness at 4 and 12 weeks post-irradiation when compared with the controls [37], the dermal thickness did not differ between the irradiated and non-irradiated patients in the current study. We also observed no difference in dermal thickness between irradiated patients with or without WHCs.
One difficult-to-explain finding is that the skin samples in those patients who received Pre-RT were more likely to contain plasma cells than the skin samples in patients who did not receive radiation. To our knowledge, plasma cells have not been explicitly described in cutaneous infiltrates following radiation. However, a study of human and murine skin demonstrated the development of a plasma-cell-supportive microenvironment and the resultant accumulation of a large number of plasma cells secreting IgM in response to chronic inflammation [39]. It is also well known that plasma cells are more prevalent at certain anatomic sites, particularly the head and neck and anogenital regions [40]. These may represent possible explanations for this finding, but its overall significance is uncertain.
The clinical characteristics in this study had no significant associations with WHCs. This is likely due to the relatively low numbers and heterogeneity of the sample population, a common limitation in studies investigating sarcoma, as the observed factors (e.g., age and tumor location) have shown significance in larger studies [11]. Despite observing no WHCs in those patients with an upper extremity tumor location or tumor size of less than 5 cm, the small cohort size limits the statistical power behind those findings. Although the sample size is a limitation of this study, an important strength is that it was conducted at the University of Iowa Hospitals and Clinics, one of only several sarcoma centers in the US. Future studies may consider recruiting at the national level to increase their sample size.
Given the importance of TAZ in wound healing, it is interesting that cases with significantly lower TAZ H-scores experienced WHCs. TAZ’s location downstream of several signal transduction pathways, conserved expression in various tissues, and interactions with other cellular mediators are factors that contribute to its importance in skin healing. An additional consideration is that interventions targeting TAZ with the intent of limiting tumor growth or metastasis may have an unintended consequence of wound healing compromise. Although the TAZ H-score differences in this cohort are not discriminative enough to be a stand-alone predictor of WHCs, future studies should conduct a more focused evaluation of TAZ expression levels in STS resections with Pre-RT as they may help to predict WHCs when used in combination with other histologic factors and could suggest a therapeutic target.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lawrence W.Jr. Donegan W.L. Natarajan N. Mettlin C. Beart R. Winchester D. Adult soft tissue sarcomas. A pattern of care survey of the American College of Surgeons Ann. Surg.198720534935910.1097/00000658-198704000-000033566372 PMC 1492738 · doi ↗ · pubmed ↗
- 2Morrison B. Soft tissue sarcomas of the extremities Proc. (Bayl Univ. Med. Cent.)20031628529010.1080/08998280.2003.1192791516278699 PMC 1200782 · doi ↗ · pubmed ↗
- 3Nakamura T. Matsumine A. Matsubara T. Asanuma K. Uchida A. Sudo A. Clinical characteristics of patients with large and deep soft tissue sarcomas Oncol. Lett.20151084184410.3892/ol.2015.328926622580 PMC 4509109 · doi ↗ · pubmed ↗
- 4Sanniec K.J. Swanson S. Casey W.J.3rd Schwartz A. Bryant L. Rebecca A.M. Predictive factors of wound complications after sarcoma resection requiring plastic surgeon involvement Ann. Plast. Surg.20137128328510.1097/SAP.0b 013e 31827 c 797323817460 · doi ↗ · pubmed ↗
- 5Koshy M. Rich S.E. Mohiuddin M.M. Improved survival with radiation therapy in high-grade soft tissue sarcomas of the extremities: A SEER analysis Int. J. Radiat. Oncol. Biol. Phys.20107720320910.1016/j.ijrobp.2009.04.05119679403 PMC 3812813 · doi ↗ · pubmed ↗
- 6Hoefkens F. Dehandschutter C. Somville J. Meijnders P. Van Gestel D. Soft tissue sarcoma of the extremities: Pending questions on surgery and radiotherapy Radiat. Oncol.20161113610.1186/s 13014-016-0668-927733179 PMC 5062836 · doi ↗ · pubmed ↗
- 7National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology: Soft Tissue Sarcoma: Version 2.2021—28 April 2021 Available online: https://www.nccn.org/guidelines/guidelines-with-evidence-blocks(accessed on 15 December 2021)
- 8Ramey S.J. Yechieli R. Zhao W. Kodiyan J. Asher D. Chinea F.M. Patel V. Reis I.M. Wang L. Wilky B.A. Limb-sparing surgery plus radiotherapy results in superior survival: An analysis of patients with high-grade, extremity soft-tissue sarcoma from the NCDB and SEER Cancer Med.201874228423910.1002/cam 4.162530030882 PMC 6144142 · doi ↗ · pubmed ↗