Midkine Serum Levels in Inflammatory and Non-Inflammatory Dilated Cardiomyopathy
Ulrich Grabmaier, Bartolo Ferraro, Kristin Lehnert, Astrid Petersmann, Stephan B. Felix, Ludwig T. Weckbach

TL;DR
This study found that midkine levels are elevated in patients with dilated cardiomyopathy but cannot distinguish between inflammatory and non-inflammatory types.
Contribution
The study evaluates midkine as a potential biomarker for differentiating inflammatory from non-inflammatory dilated cardiomyopathy.
Findings
Midkine levels were higher in DCM/DCMi patients compared to healthy individuals.
Midkine levels did not differ significantly between DCM and DCMi patients.
Midkine showed no strong correlation with clinical parameters like NYHA class or LVEF.
Abstract
Objectives: This retrospective study examines midkine, an inflammatory cytokine, as a potential serological biomarker to distinguish dilated cardiomyopathy (DCM) and inflammatory dilated cardiomyopathy (DCMi). Identifying such a biomarker is crucial for effective treatment of these two entities. Methods: The study included 54 patients with heart failure, reduced left ventricular systolic function, and suspected cardiac inflammation. Endomyocardial biopsies were obtained from all 54 patients to differentiate between DCM and DCMi. Blood sera were collected from these patients the same day the endomyocardial biopsy was performed and compared with those of 13 age-matched healthy individuals for different measurements such as midkine and NT-proBNP. Patients were followed up to a median of 194 days after the baseline visit. Results: Endomyocardial biopsies from patients with DCMi were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
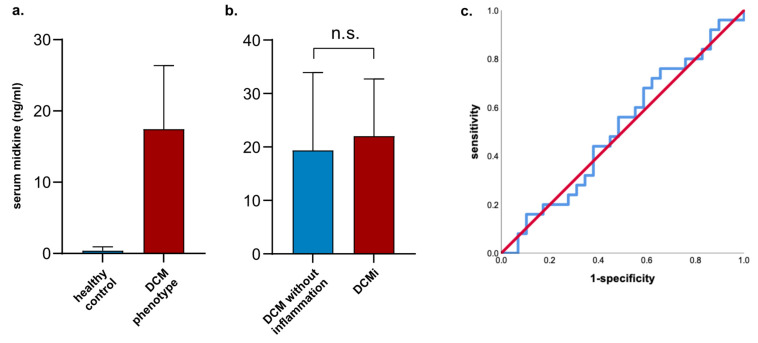 Figure 1
Figure 1- —Deutsche Forschungsgemeinschaft
- —Transregional Collaborative Research Centre ‘Inflammatory Cardiomyopathy—Molecular Pathogenesis and Therapy Berlin’
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Cardiac Fibrosis and Remodeling · Eosinophilic Disorders and Syndromes
1. Introduction
Heart failure represents a major clinical and epidemiological syndrome with increasing prevalence and high morbidity and mortality. Brain natriuretic peptide (BNP) or the N-terminal BNP (NT-proBNP) are routinely used as biomarkers in clinical practice [1]. As inflammation is a critical feature of heart failure, different inflammatory markers including C-reactive protein (CRP) or the interleukins (IL) 1, 6, and 18 represent interesting candidates as additional biomarkers. Furthermore, the pro-inflammatory cytokine midkine (MK) has been investigated as a biomarker in heart failure [2]. Midkine is a 13-kDa heparin-binding cytokine and growth factor with a relevant role in various physiological and pathophysiological processes due to its pro-inflammatory, pro-angiogenic, anti-apoptotic, and anti-infective functions [3]. Early studies by Kadomatsu et al. [4] showed that MK is up-regulated during mid-gestation in mice embryos, but its expression in adult mice is confined to the kidney. Numerous cell types such as monocytes, macrophages, monocyte-derived dendritic cells (mDCs), and endothelial cells have been identified to produce MDK under basal and pathological conditions [5]. It has been shown that MK plays a role in vascular remodeling, angiogenesis, and inflammation, in conditions such as atherosclerosis, myocardial infarction, and hypertension [3]. Moreover, MK levels were found to be elevated in the serum of patients with sepsis and septic shock when compared to control subjects [6]. In the context of dilated cardiomyopathy (DCM), a study by Danielle Jeffrey indicated that midkine is up-regulated in both the plasma and cardiac tissue of pediatric patients with DCM. Additionally, the presence of circulating midkine contributes to pathological changes in gene expression by increasing the expression of the atrial natriuretic factor (ANF) and b-type natriuretic peptide (BNP) [7]. Overall, midkine shows potential as a biomarker in various pathological conditions, including applications for early detection, disease progression monitoring, and treatment response assessment. Our research group has shown that MK was critically involved in cardiac inflammation in a mouse model of experimental autoimmune myocarditis. Blocking MK reduced leukocyte infiltration and ameliorated subsequent fibrosis and heart failure [8]. Although myocarditis is commonly self-limiting, some patients will develop progressive heart failure due to ongoing cardiac inflammation, which is referred to as inflammatory dilated cardiomyopathy (DCMi) [9,10]. As the diagnosis of DCMi may influence therapy (e.g., immunomodulation), we examined whether MK serum levels may differentiate DCMi from non-inflammatory DCM.
2. Material and Methods
2.1. Patient Study Design
Fifty-four patients (52 male, 2 female) with heart failure with reduced left ventricular systolic function and suspected cardiac inflammation gave written informed consent to be prospectively enrolled into a cardiomyopathy registry (2004–2013, University Hospital of Greifswald). Blood sera were collected and compared with those of 13 male, age-matched, healthy individuals (mean age 53.8 ± 2.8) that were used as the control. Relevant coronary artery disease as a pathophysiological cause for heart failure was excluded in all patients using coronary angiography. Endomyocardial biopsies were obtained from all 54 patients to differentiate between DCM and DCMi. DCMi was defined by the presence of >14 inflammatory cells/mm^2^, in addition to the enhanced expression of human leukocyte antigen (HLA) class II molecules as previously described [9]. Pregnant patients, patients with known autoimmune disease or treated with anti-inflammatory medication, and patients <18 years of age were excluded, as well as patients who received therapeutic dosages of heparin, as administration of such dosages can dramatically increase MK serum levels [11]. As MK levels are also influenced by renal failure, only patients with a glomerular filtration rate (eGFR) above 60 mL/min were included in the study. Blood samples were collected on the same day the endomyocardial biopsy was performed. Patients were followed up to a median of 194 [IQR 156–265] days after the baseline visit. The investigation conforms with the principles outlined in the Declaration of Helsinki.
2.2. ELISA
Midkine serum levels were measured using a colorimetric enzyme-linked immunosorbent assay (Midkine ELISA, CELLMID, Sydney, Australia). To assess the levels of circulating N-terminal pro-B-type natriuretic peptide (NT-proBNP), we used the enzyme-linked immunosorbent assay (ELISA; Biomedica, Vienna, Austria).
2.3. Glomerular Filtration Rate (GFR)
Creatinine was measured in plasma according to routine diagnostic methods and GFR was calculated with the MDRD formula.
2.4. Immunohistochemical Analysis
The data collected from the endomyocardial biopsies were obtained from hospital records. For this analysis, we relied on the expertise of the individuals conducting the work. The pathologists from the University Hospital Tübingen were part of the German Research Foundation (DFG), Transregional Collaborative Research Centre “Inflammatory Cardiomyopathy—Molecular Pathogenesis and Therapy” project that enabled the cardiomyopathy registry that is the source of samples and data for this project. The immunohistochemistry protocol used has been published in other analyses from the registry [9,12]. For the immunohistochemical analyses, we examined cardiac inflammation in paraffin-embedded tissue sections using the avidin-biotin-immunoperoxidase method, adhering to the manufacturer’s protocol (Vectastatin Elite ABC kit, Vectastatin^®^, Vector Laboratories, Newark, CA, USA) [9,12]. We employed monoclonal antibodies to assess cardiac cell infiltration, specifically evaluating CD3^+^ T-lymphocytes (Novocastra Laboratories, Newcastle upon Tyne, UK) and CD68^+^ macrophages (DAKO, Hamburg, Germany), in accordance with the guidelines for the Definition and Classification of Cardiomyopathies that were in place at the time of data collection [13]. To evaluate HLA class II expression, we utilized an anti-HLA-DR-α antibody (DAKO, Hamburg, Germany) [9].
2.5. Cardiac Parameter
Echocardiographic evaluations were conducted on all patients using 2-dimensional echocardiography during their initial hospital admission, following the American College of Cardiology/American Heart Association guidelines applicable at the time of data collection [14]. The left ventricular ejection fraction was measured using the biplane Simpson method, while left ventricular dilation was assessed by measuring the left ventricular end-diastolic diameter (LVEDD).
2.6. Viral Load EMB
For the detection of viral genomes in myocardial biopsies, a nested PCR/RT-PCR was performed as described previously [15].
2.7. Statistical Analysis
All data are presented as the median with 95% confidence interval (CI). Comparisons of dichotomous variables were analyzed by the Chi-Square-test (χ^2^). The Kolmogorov–Smirnov test was performed to analyze the normal distribution of continuous variables. Not normally distributed data were evaluated using a two-tailed Mann–Whitney U-test. Normally distributed variables were evaluated by a two-sided t-test. Correlation was tested using Pearson’s R. A p-value of <0.05 was considered statistically significant. For the statistical analysis, SPSS statistics (version 26, IBM, Armonk, NY, USA) was used.
3. Results
The clinical characteristics of patients with DCM and DCMi are depicted in Table 1. Twenty-nine patients had DCM, of whom three had a presumed alcohol toxic etiology, one had a possible familial/genetic DCM, and one had a presumed decompensated hypertensive heart disease. Twenty-five patients showed immunohistochemical evidence of inflammatory DCM. To adjust for possible confounders, groups were matched for NYHA functional class, NT-proBNP levels, renal function, and left ventricular ejection fraction (LVEF), as well as the left ventricular end-diastolic diameter (LVEDD). Therefore, these parameters were similar in both groups. Major histocompatibility complex-II (MHC-II) upregulation, the number of infiltrated CD68^+^ macrophages, as well as CD3^+^ T cells in the endomyocardial biopsy were significantly higher in the DCMi compared to the DCM group, as these parameters were used to differentiate between both entities. Further, detection of a viral genome was more frequent in DCMi patients. Follow-up characteristics are shown in Table 2.
In total, nine patients died during follow-up: four patients in the DCM group and five patients in the DCMi group, respectively (13.8% vs. 20% in the DCMi group; p = 0.542, Table 2). Both groups showed comparable improvement of LV function and diameters at follow-up 1 (at a median of 95 (IQR 69–108) days after baseline visit, Table 2), and further at follow-up 2 (at a median of 194 (IQR 156–265) after baseline visit, Table 2). In comparison to healthy individuals, MK serum levels were significantly increased in patients with a DCM phenotype (median 0.4 (IQR 0.3–0.7) ng/mL in healthy individuals vs. 21.4 (IQR 5.3–35.0) ng/mL in patients with a DCM phenotype, p < 0.001, Figure 1a).
Further, we could not detect any differences in MK serum levels between patients who initially presented with dilated cardiomyopathy in echocardiography and underwent endomyocardial biopsy for further immunohistological differentiation into both entities (median 19.4 (IQR 4.9–38.8) ng/mL in DCM vs. 22.0 (IQR 7.1–34.2) ng/mL in patients with DCMi, p = 0.883, Figure 1b). Figure 1c shows the receiver operating characteristic (ROC) curve for MK serum levels, reflecting no separation between DCM and DCMi (area under curve (AUC) of 0.512, 95% CI 0.356–0.668).
To gain further insights into the prognostic value of MK as a biomarker in heart failure, we investigated whether MK serum levels would correlate with functional parameters in heart failure including NYHA functional class, NT-proBNP levels, LVEF, and LVEDD at baseline and follow-up. However, none of these parameters correlated significantly with MK serum levels, except LVEF at follow-up 2 (Pearson’s R 0.348, p = 0.047, Table 3).
4. Discussion
DCMi reflects a relevant sub-entity of the phenotype DCM. To date, the diagnosis of DCMi relies on the immunohistochemical evaluation of endomyocardial biopsies. A definitive diagnosis is often not established in clinical practice due to safety concerns. Since evidence suggests that cardiac function cannot be improved in patients with DCMi despite receiving optimal drug therapy, left ventricular ejection fraction (LVEF) does improve with immunosuppressive therapy in patients with biopsy-proven virus-negative inflammatory cardiomyopathy [9,16,17]. Therefore, identifying a biomarker to differentiate between the two entities is of critical therapeutic importance. We have recently shown that MK mRNA expression was substantially elevated in the inflamed cardiac tissue in a myocarditis mouse model compared to the control mice [8]. Therefore, we have attempted to identify the inflammatory cytokine MK as a possible serological biomarker to distinguish the DCM entities within the present retrospective study.
MK serum levels were markedly elevated in patients with DCM or DCMi compared to healthy individuals, but did not differ between the two biopsy-distinguished groups. Further, they did not show a correlation with heart failure-classifying parameters.
As we showed in the present study, MK was not differentially concentrated between both groups. This may be explained by the fact that heart failure per se is a highly inflammatory condition, which is accompanied by a significant up-regulation and subsequent release of MK into the circulation. The up-regulation of MK in heart failure has been demonstrated in the failing hearts of pediatric patients with DCM compared to the non-failing control hearts at the RNA level [18]. These findings suggest that up-regulation of MK may be a typical mechanism for failing hearts. However, the source of MK in failing hearts and in the serum of heart failure patients is still undetermined.
Our finding of elevated MK serum levels in DCM patients is in accordance with a study conducted by Kitahara and colleagues [2]. In contrast to our study, Kitahara et al. only observed modestly increased MK serum levels (2–4-fold) in heart failure patients compared to healthy controls. In our study, MK serum levels were approximately 50-fold elevated in patients with a DCM phenotype compared to healthy individuals. This may be due to the fact that the systolic function in our study was substantially reduced (mean 29.5%) and left ventricles were markedly dilated (mean 67.8 mm), whereas systolic function and LVEDD were only mildly abnormal in the study conducted by Kitahara et al. indicating that in our study, heart failure was more progressed [2]. Nevertheless, the serum levels of healthy individuals were comparable to values measured by different working groups, underlying the validity of our data [19,20,21,22,23].
We set out to investigate whether MK serum levels would correlate with baseline and follow-up parameters classifying heart failure in patients. However, we did not observe any correlation between MK serum levels and NYHA functional class, natriuretic peptides, LVEF, or LVEDD at baseline. Only LVEF at follow-up 2 showed a weak correlation, which—in synopsis with the missing correlation with baseline and other follow-up parameters—can be regarded as an outlier. In contrast to our study, Kitahara et al. found a correlation between NYHA functional class and MK serum levels despite only moderately elevated MK serum levels in heart failure patients in that study, which may be due to the larger sample size and a more heterogeneous patient population [2]. In this regard, we would like to emphasize that our study has limitations related to the number of patients and to the gender disproportion, which is predominantly due to the higher incidence and severity of most cardiovascular diseases in males [24].
5. Conclusions
In summary, we observed markedly elevated MK serum levels in patients with a DCM phenotype with severely reduced systolic function. However, MK serum levels could not discriminate between DCM and DCMi and showed no correlation with baseline or follow-up parameters. We conclude that midkine cannot be used as a biomarker to distinguish between DCM and DCMi.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Braunwald E. Biomarkers in heart failure N. Engl. J. Med.20083582148215910.1056/NEJ Mra 080023918480207 · doi ↗ · pubmed ↗
- 2Kitahara T. Shishido T. Suzuki S. Katoh S. Sasaki T. Ishino M. Nitobe J. Miyamoto T. Miyashita T. Watanabe T. Serum midkine as a predictor of cardiac events in patients with chronic heart failure J. Card. Fail.20101630831310.1016/j.cardfail.2009.12.01420350697 · doi ↗ · pubmed ↗
- 3Majaj M. Weckbach L.T. Midkine-A novel player in cardiovascular diseases Front. Cardiovasc. Med.20229100310410.3389/fcvm.2022.100310436204583 PMC 9530663 · doi ↗ · pubmed ↗
- 4Kadomatsu K. Huang R.P. Suganuma T. Murata F. Muramatsu T. A retinoic acid responsive gene MK found in the teratocarcinoma system is expressed in spatially and temporally controlled manner during mouse embryogenesis J. Cell Biol.199011060761610.1083/jcb.110.3.6071689730 PMC 2116029 · doi ↗ · pubmed ↗
- 5Muramatsu T. Midkine, a heparin-binding cytokine with multiple roles in development, repair and diseases Proc. Jpn. Acad. Ser. B Phys. Biol. Sci.20108641042510.2183/pjab.86.41020431264 PMC 3417803 · doi ↗ · pubmed ↗
- 6Krzystek-Korpacka M. Mierzchala M. Neubauer K. Durek G. Gamian A. Midkine, a multifunctional cytokine, in patients with severe sepsis and septic shock: A pilot study Shock 20113547147710.1097/SHK.0b 013e 318208600121192283 · doi ↗ · pubmed ↗
- 7Jeffrey D.A. Pires Da Silva J. Garcia A.M. Jiang X. Karimpour-Fard A. Toni L.S. Lanzicher T. Peña B. Miyano C.A. Nunley K. Serum circulating proteins from pediatric patients with dilated cardiomyopathy cause pathologic remodeling and cardiomyocyte stiffness JCI Insight 20216 e 14863710.1172/jci.insight.14863734383712 PMC 8525651 · doi ↗ · pubmed ↗
- 8Weckbach L.T. Grabmaier U. Uhl A. Gess S. Boehm F. Zehrer A. Pick R. Salvermoser M. Czermak T. Pircher J. Midkine drives cardiac inflammation by promoting neutrophil trafficking and NE Tosis in myocarditis J. Exp. Med.201921635036810.1084/jem.2018110230647120 PMC 6363424 · doi ↗ · pubmed ↗