Man With an Itchy Back
Katherine Schaffer, Nevin Adamski, Brittany Ambrose, Kathleen Anderson

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1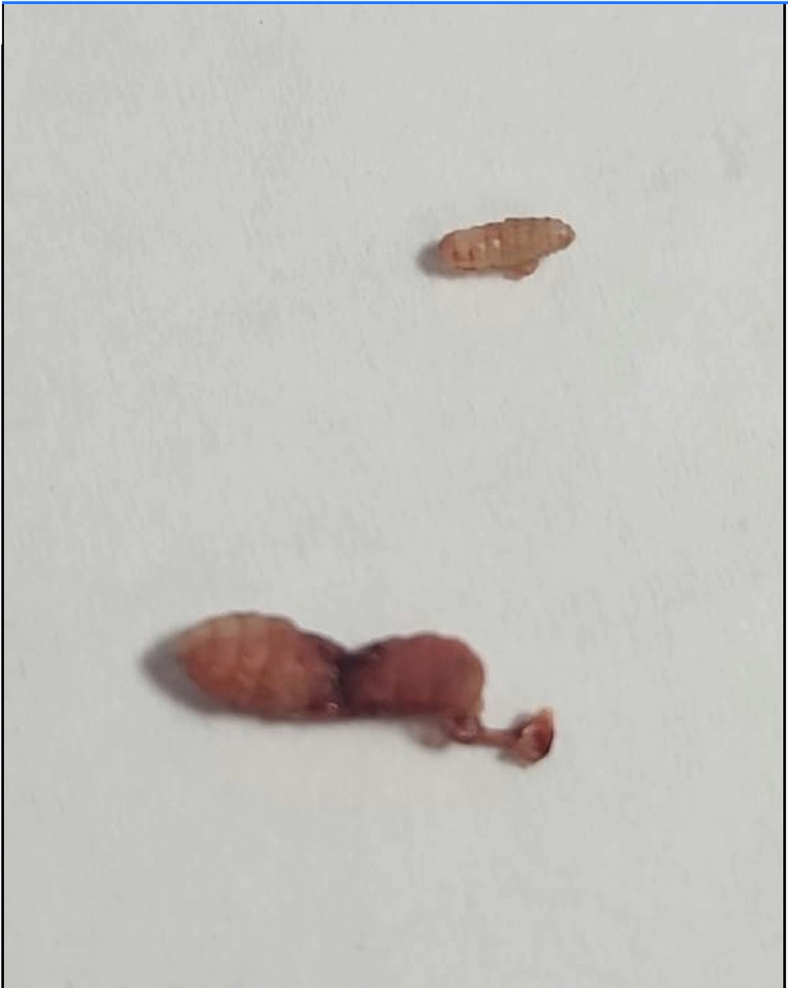 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Entomology and Diptera Studies · Rabies epidemiology and control · Human-Animal Interaction Studies
Case
1
A 61-year-old man with no significant past medical history presented with painful bug bites on his lower back 1 day after a 1.5-week-long visit to Africa. He noticed bug bites on his lower back 3 days ago; since then, they have increased in size and become more painful. He was prescribed doxycycline at urgent care earlier that morning and had taken 1 dose. He is taking prophylactic medications for malaria and has had no fever at home. Vital signs, including temperature, are within normal limits. A physical examination shows 2 exquisitely tender papular lesions with a central punctum and surrounding erythema in the bilateral paralumbar regions (Fig 1).Figure 1. Image of the patient's back with 2 furuncular myiasis.
Incision and drainage of the skin lesions were performed using local anesthesia. A foreign body was noted to be protruding through the skin opening during anesthetic injection on both sides. The skin openings were extended, and hemostats were used to extract the foreign bodies, which were identified as maggots (Fig 2).Figure 2. Image of larvae of Cordylobia anthropophaga.
Diagnosis
2
Cordylobia anthropophaga. Tumbu fly, or mango fly, is endemic in tropical Africa and causes furuncular myiasis.1 The female fly lays its eggs in soil or on wet clothes, and the primary larvae emerge approximately 2 days later. These larvae can then penetrate unbroken human skin and develop into tertiary larvae within the dermis.2 They will maintain a breathing pore in the skin from which they emerge when fully mature.
Diagnosis is based on the presence of the lesion, subjective sensation of movement, and recent travel history. Covering the punctum with gel can asphyxiate the larvae and force them to the surface. Surgical extraction may also be necessary, as in this case. Bedside ultrasonography may aid in diagnosis.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yasukawa K.Dass K.Myiasis due to Cordylobia anthropophaga Am J Trop Med Hyg 1022202025110.4269/ajtmh.19-057932519647 PMC 7008319 · doi ↗ · pubmed ↗
- 2Suárez J.A.Ying A.Orillac L.A.Cedeño I.Sosa N.First case of furuncular myiasis due to Cordylobia anthropophaga in a Latin American resident returning from Central African Republic Braz J Infect Dis 2212018707310.1016/j.bjid.2017.12.00329362134 PMC 9425688 · doi ↗ · pubmed ↗