Shortness of Breath After Heart Surgery
Savannah Pocquette, Katelyn Levy, Jeffrey Gardecki

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
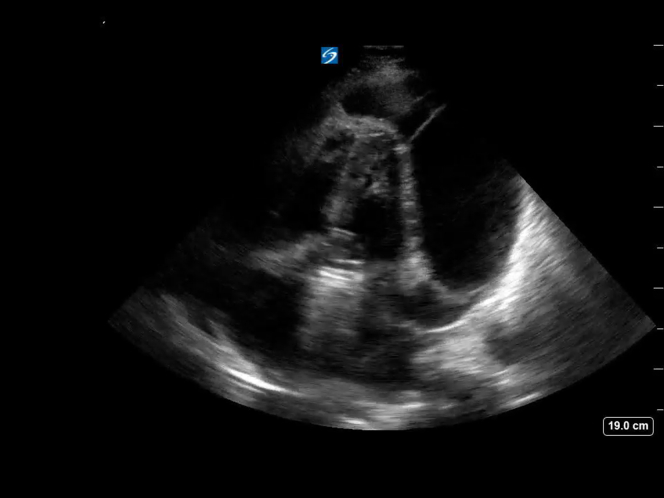 Figure 1
Figure 1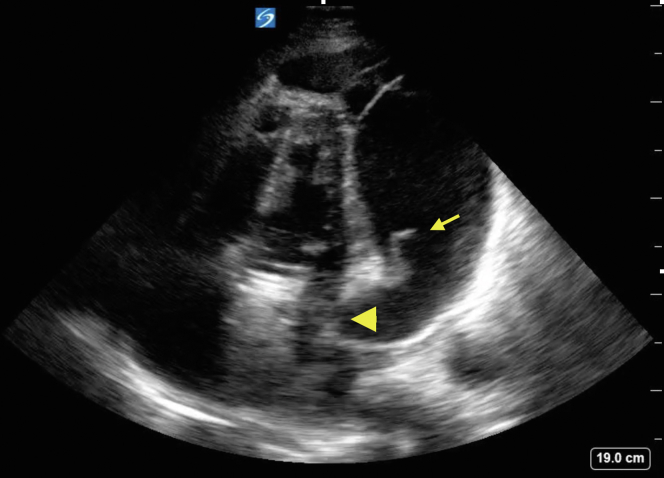 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Ultrasound in Clinical Applications · Cardiac, Anesthesia and Surgical Outcomes
Patient Presentation
1
A 56-year-old man with a history of aortic root aneurysm 3 weeks after surgery from an aortic root replacement with a mechanical valve-conduit presented to the emergency department with exertional dyspnea. He reported a week of progressive worsening of symptoms. He was afebrile with a heart rate of 112 cpm and blood pressure of 110/77 mm Hg. He had clear lungs and a faint systolic murmur without signs of volume overload. A point-of-care cardiac ultrasound was performed (Video 1). The ultrasound findings prompted consultation with cardiothoracic surgery.Video 1Apical 4 chamber view of the heart demonstrating a large circumferential complex pericardial effusion. Fibrin stranding is demonstrated beating with the atrioventricular valves. Signs of tamponade physiology are seen with both right ventricular and left ventricular collapse in diastole.
Diagnosis: Complex Pericardial Effusion Causing Tamponade
2
The patient was immediately taken to the operating room for a subxiphoid pericardial window for cardiac tamponade. Emergency physicians can use point-of-care ultrasound for the identification of pericardial effusions, which include states of profound shock and cardiac arrrest.1 The findings on point-of-care ultrasound that were suggestive of cardiac tamponade include the presence of a pericardial effusion with identification of cardiac chamber collapse (Fig).2^,^3 The specificity for tamponade goes up with progression of the chamber involved from the right atria and ventricle to eventually the left sided cardiac chambers.3 Collapse of the left atrium and ventricle can be seen in the apical 4 chamber clip. Postoperative tamponade can involve the left ventricle and is seen most frequently after valve surgery and in patients on anticoagulation.3^,^4FigureFibrin strands (arrow) can be seen moving through the cardiac cycle mimicking the appearance of the atrioventricular valves. The right ventricle and atria are not well visualized on this image; however, diastolic collapse of the left atria (arrowhead) is evident.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tayal V.S.Kline J.A.Emergency echocardiography to detect pericardial effusion in patients in PEA and near-PEA states Resuscitation 593200331531810.1016/s 0300-9572(03)00245-414659600 · doi ↗ · pubmed ↗
- 2Alerhand S.Carter J.M.What echocardiographic findings suggest a pericardial effusion is causing tamponade?Am J Emerg Med 372201932132610.1016/j.ajem.2018.11.00430471929 · doi ↗ · pubmed ↗
- 3Spodick D.H.Acute cardiac tamponade N Engl J Med 3497200368469010.1056/NEJ Mra 02264312917306 · doi ↗ · pubmed ↗
- 4Pepi M.Muratori M.Barbier P.Pericardial effusion after cardiac surgery: incidence, site, size, and haemodynamic consequences Br Heart J 724199432733110.1136/hrt.72.4.3277833189 PMC 1025541 · doi ↗ · pubmed ↗