Complex endocarditis in a young patient
Marie-Luise Dikou, Abigail Gowland, Sara Volpi, Julia Grapsa, Gianluca Lucchese

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
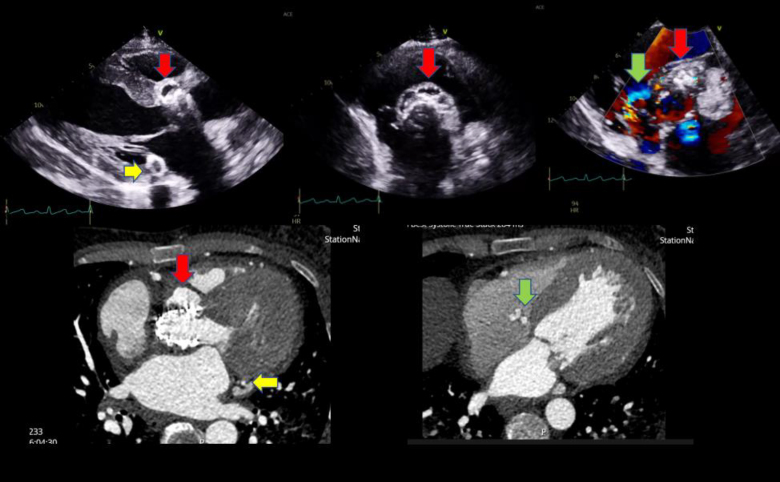 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Actinomycetales infections and treatment · Infectious Aortic and Vascular Conditions
A 36-year-old female patient presented to her local district general hospital feeling breathless, generally unwell, and lethargic on a background of a complex past medical history including an episode of Libman–Sacks endocarditis a year previously. She also had systemic lupus erythematosus with lupus nephritis and end-stage renal disease on haemodialysis, antiphospholipid syndrome, thrombocytopaenia, and recurrent pulmonary haemorrhages. She had previously undergone plasma exchange and rituximab treatment and was now on cyclophosphamide.
During her previous endocarditis episode and following a multidisciplinary meeting, with the main concern the previous alveolar haemorrhages, she was judged high risk for open-heart surgery and underwent a transcatheter aortic valve replacement (26 mm S3) locally.
The patient was transferred to our tertiary centre on this presentation with signs of heart failure, multiple positive blood cultures for Staphylococcus epidermidis, septic pulmonary emboli, and suspicion of aortic root abscess on transthoracic echocardiogram (Videos 1 and 2).
On presentation, she was clinically septic, had an infected indwelling permanent line, and grew S. epidermidis on repeat blood cultures, which was discussed with microbiology and treated with a course of vancomycin and rifampicin.
She was investigated with multiple imaging modalities including transthoracic and transoesophageal echocardiogram. She was discovered to have a large aortic root abscess (Figure 1, red arrow) with associated vegetation and fistulation into the right atrium (green arrow), as well as posterior mitral annular abscess (yellow arrow).
Despite the high surgical risk and after extensive discussion with the heart multidisciplinary care team, the patient underwent open-heart surgery without the need of extracorporeal support, with a good recovery.