Left atrial myxoma associated with multivessel coronary embolism confirmed by cardiac magnetic resonance imaging: a case of myocardial infarction with non-obstructive coronary arteries
Annalisa Pasquini, Andrea Caffè, Monica Filice, Rosa Lillo, Rocco Antonio Montone, Giovanni Alfonso Chiariello, Natalia Pavone, Marialisa Nesta, Maria Grandinetti, Piergiorgio Bruno, Francesco Burzotta, Massimo Massetti

TL;DR
A rare case of heart attack caused by a left atrial myxoma was diagnosed using advanced imaging techniques.
Contribution
Demonstrates the diagnostic utility of cardiac MRI in identifying rare causes of myocardial infarction.
Findings
Cardiac MRI detected a left atrial mass and ischaemic patterns consistent with coronary embolism.
Surgical excision confirmed the mass was a cardiac myxoma.
Multimodal imaging helped identify a rare cause of MINOCA.
Abstract
Explore the diagnostic value of multimodal imaging in identifying considerably rare causes of myocardial infarction. We report a case of myocardial infarction with non-obstructive coronary arteries (MINOCA) probably due to coronary embolism associated with a left atrial myxoma. A 56-year-old male presented with non-ST-elevation myocardial infarction, with coronary angiography showing mild coronary atherosclerosis without significant epicardial stenosis. Transthoracic echocardiography and cardiac magnetic resonance imaging (CMR) revealed a large left atrial mass, suspected to be an atrial myxoma. CMR also showed an ischaemic pattern involving multiple coronary territories, suggesting coronary embolism as the cause of the MINOCA. The patient underwent successful surgical excision of the left atrial mass, and histopathology confirmed the diagnosis of cardiac myxoma. This case highlights…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
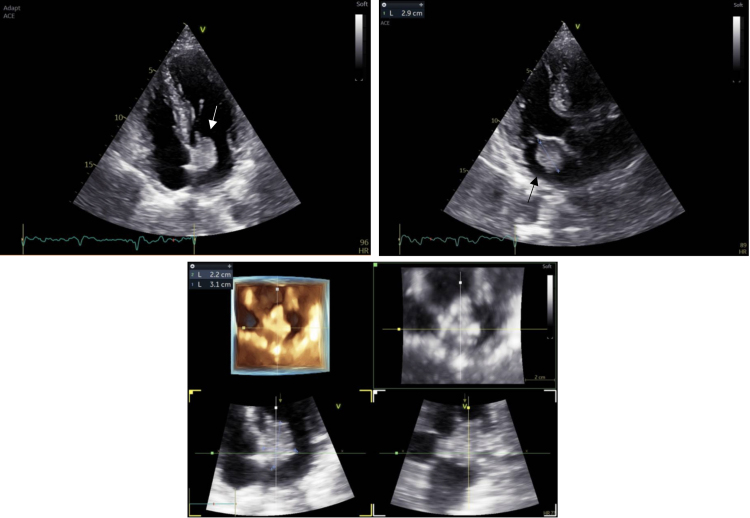 Figure 1
Figure 1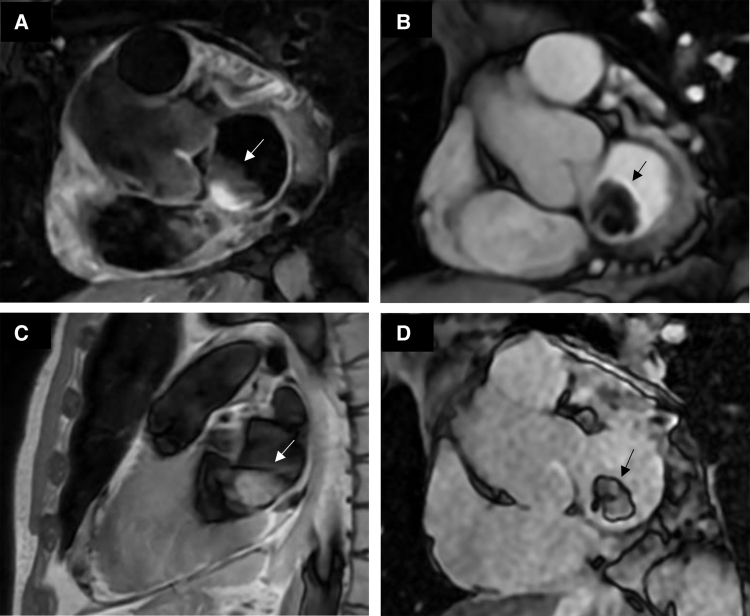 Figure 2
Figure 2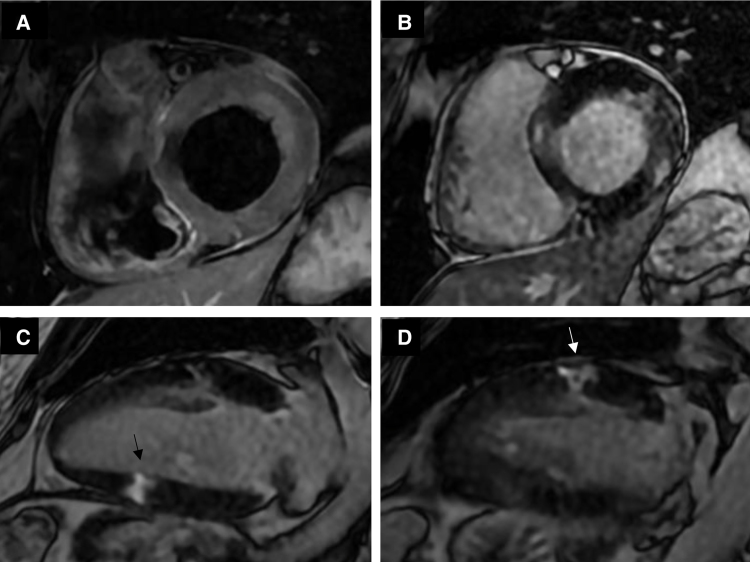 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
Case presentation
We present a case of myocardial infarction with non-obstructive coronary arteries (MINOCA) due to a left atrial myxoma-associated coronary embolism, where an embolic ischaemic pattern was confirmed by cardiac magnetic resonance imaging (CMR). This case is notably rare because a suspected coronary embolism from a cardiac myxoma was confirmed by the ischaemic pattern involving multiple coronary territories on CMR.
A 56-year-old male patient was admitted to the emergency department with left-sided stabbing chest pain that was neither aggravated by finger pressure nor relieved by position. He denied recent fever and flu-like symptoms. Blood pressure was 130/80 mmHg, heart rate was 66 bpm, peripheral oxygen saturation was 98% on room air, and body temperature was normal.
The patient had a history of type II diabetes mellitus and systemic arterial hypertension, without any previous cardiovascular events.
The electrocardiogram performed in the emergency department showed sinus rhythm, possible previous lateral necrosis, and non-specific ventricular repolarization abnormalities, while the chest X-ray was within normal limits. High-sensitivity troponin I was 422 and 3415 ng/L (upper limit of normal 57 ng/L) in two consecutive determinations within 1 h. Other routine laboratory tests were within normal limits, except for a mild neutrophilic leukocytosis (white blood cell count 10.8 × 109/L).
Transthoracic echocardiography (Figure 1 and Videos 1 and 2) showed a voluminous left atrial echogenic mass with a large implantation site on the inferior interatrial septum and a floating and irregular border, in the absence of mitral valve plane involvement or haemodynamic compromise. Left ventricular ejection fraction was preserved without regional wall motion abnormalities. All other findings were within normal limits.
Transthoracic echocardiography. Presence of a left atrial oval formation.
The patient was therefore admitted to the cardiac intensive care unit and underwent coronary angiography the following day, which revealed a left-dominant circulation with mild coronary atherosclerosis in the absence of significant epicardial lesions (Videos 3 and 4). High-sensitivity troponin I peaked on Day 1 (18 248 ng/L).
Coronary computed tomography angiography confirmed the absence of significant epicardial atherosclerosis and the presence of a left atrial oval formation (29 × 22 mm) involving the atrioventricular plane, in contact with the posteromedial commissure and the A3 and P3 mitral leaflets.
CMR imaging showed a highly mobile floating solid mass (28 × 20 mm in four-chamber view) with lobulated margins, broadly in contact with the interatrial septum, caudal to the oval fossa and extending to the junction between the anterior mitral leaflet and the valvular annulus, partially exceeding the latter during diastole. The mass was isointense on T1-weighted images and hyperintense on T2-black blood, with mild eccentric enhancement (Figure 2). This mass was suspected to be an atrial myxoma.
CMR, left atrial mass. CMR T2-weighted black-blood image (A), cine SSFP image (B), T1-weighted image (C), and myocardial delayed enhancement image (D) showing the left atrial mass suspected to be a left atrial myxoma.
Furthermore, on T2-weighted images, oedema was documented in the lateral basal and mid-ventricular wall and focal oedema in the inferior mid-ventricular wall. On delayed enhancement images, abnormal transmural enhancement was demonstrated in parts of the lateral mid-ventricular wall and focal enhancement in the inferior mid-ventricular wall. This was associated with mild diffuse subendocardial hyperintensity in the anterior mid-ventricular wall and transmural hyperintensity in the remaining anterolateral and inferior mid-ventricular walls. Cine-CMR images showed regional wall motion abnormalities in the left anterior descending and circumflex artery territories (Figure 3 and Video 5). This multivessel ischaemic pattern was consistent with embolic myocardial infarction, so the diagnosis of embolic MINOCA was established.
CMR, multifocal ischaemic changes. CMR T2-weighted image (A) and myocardial delayed enhancement images (B–D) showing ischaemic changes in the left anterior descending and circumflex artery territories.
Outcome and follow-up
On Day 5, the patient underwent surgical removal of a gelatinous left atrial mass through a biatrial transseptal approach. The postoperative course in the cardiac surgical intensive care unit was uneventful. On postoperative Day 2, the patient was transferred to the cardiac surgery unit and then to a cardiac rehabilitation unit.
The diagnosis of cardiac myxoma was then confirmed by histopathological examination, which shows cellular elements with oval nuclei and finely dispersed chromatin, interspersed in a myxoid matrix.
On 6-month follow-up, the patient did not experience any cardiovascular adverse event or tumour recurrence at transthoracic echocardiographic evaluation.
Discussion
MINOCA is a working diagnosis that applies in the presence of criteria for acute myocardial infarction (MI) and no coronary artery stenosis ≥50% on coronary angiography in the absence of alternative non-ischaemic causes for the acute presentation.^1^ MINOCA accounts for about 5–6% of all patients undergoing coronary angiography for MI, and a multimodal diagnostic approach is needed to tailor treatment based on pathophysiologic mechanisms, based on coronary functional assessment through acetylcholine (ACh) provocative testing,^2^ optical coherence tomography (OCT), and CMR.^3^ Causes of MINOCA include epicardial or microvascular coronary artery spasm, non-significant atherosclerotic plaque disruption rupture/erosion, non-obstructive coronary artery dissection, and coronary embolism.^1^
Cardiac myxomas are the most common primary cardiac tumours, accounting for 50–85% of benign cardiac neoplasms. They arise from mesenchymal cell precursors and form intracavitary masses, mainly in the left atrium (75% of cases), where they are often attached to the fossa ovalis by a stalk/peduncle. However, myxomas may also arise in the right atrium, left atrial free wall or appendage, and rarely in the ventricles or valve leaflets.^4,5^
The estimated prevalence of cardiac myxomas is 0.03%, with an annual incidence of 0.5–1 case per million. Myxomas can affect any age but are most commonly diagnosed in middle age and have a female preponderance (female-to-male ratio of approximately 3:1).^7^ About 7% of patients diagnosed with cardiac myxoma are affected by Carney complex, an autosomal dominant syndrome associated with endocrine hyperactivity and lentiginosis.^4^
Intracardiac obstruction may be the initial manifestation (mainly associated with polypoid tumours), with valvular obstruction often involving the mitral valve during diastole, which may lead to syncopal episodes, heart failure symptoms, and the development of progressive pulmonary hypertension.^4,5^
Myxomas may present as polypoid or papillary (or villous), the latter being particularly prone to give rise to embolic events due to their friable texture and tendency to fragment.^4,5^ Embolic events occur in 30–40% of myxoma patients and represent the ‘functional malignancy’ of myxoma.^4,5^ Myxoma-related coronary embolism is a rare phenomenon: in a cohort of 162 patients with cardiac myxoma, only one presented with coronary embolism (0.62%).^6^ This rarity is attributed to the small diameter of the coronary ostia, their right-angled junction within the aortic bulb, and the protection provided by the aortic valve cusps.^7^
Other reports of myocardial infarction likely due to embolism arising from cardiac myxomas have been previously described in the literature.^7^ Typically, CMR, when applied, has been used in such instances primarily to characterize the cardiac mass rather than to confirm an embolic ischaemic pattern in MINOCA.^8^ In our case, however, CMR also played a key role in supporting the diagnosis of coronary embolism as the underlying mechanism of MINOCA, revealing ischaemic involvement of multiple coronary territories.
On the other hand, ACh intracoronary testing and OCT were not performed in our case, as a vasomotor abnormality was not suspected based on the clinical presentation, nor was plaque instability indicated by the angiographic findings.
In conclusion, in this case report, we have documented a rare occurrence of MINOCA due to coronary embolism from a left atrial myxoma. The identification of an embolic pattern through CMR is considerably rare in such clinical scenarios, making its application in this case particularly valuable and underscoring its crucial role in the diagnostic process for MINOCA.^9^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM et al Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation 2019;139:e 891–e 908.30913893 10.1161/CIR.0000000000000670 · doi ↗ · pubmed ↗
- 2Montone RA, Rinaldi R, Del Buono MG, Gurgoglione F, La Vecchia G, Russo M et al Safety and prognostic relevance of acetylcholine testing in patients with stable myocardial ischaemia or myocardial infarction and non-obstructive coronary arteries. Euro Intervention 2022;18:e 666–76.35377315 10.4244/EIJ-D-21-00971 PMC 10241282 · doi ↗ · pubmed ↗
- 3Tayal B, Freeman P, Ericsson F, Kragholm KH, Andersen NH, Hagendorff A et al Characterisation of patients with and without cardiac magnetic resonance imaging abnormalities presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA). Acta Cardiol 2021;76:760–8.32594904 10.1080/00015385.2020.1785134 · doi ↗ · pubmed ↗
- 4Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, Manisty C et al Cardiac tumors: JACC Cardio Oncology state-of-the-art review. JACC Cardio Oncol 2020;2:293–311.34396236 10.1016/j.jaccao.2020.05.009PMC 8352246 · doi ↗ · pubmed ↗
- 5Islam AKMM. Cardiac myxomas: a narrative review. World J Cardiol 2022;14:206–19.35582466 10.4330/wjc.v 14.i 4.206PMC 9048271 · doi ↗ · pubmed ↗
- 6He DK, Zhang YF, Liang Y, Ye SX, Wang C, Kang B et al Risk factors for embolism in cardiac myxoma: a retrospective analysis. Med Sci Monit 2015;21:1146–54.25900256 10.12659/MSM.893855 PMC 4418206 · doi ↗ · pubmed ↗
- 7Braun S, Schrötter H, Reynen K, Schwencke C, Strasser RH. Myocardial infarction as complication of left atrial myxoma. Int J Cardiol 2005;101:115–21.15860393 10.1016/j.ijcard.2004.08.047 · doi ↗ · pubmed ↗
- 8Rofe A, Fazio TN, Jones N, Al-Kaisey AM. An unusual presentation of atrial myxoma: thromboembolic phenomenon with a recent normal echocardiogram. BMJ Case Rep 2019;12:e 230266.10.1136/bcr-2019-230266 PMC 676837431570351 · doi ↗ · pubmed ↗