Technological Advances for Gait and Balance in Normal Pressure Hydrocephalus: A Systematic Review
Alessandro Zampogna, Martina Patera, Marco Falletti, Giulia Pinola, Francesco Asci, Antonio Suppa

TL;DR
This paper reviews technologies used to assess gait and balance in normal pressure hydrocephalus, highlighting their role in early detection and diagnosis.
Contribution
A systematic review of gait and balance assessment technologies for normal pressure hydrocephalus, emphasizing methodological diversity and gaps in longitudinal data.
Findings
NPH patients show significant kinematic differences in gait and balance compared to healthy controls.
Various tools like pressure-sensitive platforms and motion-capture systems are used to assess gait and balance in NPH.
Longitudinal data is lacking, limiting conclusions about prognosis.
Abstract
Normal pressure hydrocephalus (NPH) is a recognized cause of reversible cognitive and motor decline, with gait and balance impairments often emerging early. Technologies providing gait and balance measures can aid in early detection, diagnosis, and prognosis of the disease. This systematic review comprehensively discusses previous studies on the instrumental assessment of gait and balance in NPH. A PubMed search following PRISMA guidelines identified studies published between 2000 and 2024 that used laboratory instruments to assess gait and balance in NPH. Studies underwent quality assessment for internal, statistical, and external validity. Methodological details such as motor tasks, instruments, analytical approaches, and main findings were summarized. Overall, this review includes 41 studies on gait and 17 on balance, most of which used observational, cross-sectional designs. These…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
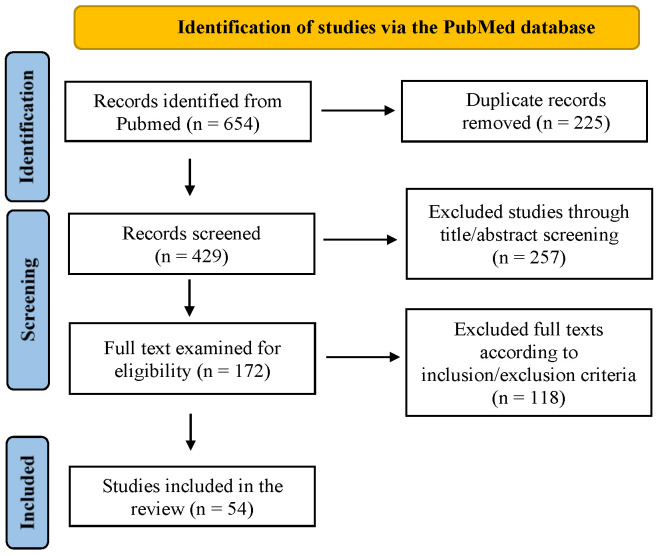 Figure 1
Figure 1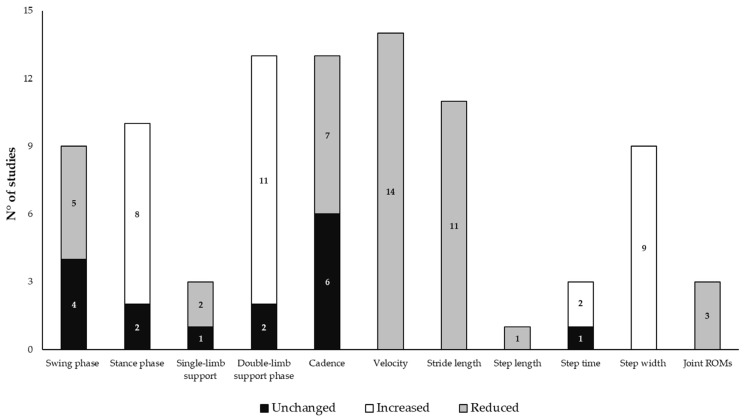 Figure 2
Figure 2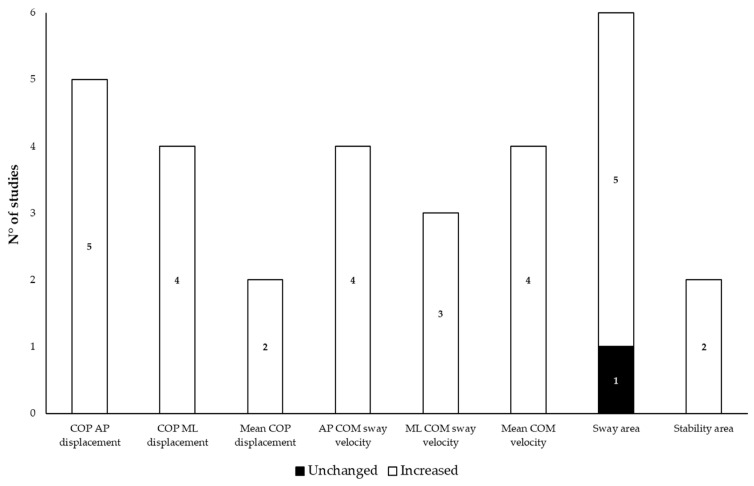 Figure 3
Figure 3- —European funding
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Spinal Dysraphism and Malformations · Fetal and Pediatric Neurological Disorders
1. Introduction
Idiopathic normal pressure hydrocephalus (NPH) is a neurological disorder affecting 3.7% of individuals over 65 and up to 5.9% over 80 [1,2]. It involves ventricular and/or subarachnoid space distension caused by increased cerebrospinal fluid (CSF), despite normal lumbar puncture pressures [3,4,5]. Patients typically present an insidiously progressive gait and balance disorder associated with urinary dysfunction and cognitive decline, often culminating in severe complications and death [5,6]. Temporary symptom relief following a lumbar puncture (tap test) aids diagnosis and predicts response to shunt surgery, which diverts excess CSF to another body site (e.g., peritoneal cavity, heart) [7]. Early treatment can reverse dementia and motor impairments, highlighting the critical need for prompt diagnosis [8].
NPH is underdiagnosed and poorly treated due to several clinical challenges [9]. Its variable presentation can lead to misdiagnosis, as motor signs like bradykinesia and freezing of gait can be mistakenly attributed to parkinsonian syndromes, which require different treatments [10]. Furthermore, while the tap test is commonly used to assess surgical candidates, some patients may benefit from shunt therapy even without obvious clinical motor improvement after acute deliquoration [11,12]. Indeed, although the tap test demonstrates high specificity (75%) and positive predictive value (92%), its low sensitivity (58%) and negative predictive value (37%) limit its accuracy in identifying suitable surgical candidates [13]. Additionally, the absence of reliable predictive measures for long-term surgical outcomes further underscores the need for objective motor assessments to identify NPH objectively and specifically and guide proper treatment decisions early.
Over the last two decades, researchers have increasingly adopted laboratory instruments to objectively assess gait and balance in patients with NPH [12,14,15,16,17,18,19,20,21]. Using different instrumental approaches, such as optoelectronic systems, wearable sensors, and dynamometric platforms and carpets, a large amount of standardized and comparable data have been collected in patients with NPH before and after the tap test and/or shunt surgery. Accordingly, despite not being routinely adopted into daily clinical practice, quantitative measures of gait and balance are already largely available and may help clinicians in the diagnostic and therapeutic management of NPH. Aligned with this observation, a recent meta-analysis examined the responsiveness of gait parameters to CSF drainage in NPH, supporting the use of gait analysis to select patients for shunt surgery [22]. In this systematic review, we have comprehensively summarized previous original studies that adopted laboratory instruments to objectively assess gait and balance in patients with NPH. More in detail, we first report methods and findings of studies assessing gait and balance in NPH objectively through laboratory instruments. Then, we critically examine and discuss the results of our systematic research to provide an up-to-date overview of the knowledge in this field and possible perspectives to improve the clinical management of patients with NPH. Our systematic review expands on previous works by exploring a broad range of analytical and clinical aspects. It analyzes both gait and balance abnormalities in NPH, in comparison not only to healthy controls but also to other neurological conditions. It also provides updated insights into emerging technologies driving advancements in both research and clinical practice. Lastly, it examines the pathophysiological mechanisms underlying gait and balance disorders in NPH.
2. Materials and Methods
This systematic review was performed according to the PRISMA statement [23] (Supplementary Materials Table S1).
2.1. Search Strategy
Two separate raters (A.Z. and M.P.) independently questioned the PubMed database to find previous original studies adopting laboratory instruments to objectively assess gait and balance in NPH. More in detail, the literature search aimed at the application of different technologies, such as wearable sensors, force platforms and computerized dynamic posturography, to the clinical appraisal of NPH. The queries used for the literature search included the following keywords and their reciprocal combination: (“normal pressure hydrocephalus” or “idiopathic normal pressure hydrocephalus”) and (“gait” or “balance”) and (“sensors” or “accelerometer” or “wearables” or “force platform” or “posturography” or “gait analysis” or “objective assessment”).
2.2. Study Selection and Quality Assessment
In this review, we included original studies assessing gait and/or balance in patients with NPH through laboratory instruments. We selected only articles written in English and published from January 2000 to October 2024. The inclusion of studies from 2000 onwards is based on the observation that most research on the topic has been conducted in the past 25 years, likely driven by advancements in technology. We excluded reviews, case reports, and conference proceedings, as well as studies whose full texts are not available or that used non-laboratory instruments, such as stopwatches, activity monitors, and video recordings. First, we examined the titles and abstracts of the articles to exclude duplicate records and off-topic papers. Then, we inspected all the full texts of the identified articles to assess their eligibility based on our inclusion/exclusion criteria. We also checked the reference lists of all the identified articles to collect additional relevant papers possibly missed in the electronic database search.
Following PRISMA guidelines [23], we conducted a quality assessment of the included studies using a 17-item checklist tailored to our topic [24,25,26,27]. The checklist evaluated the internal, statistical, and external validity of the studies (see Supplementary Materials Table S2 for details). The evaluation was independently conducted by two raters (A.Z. and M.P.). Any disagreements were reviewed by two additional raters (M.F. and G.P.) and resolved through collegial discussion to reach a consensus. Each question was rated as “Yes” (2 points), “No” (0 points), or “Not Completely” (1 point), with a maximum score of 34. Studies were categorized as high quality (≥27/34), medium quality (≥20/34), or low quality (<20/34) based on their total score, in accordance with established procedures [27].
3. Results
3.1. Search Results and Study Selection
Our query retrieved 654 potentially eligible articles for the systematic review. After removing 225 duplicates, we screened titles and abstracts, excluding 257 articles (e.g., off-topic articles, pre-2000 studies, conference proceedings, and non-laboratory studies). Following a full-text review based on the inclusion/exclusion criteria, we excluded 118 articles. Manual reference searches identified two relevant studies. This process resulted in the inclusion of 54 articles: 41 on gait assessment and 17 on balance in NPH, with 4 addressing both. Figure 1 presents a flow diagram summarizing the search and screening strategy.
3.2. Gait in NPH
Table 1 summarizes the main methods and findings of the 41 selected articles focused on the objective assessment of gait through laboratory instruments.
3.2.1. Methodological Approach
The size and sample population characteristics were variable across the 41 included studies in the objective evaluation of gait in NPH. Twenty-seven studies enrolled a limited number of patients with NPH with a size range of 4 to 42 patients [12,15,18,19,28,29,31,33,35,36,37,38,40,42,44,45,46,48,49,50,51,52,55,56,57,58,61], whereas only 14 studies included a large number of patients with a size range of 50 to 97 patients [14,16,17,30,34,39,41,43,47,53,54,59,60]. The enrolled patients with NPH overall showed a mean age of 75.4 ± 2.23 years. Twenty-three studies included a control group of age-matched healthy subjects (HS) [12,14,18,19,28,34,35,36,38,40,42,44,45,47,49,50,53,55,56,57,58,59,61]. Also, some authors (i.e., 6 studies) compared patients with NPH and those suffering from other neurological disorders, such as Parkinson’s disease (PD) [18,29,38,56,57], progressive supranuclear paralysis (PSP) [29,35], dementia, and other conditions responsible for hydrocephalus-like changes in gait [29,32,38].
Most studies (i.e., 31) assessed gait objectively before and after acute and/or chronic deliquoration [12,14,15,16,17,18,19,28,29,30,31,32,33,34,36,37,38,40,41,42,44,45,47,48,49,51,52,53,54,58,60]. More in detail, 26 studies used the tap test or transitory CSF drainage to assess the effects of acute deliquoration on gait in NPH [12,14,15,16,17,18,19,28,29,30,31,32,34,36,37,38,40,41,42,45,47,48,51,52,54,60]. Among these, seven studies also assessed gait changes due to chronic deliquoration in patients with NPH that underwent shunt surgery [12,15,19,37,38,40,41,48,49,51,52,53,58]. Only a few authors investigated the isolated effects of shunt surgery [33,44,49,53,58]. Lastly, 10 studies examined baseline gait parameters without considering the effects of deliquoration [35,39,43]. Among studies that used the tap test or transitory CSF drainage, most (i.e., 22 out of 26) specified that acute deliquoration involved the removal of at least 30 mL CSF (CSF range: 30–50 mL) [12,14,15,16,18,28,29,30,31,32,34,36,37,38,40,41,42,45,47,51,52,60], whereas four studies did not clarify this point [17,19,48,54].
When considering the effects of the tap test or transitory CSF drainage, some authors analyzed gait a few hours after the acute deliquoration (i.e., 1 to 8 h) [14,15,31,34,37,48,51,54], whereas others adopted a prolonged time for the re-assessment (i.e., 24 to 96 h) [12,16,17,18,19,28,29,30,31,32,36,38,40,41,42,45,47,48,52,54,60]. Similarly, patients with NPH who underwent shunt therapy were assessed 1 week to 6 months after surgery [15,19,37,40,41,48,51,52,58]. Only two articles did not specify the timing for clinical re-assessment after shunt surgery [49,53].
Concerning the motor tasks adopted to assess gait in NPH, most studies used free-speed locomotion along paths with different lengths (i.e., 3 to 18 m), including the timed up-and-go (TUG) test [14,16,18,19,28,29,30,32,33,34,35,36,37,38,39,40,41,42,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. Two articles collected data from 72 h of home-monitoring of patients and compared them with an experimental evaluation [50,58]. A few authors also assessed the effect of external cues [18] and cognitive functions (i.e., dual task) on gait [29,31,32,35,53,59,61]. Lastly, three studies analyzed possible changes in gait parameters with different walking velocities (i.e., preferred and maximal velocity) [31,59,61].
Concerning the objective evaluation of gait in NPH, we identified three main instrumental settings: i. pressure-sensitive systems [12,14,15,29,31,33,35,36,37,41,42,48,53,54,59,60], ii. wearable inertial sensors [16,19,30,34,38,39,40,44,45,47,48,49,50,51,52,57,58,61], and iii. optoelectronic systems [17,18,28,29,32,33,43,44,46,55,56]. Only a few authors adopted additional devices, such as a knee goniometer, optical infrared sensors, or punched-out peaks under shoe soles, imprinting footmarks on a draft paper, in combination with a pressure-sensitive or optoelectronic system [14,18,28,49]. Wearable inertial sensors included one to three tri-axial accelerometers and smartphones equipped with inertial sensing systems, positioned mostly on the waist, abdomen, and lower limbs [16,19,30,34,38,39,40,44,45,49,50,51,52,57,58,61], and rarely on the head and upper limbs [45,50,58,61]. Lastly, one author applied machine learning algorithms to inertial gait data, using a data-driven approach to classify pathological strides [50].
Key outcome measures of the selected studies included TUG duration [36,40,46,52,57]; gait cycle phases [12,14,15,16,18,28,29,34,37,42,43,48,50,51,52,53,55,57,58,59,60]; spatiotemporal kinematic parameters such as cadence, velocity, stride/step length/time/width/height, and gait variability indices [12,14,15,16,17,18,19,28,29,30,31,32,33,34,35,37,39,41,42,43,44,45,46,48,49,50,51,52,53,55,57,58,59,60]; plantar pressure variability[48]; body segment fluctuation [56]; and joint angles/ROM [14,15,18,28,33,37,42,47,50,51,52,57,58,60,61].
3.2.2. Main Findings
Compared to HS, patients with NPH had longer TUG test times, mainly due to an extended gait cycle, with notable prolongation of the double-limb support phase and shortened swing and single-limb support phases [12,14,18,28,34,38,40,42,50,53,57,59]. They also exhibited reduced cadence, velocity, stride length, and step length/width/height compared to HS [14,18,19,28,34,35,42,44,50,53,55,57,58,59]. The stride length/time coefficient of variation (CV) was increased [18,28,35,42,53,59], while the step time/width CV was reduced [18,19,35]. Additionally, patients had higher plantar pressure variability [48], altered heel-height variability [49], and significant fluctuations in all body segments [56] compared to HS. Regarding joint angles, increased toe-out angle and reduced range of motion in limb joints were observed [14,18,28,42,58,61]. Finally, gait parameters correlated with frontal cognitive functions [42,51], clinical scores [52,59], and radiological changes (e.g., temporal horn value, Evans index) [31,33,54].
Compared to patients with parkinsonian syndromes, those with NPH exhibited lower gait velocity, stride length, step height, gait variability, and joint range of motion, but higher step width and body fluctuation indexes than patients with PD or PSP [18,35,56,57]. Additionally, NPH patients experienced less gait impairment during dual-task conditions compared to those with PSP [35]. By contrast, Allali and colleagues found no significant differences in baseline spatiotemporal gait parameters between NPH patients and those with other conditions mimicking NPH, such as vascular, frontotemporal, and alcoholic dementia, under either single- or dual-task conditions [29].
Concerning the effects of acute and chronic deliquoration, most gait parameters, including the duration of the TUG test, gait cycle phases, and kinematic spatiotemporal parameters, improved after the tap test and/or shunt surgery in NPH [12,14,15,16,17,18,19,28,29,30,31,32,33,34,36,37,38,41,42,44,45,49,51,52,52,57,58,60]. The improvement in gait kinematics was higher in patients with NPH presenting a frontal-like gait than those with a parkinsonian-like gait [17]. The extent of parameter response to deliquoration was significantly correlated with the patients' Evans index (i.e., a radiological marker of ventricular volumes) [31,33]. A few authors reported a greater improvement in specific gait parameters, such as gait velocity, stance phase duration, stride length, and base width, following shunt surgery compared to the tap test [12,37,51]. Changes in the double-limb support phase duration, gait velocity, stride length, and cadence after acute deliquoration significantly correlated with the response to the shunt surgery [12,31,51]. Among these parameters, gait velocity and stride length were proposed as the most sensitive response marker to acute deliquoration in NPH [28,58]. Changes in step width were the most discriminative parameter among patients with NPH and those with mimicking conditions [29]. However, one study found that baseline spatiotemporal gait parameters could not differentiate between NPH patients who improved after acute deliquoration and those who did not [30]. Based on kinematic measures, some authors calculated specific indices and thresholds to differentiate NPH gait from that of HS. In particular, fluctuations in trunk tri-axial accelerations, reduced stride length and gait velocity, and an increase in the double support phase and stride length CV were significantly associated with the NPH pathological gait [47,53]. Some authors also applied machine learning algorithms for the automatic classification of stride profiles in patients with NPH [50].
Regarding the time of assessment after the tap test, a few authors showed that the main changes in spatiotemporal gait parameters in NPH occurred after 24–72 h after acute deliquoration, thus possibly demonstrating the existence of some false-negative results within the first 24 h [16,31,41,51]. Table 2 summarizes changes in the main kinematic measures of gait in patients with NPH before and after acute and/or chronic deliquoration, while Figure 2 displays the consistency of studies on the main findings when comparing patients to HS.
3.3. Balance in NPH
Table 3 summarizes the main methods and findings of the 17 selected articles focused on the objective assessment of balance through laboratory instruments.
3.3.1. Methodological Approach
Most of the studies concerning balance involved a limited number of NPH patients. In detail, 16 studies involved small cohorts ranging from 9 to 40 subjects, whereas only one study presented a larger cohort with a sample of 56 NPH patients [71]. The enrolled patients’ mean age was 72.2 ± 5.3 years.
Twelve studies included a control group of age-matched HS [20,21,55,57,61,62,63,64,65,66,68,69,70,72]. In contrast, six articles compared NPH patients to those affected by other neurological disorders, such as PD [57,72], ventriculomegaly [68], brain atrophy [62,64,65], and subcortical arteriosclerotic encephalopathy [20].
The effects of CSF drainage on balance performance were assessed in nine articles. More in detail, three studies reassessed the patients after isolated acute deliquoration [67,70,71], seven after shunt surgery [15,20,62,65,66,68,69], and two after both procedures [15,68]. Lastly, seven articles assessed baseline changes of balance in NPH patients without investigating the effects of CSF drainage [21,55,57,61,63,64,72].
Among the evaluated effects of acute deliquoration, postural abilities were examined less than 24 h [15,68,71] or 72 h [69] after the tap test procedure. Studies evaluating the effects of chronic deliquoration reassessed patients 1 week [65,69] or 3 months [15,20,66,68] after the shunt surgery. Only a few papers did not report any information about the time of assessment after acute or chronic deliquoration [62,67].
Concerning the motor tasks adopted to assess balance, postural abilities were mostly assessed during the upright stance or, alternatively, during a 5–10 m walking test [55,68] or the pull test [70]. Several authors explored the impact of sensory stimuli, such as vision, by having participants close their eyes [20,61,62,63,64,65,66,67,68], and proprioception, by asking patients to walk on foam surfaces [68]. A few others evaluated voluntary multidirectional leaning tasks [69,72].
Regarding the experimental setup, force platforms were the most adopted instruments to assess balance [20,21,62,63,64,65,66,67,69,72]. Alternative solutions included inertial sensors [15,57,68,70] or optoelectronic systems [55]. The main outcome measures described the main changes in center of pressure (COP) and center of mass (COM), including anteroposterior (AP) and mediolateral (ML) displacements [20,21,57,61,63,65,68]; mean COM/COP displacements, such as the locus length or the sway radius [61,62,64,65,69,72]; the sway area [15,20,57,61,62,65,69,72]; AP and ML sway velocities [20,21,55,57,63,68,71]; mean sway velocity [57,70,71]; and the stability area [21,69,71,72]. Other parameters reported were AP and ML maximum leaning distances during voluntary multidirectional leaning [69,72], AP and ML distances between COM and the base of support (COM-BOS distance) [55], and reaction times and COM acceleration during the pull test [70].
3.3.2. Main Findings
When examining baseline changes in balance, patients with NPH showed increased AP and ML sway [20,21,57,61,63], sway area [20,57,62,64,65,69,72], sway radius [62,64,65], and locus length [69,72] during quiet standing, as well as reduced AP and ML leaning distances during multidirectional leaning tests compared to HS [69,72]. Moreover, patients with NPH were characterized by higher sway velocities [20,21,57,63,68], lower COP stability areas [21,69,72], and worse balance performances under different sensory conditions (i.e., sensory organization test scores) than HS [66,67].
Concerning the comparison with other pathological conditions, balance assessment disclosed significant differences between patients with NPH and those affected by subcortical arteriosclerotic encephalopathy and brain atrophy. More in detail, compared to subcortical arteriosclerotic encephalopathy, patients with NPH showed higher AP displacement and lower AP/ML ratio and AP sway velocity when standing with feet together and eyes closed [20]. Also, NPH patients showed higher sway area/radius than patients with brain atrophy [64,65] and lower sway velocity during gait than patients with ventriculomegaly [68]. Compared to PD, NPH patients presented increased sway area [57,72], root mean square sway, and ML displacement [57]; reduced stability area; and increased locus length per unit area [72].
Regarding the effects of acute and chronic deliquoration, most studies consistently reported a significant improvement in balance parameters in patients with NPH. When considering acute deliquoration, Abram et al. reported increased composite sensory organization test scores (i.e., 2,4,5), associated with improved somatosensory and visual performances [67]. Among many parameters, authors reported improvement in the AP sway angle [68] and sway velocities [68,71], and a reduction in the base of support [71] during quiet standing, plus reduced AP/ML sway velocities during gait [68]. Similarly, patients with NPH who had undergone shunt surgery showed reduced sway area [20,62,65,68,69], sway radius [62,65], COP length trajectory [65], AP displacement [20], and increased stability area and leaning distances in the post-surgical period [69]. Conversely, only a minority of authors did not report any significant changes in postural abilities in patients with NPH after acute or chronic deliquoration [15,21,66].
Finally, several authors investigated the impact of visual deprivation on balance performance and obtained controversial results. In fact, in different studies, NPH patients showed both worse [20,61,63,64,66] and better postural performance [62,65,68] after eye closure compared to HS. The impact of eye closure after acute and chronic deliquoration was equally controversial: some authors reported improvement in postural response with eyes closed after CSF removal [66,67], while others described significant worsening [62,65,68].
Table 4 summarizes the main kinematic measures of balance in patients with NPH before and after acute and/or chronic deliquoration, while Figure 3 displays the consistency of studies on the main balance findings when comparing patients to HS.
3.4. Quality Assessment
Among the studies focused on gait evaluation, 17 (41%) were categorized as high quality, 23 (56%) as medium quality, and 1 (3%) as low quality. In comparison, studies assessing balance showed 8 articles (47%) classified as high quality and 9 (53%) as medium quality, with no studies falling into the low-quality category. Detailed results of the quality assessment for each study included in this review are provided in Supplementary Materials Table S2.
4. Discussion
Following PRISMA guidelines, this systematic review provides a concise overview of the current research on instrumental gait and balance assessments in NPH. We have demonstrated that a specific pattern of kinematic alterations affecting gait and balance can be instrumentally identified in patients with NPH compared to HS or other neurological conditions considered in the differential diagnosis. The adopted methodological transparency facilitates the replication of the review and enables readers to critically evaluate the strengths and limitations of instrumental approaches in this field. Additionally, a comprehensive quality assessment of the included studies minimizes potential biases and overinterpretation, offering a clear perspective on how existing findings might inform the clinical management of NPH.
4.1. Gait and Balance in NPH: Instrumental Assessment
While significant progress has been made in instrumentally characterizing gait and balance in NPH, substantial methodological heterogeneity is evident in the literature. When considering adopted technologies, different authors used several tools, including pressure-sensitive platforms, optoelectronic motion-capture systems, and wearable inertial sensors, each with specific strengths and limitations [73]. Platforms provide precise force and pressure data during both static and dynamic motor tasks but are limited to laboratory settings and can be relatively costly [74]. Similarly, optoelectronic systems capture detailed spatial–temporal parameters and joint kinematics with high accuracy but require complex setups [75]. Though less precise, wearable sensors measure spatial–temporal parameters of balance and gait and are highly portable, thus potentially enabling long-term and real-world monitoring of movement [74]. Given abnormal intracranial pressure fluctuations in NPH, as shown through intraventricular devices [76], wearable sensors could be a valuable research tool for long-term movement monitoring in real-life conditions, benefitting from their ease of use and affordability [77]. In addition to the instrumental heterogeneity, there is variability in the motor tasks, including pathways of different lengths to assess gait at varying speeds and postural exercises under different visual conditions to evaluate balance. Moreover, an additional methodological source of variability is the timing of gait and balance assessments following CSF drainage. Only a minority of authors have adhered to current recommendations, which advocate for multiple evaluations within the first week after acute deliquoration, including assessments within 24 h (i.e., 2–4 h), the following day, and up to 7 days after [5,78,79]. Lastly, data analysis approaches have also varied. While some studies have performed classic statistical comparisons between groups, other authors have applied advanced machine learning methods, suggesting potential applications [50,80]. Machine learning techniques offer promising opportunities for improving data analysis in NPH by analyzing and merging extensive datasets from clinical, imaging, and sensor measurements, potentially helping to identify patterns and predict outcomes with greater accuracy [81,82]. Overall, the high variability in assessment tools and experimental protocols affects the comparability and reproducibility across investigations. This underscores the need for standardized approaches, as also emphasized by a recent meta-analysis addressing the topic of gait analysis in NPH [22].
When specifically focusing on gait, the reviewed studies identified several abnormalities in spatiotemporal and kinematic parameters in patients with NPH, such as prolonged double-limb support phase and increased step width, associated with reduced gait velocity and stride length [22]. Some discrepancies exist among studies when examining cadence [18,42,57], although a recent meta-analysis provided statistical evidence of a significant reduction in this feature in patients with NPH compared to HS [22]. Overall, most studies identify a set of kinematic gait alterations that differentiate patients with NPH from HS and individuals with other neurological conditions associated with hypokinetic gait, such as PD and atypical parkinsonism [14,18,19,28,34,35,42,45,50,53,55,57,58,59]. While these kinematic alterations alone are not specific to a distinct disease, their combination may suggest a possible movement profile characteristic of NPH. This composite gait pattern could aid in the disease assessment and management of patients, providing objective measures of movement impairment that may help guide treatment decisions and monitor disease progression over time [61]. Most kinematic parameters partially improved following acute and chronic CSF drainage, supporting their potential utility also for treatment outcome monitoring. In particular, changes in gait velocity appear to be the most consistently reported and sensitive measure in NPH patients who respond positively to CSF drainage [22]. Gait velocity is a widely recognized measure of motor performance and functional mobility, which is particularly valuable in the assessment of neurological disorders and ageing-related conditions [83]. Generally, in neurological diseases, reduced gait velocity correlates with disease severity, fall risk, and decreased quality of life [84,85]. Similarly, when examining balance, increased anteroposterior and mediolateral sway, larger sway areas, and reduced leaning distances partially improved after acute and chronic deliquoration. Partial improvement in balance after shunting may reduce fall risk in NPH patients [39]. However, balance relies on complex brain networks, and the suboptimal response to interventions is due to several factors [74]. Cognitive impairments, common in these patients, often lead to poor responses to CSF drainage [86]. Additionally, peripheral and/or central vestibular dysfunctions contribute to postural instability and reduce the effectiveness of therapeutic interventions [39]. Overall, the incomplete recovery of gait and balance abnormalities suggests that other factors beyond intracranial pressure, possibly irreversible, may contribute to motor dysfunction in NPH [87].
4.2. Pathophysiological Insights from Gait and Balance Kinematics in NPH
Despite heterogeneous methodological approaches, studies highlighted a distinctive pattern of walking and balance impairments in patients with NPH. Specifically, gait in NPH is characterized by small, “magnetic” steps (i.e., shuffling gait) with a broad base of support, reduced walking speed, and increased stride length variability. Both static and dynamic postural control are compromised, as evidenced by heightened multidirectional oscillations during upright stance and diminished functional stability during body excursions. Notably, patients with NPH often exhibit extra-rotated feet during gait, resembling a “duck-footed” walking pattern. This adaptation likely serves as a compensatory mechanism to enhance stability by widening the base of support and prolonging the double-limb support phase. Pathophysiologically, several factors, including hypoperfusion, glymphatic impairment, disturbance of metabolism, astrogliosis, neuroinflammation, and blood–brain barrier disruption, jointly participate in NPH clinical development and kinematic abnormalities [88]. The mechanical stretching and compression of neural fibers adjacent to the lateral ventricles, potentially extending to brainstem structures such as the pedunculopontine nucleus, has been suggested as a possible trigger factor [89]. Previous studies have demonstrated reduced cerebral perfusion in different key regions involved in gait and balance, including the basal ganglia, frontal lobes, and temporal lobes [78,90,91,92,93], which is possibly linked to the mechanical stress on the parenchyma and blood vessels induced by ventricular enlargement. In line with this hypothesis, deliquoration could restore cerebral perfusion in these areas, leading to clinical improvement in patients with NPH [93]. Most studies reviewed herein have demonstrated significant changes in various spatiotemporal gait parameters following both acute and chronic deliquoration in NPH. Notably, some of these changes correlated with ventricular volumes and the clinical phenotype of gait impairment, with frontal-like dysfunction showing greater responsiveness to deliquoration [17,33,53]. Consequently, quantitative gait parameter changes after acute deliquoration may serve as a sensitive tool for monitoring therapeutic outcomes, complementing their utility in the diagnostic process by reflecting underlying brain abnormalities and differing therapeutic responses. Indeed, identifying the neurophysiological changes and brain regions associated with abnormal gait and balance kinematics could help clinicians better interpret instrumental findings, supporting more accurate differential diagnoses, therapeutic interventions, and tailored rehabilitation strategies.
A noteworthy clinical challenge lies in the differential diagnosis of NPH and neurodegenerative disorders that present with overlapping symptoms, such as parkinsonian syndromes and other neurodegenerative conditions. Patients with NPH often exhibit parkinsonian signs, including bradykinesia, rigidity, and a small-step gait [89]. The differential diagnosis between NPH and other parkinsonian disorders is challenging, due to the similar clinical presentation and the transient gait improvement observed in some cases of vascular parkinsonism after acute deliquoration [79]. Parkinsonian features in NPH likely stem from hypoperfusion of the basal ganglia rather than classical dopaminergic cell loss [92], as suggested by abnormalities in nigrostriatal dopaminergic imaging (e.g., DAT scans) and the lack of response to levodopa treatment [94,95,96]. Other pathological conditions presenting radiological or clinical similarities to NPH are vascular or neurodegenerative dementias, such as subcortical arteriosclerotic encephalopathy, brain atrophy, or Alzheimer’s disease. Concerning the latter, NPH can sometimes coexist with Alzheimer’s disease, likely due to the similar age of onset and potential shared pathophysiological mechanisms. It has been hypothesized that abnormal CSF production and turnover in NPH may impair the clearance of amyloid–beta peptides and tau protein from the brain interstitial fluid space [97], a process that is further exacerbated by reduced cerebral venous compliance [98]. Together, these factors could contribute to neuronal dysfunction and reduced survival, potentially initiating a neurodegenerative cascade [97]. However, these remain hypotheses that are not yet supported by sufficient data, and the studies included in this review do not provide comparisons between NPH and Alzheimer’s disease patients.
As a final observation, this review confirms controversies about visual deprivation on balance in NPH. Indeed, some studies have reported that postural performance in NPH paradoxically does not deteriorate with eye closure [99]. The neural control of postural stability depends on the integration of somatosensory, vestibular, and visual inputs, and maintaining equilibrium requires coordinating these systems to produce motor strategies that maintain the COM in a stable range to prevent falls [70]. It has been suggested that balance in patients with NPH does not worsen following eye closure owing to possible hyper-compensation by specific neural networks in response to the baseline impairment of postural control. In line with this hypothesis, increased bilateral activation of the supplementary motor area has been observed in patients who do not exhibit worsened performance following visual deprivation [99]. A similar hypothesis has been suggested to explain the observation that patients with NPH demonstrate improved gait velocity during dual motor tasks compared to PSP patients, likely due to compensatory hyperactivity of the prefrontal cortex [35].
Although conducted according to rigorous methodological standards, this systematic review has some limitations that must be acknowledged. As previously highlighted, the primary challenge in reaching clear conclusions stems from the significant heterogeneity in study designs, methodologies, and patient populations, which complicates the comparability and generalizability of the findings. Variations in how gait and balance are assessed, differences in patient demographics, and diverse treatment protocols make it difficult to draw consistent conclusions across studies. Moreover, many studies rely on cross-sectional or retrospective designs, which limit the ability to establish causality or assess long-term outcomes effectively. Finally, there is a lack of high-quality, prospective studies that explore the long-term prognostic value of instrumental measures of gait and balance abnormalities in NPH patients.
5. Conclusions
This systematic review analyses the literature on instrumental gait and balance assessment in NPH, focusing on studies using laboratory equipment and wearable technologies. Numerous studies have identified quantitative measures of gait and balance disorders that could aid in early detection and differential diagnosis of NPH. These studies also highlight how specific kinematic measures change in response to common CSF drainage therapies. Although no single kinematic measure is uniquely associated with NPH, a complex pattern of gait and balance abnormalities appears to be more distinctive of the condition, offering potential value in clinical management. However, evidence remains limited regarding reliable predictive markers for shunt surgery outcomes. Most studies have short-term follow-ups, hindering a full understanding of how gait and balance improvements correlate with long-term recovery or quality of life. Further key limitations in available studies include uneven group sizes, inconsistencies in study design and preparation, and challenges in selecting homogeneous groups of patients. Also, in terms of analytical approaches, reliance on traditional statistical methods, the requirement for balanced data sets, and the underutilization of AI for advanced classification and predictive analysis remain notable constraints. More research is therefore needed to establish how kinematic measures of balance and gait can predict surgical success in patients with NPH. Future studies should adopt standardized protocols and include larger, more diverse cohorts to improve the reliability and clinical relevance of the findings. Moreover, efforts should aim to bridge the gap between traditional methods and modern approaches, such as machine learning, to enable meaningful comparisons across periods and populations. Developing novel computational parameters, like fractal dimensions reflecting gait uniformity, could also offer significant potential for deeper insights and improved population monitoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andersson J. Rosell M. Kockum K. Lilja-Lund O. Söderström L. Laurell K. Prevalence of Idiopathic Normal Pressure Hydrocephalus: A Prospective, Population-Based Study P Lo S ONE 201914 e 021770510.1371/journal.pone.021770531141553 PMC 6541279 · doi ↗ · pubmed ↗
- 2Jaraj D. Rabiei K. Marlow T. Jensen C. Skoog I. WikkelsøC. Prevalence of Idiopathic Normal-Pressure Hydrocephalus Neurology 2014821449145410.1212/WNL.000000000000034224682964 PMC 4001197 · doi ↗ · pubmed ↗
- 3Rekate H.L. The Definition and Classification of Hydrocephalus: A Personal Recommendation to Stimulate Debate Cerebrospinal Fluid Res.20085210.1186/1743-8454-5-218211712 PMC 2263019 · doi ↗ · pubmed ↗
- 4Fasano A. Espay A.J. Tang-Wai D.F. WikkelsöC. Krauss J.K. Gaps, Controversies, and Proposed Roadmap for Research in Normal Pressure Hydrocephalus Mov. Disord. Off. J. Mov. Disord. Soc.2020351945195410.1002/mds.2825132959936 · doi ↗ · pubmed ↗
- 5Nakajima M. Yamada S. Miyajima M. Ishii K. Kuriyama N. Kazui H. Kanemoto H. Suehiro T. Yoshiyama K. Kameda M. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus Neurol. Med. Chir.202161639710.2176/nmc.st.2020-0292 PMC 790530233455998 · doi ↗ · pubmed ↗
- 6Toma A.K. Stapleton S. Papadopoulos M.C. Kitchen N.D. Watkins L.D. Natural History of Idiopathic Normal-Pressure Hydrocephalus Neurosurg. Rev.20113443343910.1007/s 10143-011-0316-721594683 · doi ↗ · pubmed ↗
- 7Halperin J.J. Kurlan R. Schwalb J.M. Cusimano M.D. Gronseth G. Gloss D. Practice Guideline: Idiopathic Normal Pressure Hydrocephalus: Response to Shunting and Predictors of Response: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology Neurology 2015852063207110.1212/WNL.000000000000219326644048 PMC 4676757 · doi ↗ · pubmed ↗
- 8Tipton P.W. Elder B.D. Cogswell P.M. Graff-Radford N. Normal Pressure Hydrocephalus, or Hakim Syndrome: Review and Update Neurol. Neurochir. Pol.20245882010.5603/pjnns.9734338054275 · doi ↗ · pubmed ↗