Estimated Blood Loss in Surgery for Thoracolumbar Fracture With Diffuse Idiopathic Skeletal Hyperostosis Using Percutaneous Pedicle Screws Compared to Surgery for Femoral Trochanteric Fractures
Megumu Kawai, Takeshi Sasagawa

TL;DR
The study compares blood loss in spinal surgery for thoracolumbar fractures with DISH using percutaneous screws to hip surgery for femoral fractures in elderly patients.
Contribution
The study provides a novel comparison of estimated blood loss in two different surgical procedures involving elderly patients.
Findings
Estimated blood loss was comparable between thoracolumbar and femoral surgeries.
Hidden blood loss was significantly less in thoracolumbar surgeries using percutaneous screws.
In thoracolumbar surgeries, hidden blood loss accounted for 71% of total estimated blood loss on day one.
Abstract
Introduction: Long posterior spinal stabilization is often needed for thoracolumbar fractures with diffuse idiopathic skeletal hyperostosis (DISH). Recently, surgery using percutaneous pedicle screws (PPS) has become more frequent. However, hidden blood loss (HBL) cannot be ignored in surgeries using PPS. The aim of this study was to measure estimated blood loss (EBL) including HBL in surgeries using PPS for thoracolumbar fractures with DISH, by comparing with EBL including HBL in surgeries for femoral trochanteric fractures, a common trauma among elderly people. Materials and methods: Twenty-two patients who underwent surgery using PPS for thoracolumbar fracture with DISH were included (group D). Sixty-six patients with trochanteric fractures of the femur were matched to group D for age, sex, anticoagulant use, height, and weight and used as controls (group F). We evaluated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
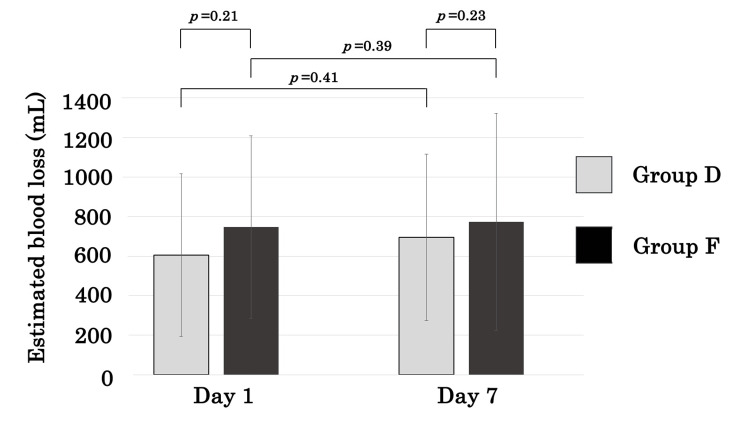 Figure 1
Figure 1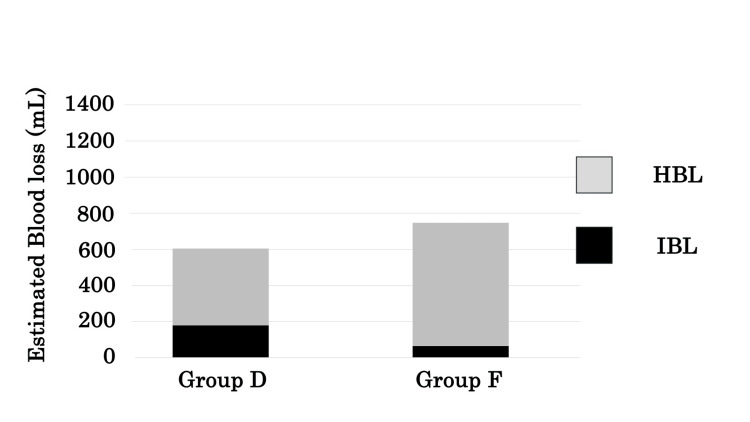 Figure 2
Figure 2| Injured level | Number of patients, n |
| T6 | 1 |
| T7 | 1 |
| T8/9 | 1 |
| T9 | 2 |
| T10 | 1 |
| T11 | 3 |
| T12 | 5 |
| T12/L1 | 1 |
| L1 | 5 |
| L2 | 1 |
| L3 | 1 |
| Group D | Group F | P | |
| Number | 22 | 66 | |
| Age, years | 77.0±10.0 | 78.4±12.8 | 0.55 |
| Male, n (%) | 18 (81.8) | 54 (81.8) | 1.00 |
| Height (m) | 1.60±0.09 | 1.61±0.09 | 0.89 |
| Weight (kg) | 60.6±13.4 | 57.7±8.1 | 0.43 |
| Anti-coagulant medication, n | 5 | 15 | 1.00 |
| Group D (n=22) | Group F (n=66) | P | |
| Hb before operation (g/dL) | 12.3±1.6 | 11.6±2.0 | 0.88 |
| Transfusion (units) | 0.8±1.2 | 1.4±1.9 | 0.31 |
| Hb on postoperative day 1 (g/dL) | 10.4±1.6 | 9.6±1.8 | 0.03* |
| Hb on postoperative day 7 (g/dL) | 10.8±1.4 | 9.8±1.5 | 0.01* |
| EBL on postoperative day 1 (mL) | 605.1±410.4 | 747.7±461.5 | 0.21 |
| EBL on postoperative day 7 (mL) | 695.8±421.1 | 773.0 ±548.8 | 0.23 |
| IBL (mL) | 178.1±163.0 | 63.3 ±93.4 | <0.01* |
| HBL (mL) | 427.0±429.6 | 684.4 ±203.5 | 0.03* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip disorders and treatments · Hip and Femur Fractures · Bone and Joint Diseases
Introduction
Thoracolumbar fractures with diffuse idiopathic skeletal hyperostosis (DISH) often do not achieve bony fusion using conservative treatment [1]. Therefore, posterior spinal stabilization may be needed in such cases. Longer fusions spanning three levels above and three levels below are recommended because of the long lever arm associated with bony ankylosis among patients with DISH [2]. These patients are mostly elderly males and often have diabetes or obesity as an underlying condition [3]. Worldwide, mortality rates from 8% to 32% have been reported in this population using conventional open surgery [2,4]. In Japan, a mortality rate of 12% has been reported [5]. Hence, the invasiveness of conventional open surgery is an issue for elderly patients with underlying diseases.
Recently, posterior spinal stabilization with percutaneous pedicle screws (PPS) has become more frequent because it is less invasive. Intraoperative blood loss (IBL) during surgery using PPS is reported as 134-167 mL, significantly less than the 500-1240 mL in conventional surgery [5,6]. However, not only IBL but also hidden blood loss (HBL) cannot be ignored in surgery using PPS [7]. HBL is invisible blood loss caused by hemolysis and extravasation of blood into tissues [8]. Therefore, studies of estimated blood loss (EBL) including HBL are necessary in order to assess blood loss in surgery using PPS. To the best of our knowledge, there are no reports on EBL including HBL in posterior spinal stabilization using PPS for thoracolumbar fractures with DISH. Therefore, it is not clear whether EBL in this procedure is acceptable for surgeries involving the elderly population. The aim of this study was to examine whether EBL in posterior spinal stabilization using PPS for thoracolumbar fractures with DISH is reasonable for the elderly, by comparing it with EBL in trochanteric fractures of the femur, a common surgery for the elderly.
Materials and methods
The medical ethics committee of our hospital approved the present study. All patients provided informed consent to use all patient data. This investigation was a retrospective study using electronic medical records. Twenty-two patients who underwent posterior spinal stabilization using PPS for thoracolumbar fracture with DISH between January 2015 and January 2023 were included (group D). Exclusion criteria included patients who underwent conventional open surgery, those with other trauma requiring surgery, those with hemothorax requiring a chest drain, and the lack of a complete data set. Fractures at various vertebral levels are shown in (Table 1).
Spinal stabilization with PPS was performed between three levels above and three levels below the fracture in all patients but not at the fracture level. Three patients also underwent posterior decompression. In these cases, posterior decompression with a median incision was performed after spinal stabilization with PPS.
A total of 66 patients with trochanteric fractures of the femur were matched to group D for age, sex, anticoagulant use, height, and weight and used as controls (group F). All 66 patients in group F underwent osteosynthesis. We evaluated IBL, EBL on the first and seventh postoperative days, and HBL on the first postoperative day. Each variable was compared between the study groups. IBL was evaluated by the measured suction loss plus the weight of loss in gauze. EBL was calculated using the Nadler formula [9] shown below based on Hb values. HBL was calculated as the difference between EBL on the first postoperative day and IBL. The Nadler formula is defined by
Women’s blood volume (L)=height (m)^3^×0.356+weight (kg)×0.033+0.183;
Men’s blood volume (L)=height (m)^3^×0.367+weight (kg)×0.032+0.604;
Hb_loss (g)=blood volume (L)×(Hb_pre (g/L)-Hb_post_ (g/L))+26.5 (g)×(transfusion unit);
EBL (mL)=(Hb_loss_ (g)/Hb_pre_ (g/L))×1000;
HBL (mL)=EBL_day 1_ (mL)-IBL (mL);
Hb_pre_: Hb before surgery; Hb_post_: Hb one or seven days after surgery; EBL_day 1_: EBL on day one.
All data are expressed as mean ± standard deviation. A Mann-Whitney U test and a chi-square test were used to compare data. Differences with p<0.05 were considered significant. All statistical analyses were conducted using IBM SPSS Statistics for Windows (version 22; IBM Corp, Armonk, NY).
Results
The average age was 77 years in group D and 78 years in group F. In both groups, 82% were male, and 23% took anticoagulant or antiplatelet medication. There were no significant differences in body size (Table 2).
EBL was not significantly different between the two groups on either postoperative day one or day seven (Figure 1, Table 3). Although EBL on day seven tended to be higher than on day one in both groups, the differences were not statistically significant (Figure 1). IBL in group D was significantly greater than in group F (p<0.01). In contrast, HBL in group D was significantly less than in group F (p=0.03, Table 3). In group D, HBL accounted for 71% of EBL on day one, whereas in group F, it accounted for 92% (Figure 2).
Comparisons of EBL between groups.EBL, estimated blood loss
*Table 3: Perioperative outcomes in each group. p<0.05EBL, estimated blood loss; IBL, intraoperative blood loss; HBL, hidden blood loss
The percentage of EBL accounted for by HBL and IBL in groups D and F. EBL, estimated blood loss; IBL, intraoperative blood loss; HBL, hidden blood loss
Discussion
EBL in posterior spinal stabilization using PPS for thoracolumbar fractures with DISH was not different from that in surgery for trochanteric fractures of the femur. Surgical treatment of thoracolumbar fractures with DISH often is performed due to the risk of nonunion and delayed paralysis associated with conservative management. Despite the fact that surgery using PPS for thoracolumbar fractures with DISH requires fusions covering several vertebral levels, EBL was the same as in surgery for trochanteric fractures of the femur, and therefore, acceptable for elderly patients.
Sheat et al. first reported the importance of HBL in orthopedic surgery for knee joint prostheses [10]. Recently, HBL in surgery using PPS for thoracolumbar fractures without DISH has also been reported several times [7,8,11]. In these studies, HBL accounted for 68-85% of EBL [7,8,11], which is very similar to the current study (71%).
In this study, EBL was not significantly different between groups. However, HBL in group F was greater than in group D, while IBL in group D was greater than in group F. Therefore, the etiologies of perioperative bleeding were different between the groups. HBL in surgery for spine fractures is correlated with the degree of fracture dislocation and reposition [12] and is caused by blood infiltration into the soft tissue or the postoperative muscle space [12]. Moreover, according to Zhou et al., muscle thickness is a risk factor for HBL [13]. In that study, most cases exhibited minimal preoperative dislocation. Fractures were mostly located at the thoracolumbar junction where the soft tissue is relatively thin. Therefore, despite a large IBL due to the length of the stabilization (three levels above and three levels below), HBL was not greater than in surgery for femoral trochanteric fractures. Ren et al. reported that topical use of tranexamic acid can reduce HBL in posterior lumbar spinal fusion surgery without significant complications [14]. However, there is no report of the effect of tranexamic acid for posterior stabilization using PPS for thoracolumbar fractures with DISH. Therefore, it is necessary to examine whether tranexamic acid is effective in reducing HBL in cases of DISH.
The importance of HBL in surgery for trochanteric fractures of the femur also has been reported [15-18]. Smith et al. reported that most of the HBL in proximal femoral fractures was preoperative [17]. Similarly, Guo et al. reported that intramedullary fixation does not cause a large amount of HBL in femoral fractures, rather bleeding from the fracture site is the main cause of HBL [18]. In this study, the proportion of HBL in EBL was 92% and the proportion of IBL was 8%, suggesting that bleeding was caused primarily by the fracture, not the surgery.
Transfusions of 0.8-1.4 units on average were required in both groups in the perioperative period. Sasagawa et al. reported that EBL on day seven tended to be less than on day one postoperatively when using PPS for traumatic thoracolumbar fractures in a younger population, and no patients required transfusion [11]. On the other hand, in our study, the average age was 77-78 years, relatively older than in their report. EBL on day seven tended to be higher than on day one in both groups. Zhou et al. reported that the amount of HBL is correlated with age [13], reasoning that bleeding is liable to infiltrate more easily into interstitial spaces and agglutinate there owing to muscle wastage [13,19]. Additionally, hematopoiesis in the elderly is lower than in the younger population [20]. Consequently, EBL may increase over time in the elderly because of the persistence of postoperative invisible bleeding and low hematopoiesis. Postoperative anemia in the elderly may lead to disorders of the brain, heart and kidneys, infections [21], and delirium [22]. Therefore, sustained monitoring of postoperative hemoglobin levels is essential in the elderly population.
There were some limitations to the present study. First, the sample size is small. If the sample size were larger, factors resulting in increased EBL might be examined. Second, the days between injury and surgery varied among patients so the assessment of surgical invasiveness is not only based on the amount of blood loss. To understand the blood loss in surgery using PPS for thoracolumbar fractures with DISH, further study is required.
Conclusions
We measured EBL in posterior spinal stabilization for thoracolumbar fractures with DISH in elderly patients by comparing it with EBL in surgery for trochanteric fractures of the femur, a common trauma among elderly people. EBL in surgery for thoracolumbar fracture with DISH using PPS is comparable to that for trochanteric fractures of the femur. Therefore, even though surgery using PPS for thoracolumbar fractures with DISH requires fusions covering several vertebral levels, this is an acceptable procedure for elderly patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Conservative treatment for stable low-energy thoracolumbar vertebral fractures in nonfused segments among elderly patients with diffuse idiopathic skeletal hyperostosis: a matched case-control study Medicine (Baltimore) Okano I Tachibana T Nishi M 098201910.1097/MD.0000000000016032 PMC 658762531192958 · doi ↗ · pubmed ↗
- 2Spine fractures in patients with ankylosing spinal disorders Spine (Phila Pa 1976) Caron T Bransford R Nguyen Q Agel J Chapman J Bellabarba C 06435201010.1097/BRS.0b 013e 3181 cc 764f 20421858 · doi ↗ · pubmed ↗
- 3Risk factors for diffuse idiopathic skeletal hyperostosis: a case-control study Rheumatology (Oxford) Kiss C Szilágyi M Paksy A Poór G 27304120021179287610.1093/rheumatology/41.1.27 · doi ↗ · pubmed ↗
- 4Injuries of the cervical spine in patients with ankylosing spondylitis: experience at two trauma centers J Neurosurg Spine Einsiedel T Schmelz A Arand M 3345520061685095410.3171/spi.2006.5.1.33 · doi ↗ · pubmed ↗
- 5Spinal fractures in diffuse idiopathic skeletal hyperostosis: advantages of percutaneous pedicle screw fixation J Orthop Surg (Hong Kong) Okada E Shiono Y Nishida M 23094990198434072720193107956310.1177/2309499019843407 · doi ↗ · pubmed ↗
- 6Perioperative complications in open versus percutaneous treatment of spinal fractures in patients with an ankylosed spine J Clin Neurosci Moussallem CD Mc Cutcheon BA Clarke MJ 88923020162703885410.1016/j.jocn.2016.01.020 · doi ↗ · pubmed ↗
- 7Comparison of hidden blood loss between three different surgical approaches for treatment of thoracolumbar fracture J Invest Surg Chen ZX Sun ZM Jiang C Zhang H Tong MJ Lin Y Wu YS 7557603220192967217510.1080/08941939.2018.1458925 · doi ↗ · pubmed ↗
- 8Hidden blood loss during perioperative period and the influential factors after surgery of thoracolumbar burst fracture: a retrospective case series Medicine (Baltimore) Yin M Chen G Yang J 098201910.1097/MD.0000000000014983 PMC 645582130921207 · doi ↗ · pubmed ↗