Feasibility of Proton Beam Therapy for Para-Aortic Lymph Node Recurrence in Patients With Gynecologic Cancer After Pelvic Irradiation: A Case Series
Yuka Mizuno, Ayumi Shikama, Kaoru Fujieda, Hiroya Itagaki, Yuri Tenjimbayashi, Yusuke Kobayashi, Tsukasa Saida, Takashi Saito, Hideyuki Sakurai, Toyomi Satoh

TL;DR
This study explores using proton beam therapy to treat lymph node cancer recurrence in gynecologic cancer patients who have already had pelvic radiation.
Contribution
The study demonstrates the feasibility and safety of proton beam therapy in managing para-aortic lymph node recurrence after prior pelvic irradiation.
Findings
Proton beam therapy achieved favorable local control with minimal overlap of irradiated fields in most patients.
Adverse events were observed but linked to prior pelvic irradiation rather than the proton therapy itself.
Four patients showed no re-enlargement of treated lymph nodes after proton therapy.
Abstract
Aim: Irradiation of para-aortic lymph node recurrences in patients with prior pelvic irradiation raises concerns about overlapping irradiated fields, which should be minimized to reduce severe adverse events. We report six gynecologic cancer patients treated with proton beam therapy for para-aortic lymph node recurrence after pelvic irradiation. Methods: Six patients who received proton beam therapy for para-aortic lymph node recurrence after pelvic irradiation between 2010 and 2022 were included. Overlapping fields were assessed using the 50% dose distance between the initial and proton therapy fields. Results: A 5- to 10-mm overlap was observed in three patients. Grade 2 rectal hemorrhage occurred in three patients, grade 3 hematuria in two, and grade 4 sigmoid perforation in one. These adverse events were linked to pelvic irradiation and peritoneal dissemination. Among five…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
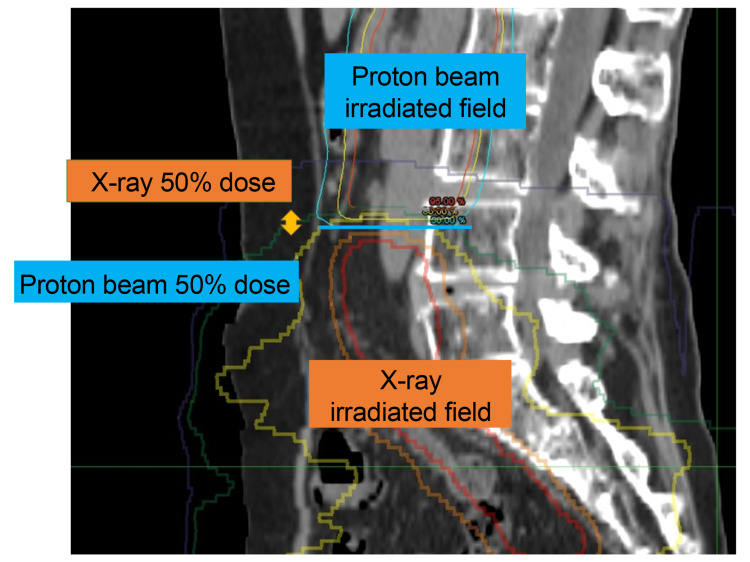 Figure 1
Figure 1| Case | Primary | Histology | Initial treatment | Treatment for recurrence | |||||||||
| Treatment | Irradiation range | Irradiation dose (Gy/fr) | Age at recurrence (years) | Time from treatment completion to recurrence (months) | Site of recurrence | Short axis of PALN (mm) | 50% dose distance between irradiated and PBT fields (mm) | PBT dose (Gy/fr) | Concurrent | Best response | |||
| CDDP | |||||||||||||
| 1 | Cervix | SCC | CCRT (X-ray) | Pelvic to L5 | 50/25 | 63 | 23 | PALN | 10 | -2: Separate | 56/28 | No | CR |
| 2 | Cervix | Adenosquamous carcinoma | Surgery → CCRT (IMRT) | Pelvic to L4 | 50.4/28 | 59 | 11 | PALN, mediastinal LN*1 | 12 | 5: Overlap | 60/30 | Yes | PD (new lesions: supraclavicular LN) |
| 3 | Cervix | Mucinous carcinoma (gastric type) | Surgery → CCRT (X-ray) | Pelvic to S1 | 50/25 | 63 | 24 | PALN | 17 | 9: Overlap | 56/28 | Yes | CR |
| 4 | Cervix | Mucinous carcinoma (gastric type) | CCRT (X-ray) | Pelvic to L5 | 50/25 | 60 | 4 | PALN | 15 | 0: Separate | 60/30 | No | SD |
| 5 | Vulva | Pagetoid spreading tumor | CCRT (IMRT) | Pelvic to L5, inguinal LNs, vulva | 60/30 | 42 | 14 | PALN | 8 | 10: Overlap | 56/28 | No | PD (new lesions: external iliac LN) |
| 6 | Endometrium | Mixed carcinoma*2 | Surgery → CT → RT (X-ray) | Pelvic to S1 | 50/25 | 46 | 6 | PALN | 9 | Impossible to measure | 56/28 | Yes | PD (new lesions: lung) |
| PALN | |||||||||||||
| Case | During PBT | After PBT (months) | |||||
| Nausea | Diarrhea | Neutropenia | Rectal hemorrhage | Hematuria | Colonic perforation | Anemia | |
| 1 | N/A | N/A | N/A | Grade 2 (4) | Grade 3 (1) | Grade 4* | N/A |
| 2 | Grade 1 | N/A | N/A | N/A | N/A | N/A | N/A |
| 3 | Grade 2 | Grade 1 | N/A | N/A | N/A | N/A | N/A |
| 4 | N/A | Grade 2 | N/A | Grade 2 (4) | Grade 3 (3) | N/A | Grade 3 (4) |
| 5 | N/A | N/A | Grade 2 | Grade 2 (4) | N/A | N/A | Grade 3 (4) |
| 6 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Case | Site of progression after PBT (time in months) | Post-treatment | Time from completion of PBT to post-treatment (months) | Re-enlargement of PALN (months) | Overall survival after PBT (months) | Prognosis |
| 1 | Supraclavicular LN | N/A | N/A | No | 12 | Death |
| 2 | Supraclavicular LN | PBT (60 Gy/30 fr) | 2 | No | 34 | Alive with disease |
| 3 | Lung | TC-Bev | 21 | No | 34 | Death |
| 4 | Pelvic LN | N/A | N/A | Yes (7) | 13 | Death |
| 5 | External iliac LN | TC | 6 | No | 22 | Death |
| 6 | Lung | N/A | N/A | Yes (6) | 9 | Death |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Pelvic and Acetabular Injuries · Colorectal and Anal Carcinomas
Introduction
Patients with gynecologic cancer often develop para-aortic lymph node (PALN) recurrence after initial treatment, posing a significant challenge in the management of gynecologic cancers and impacting the outcomes and treatment strategies of patients. The incidence of PALN recurrence has been reported as 2.1% in patients with cervical cancer [1] and 1-3% in patients with endometrial cancer [2,3]. Although radiotherapy can offer curative treatment for PALN recurrence, irradiation of the PALNs may be avoided in patients with prior pelvic irradiation because the lower line of irradiation for PALN recurrence may overlap the upper line of pelvic irradiation. Attention should focus on the dose to overlapping irradiated fields to mitigate severe adverse events [4].
Proton beam therapy (PBT) delivers higher doses to tumors while minimizing irradiation to surrounding organs. In recent years, the efficacy of PBT for various cancers has been reported [5,6]. However, data regarding the feasibility of PBT for recurrent gynecologic cancers remain limited [7].
This study reports on six gynecologic cancer patients treated with PBT for PALN recurrence after pelvic irradiation to reduce the risk of adverse events.
Materials and methods
Patients
This study included six gynecologic cancer patients who underwent initial treatment, including pelvic irradiation, at the University of Tsukuba Hospital and were treated with PBT for PALN recurrence between January 2010 and December 2022. All patients were diagnosed with recurrence as lymph node enlargement greater than 10 mm in short diameter on computed tomography (CT) or positive fluorodeoxyglucose uptake on positron emission tomography (PET)-CT before treatment. Clinical information was collected retrospectively from medical records to investigate treatment history and adverse events. The patients with oligometastasis who could be treated as curative irradiation were included. We excluded the patients with an Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) >2, ileus, or severe radiation-related complications.
PBT
PBT planning was performed using CT scans with a slice interval of 2.5-5 mm in the supine position. Captured CT images were transferred to the VQA treatment planning system (Version 1.7 or 2.0, Hitachi, Tokyo, Japan). A passive scattering method was employed, and the proton beam energy was selected within the range of 155-230 MeV. In all cases, a single dose of 2 Gy relative biological effectiveness (RBE) was administered. The initial clinical target volume (CTV1) was defined as the gross tumor volume (GTV) plus a 5-mm margin and the PALN region. While the craniocaudal range of CTV1 was generally established from the L1 to L5 vertebral levels, adjustments were made to the lower boundary of the PBT field to avoid overlap with previously irradiated areas. CTV1 received a dose of 50 Gy (RBE) through two opposing anterior-posterior fields. Subsequently, the clinical target volume for boost irradiation (CTV2) was defined as GTV plus 5 mm, with an additional dose of 6-10 Gy (RBE). Dose constraints for organs at risk were assessed by overlaying the dose distribution from previous pelvic X-ray irradiation with the current PBT distribution. The cumulative dose from X-rays and PBT in overlapping slices was carefully managed. Specifically, the maximum combined dose for the intestines and cauda equina in overlapping slices was limited to 60 Gy (RBE). In slices without overlap, the maximum dose to the intestines was maintained at ≤54 Gy (RBE).
Evaluation
Overlapping irradiated fields were assessed using the 50% isodose line distance between the initial irradiated field and the PBT field. All patients were scheduled for weekly consultations during PBT treatment and follow-up visits every 1-3 months after PBT completion. Acute and late toxicities were assessed using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), Version 4.0 [8]. Treatment response was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST), Version 1.1.7 [9].
Ethics
All procedures were conducted in accordance with the Declaration of Helsinki. This retrospective study was approved by the Institutional Review Board of the University of Tsukuba Hospital (approval number: H24-108). Informed consent for treatment was obtained from all patients.
Results
The patients' background characteristics and treatments are summarized in Table 1. Of the six patients, four had cervical cancer, one had vulvar cancer, and one had endometrial cancer. Initial treatments included concurrent chemoradiotherapy (CCRT) in five patients and postoperative adjuvant radiotherapy in three patients. The upper pelvic irradiated levels were set between L4 and S1, with irradiation doses ranging from 56 to 60 Gy. The median time from initial treatment to recurrence was 18 months (range: 4-24 months) (Figure 1). Among the six patients, three patients displayed overlapping irradiated fields measuring 5-10 mm, which was evaluated using the 50% isodose line distance. The PBT doses ranged from 50 to 60 Gy (RBE). Three patients received CCRT with weekly cisplatin (Table 1; cases 2, 3, and 6).
Distance of overlapping irradiated fieldsOverlapping irradiated fields were assessed as the 50% dose distance between the initial irradiated field and proton beam therapy field.
The adverse events after PBT are shown in Table 2. Sigmoid perforation (grade 4) occurred in one patient who developed multiple peritoneal dissemination and massive ascites. The perforation was located outside the PBT field, as confirmed by CT. Two months prior to perforation, the patient underwent a colonoscopy, which revealed radiation-induced proctitis confined to the rectum. Thus, the sigmoid perforation was likely associated with dissemination rather than PBT. Rectal hemorrhage (grade 2) occurred in three patients, and hematuria (grade 3) occurred in two patients. Rectal hemorrhage was diagnosed as radiation-induced proctitis on colonoscopy and hematuria as radiation-induced cystitis on cystoscopy. Both events were attributed to the initial pelvic irradiation since the affected organs were outside the PBT field.
The prognosis of patients after PBT is shown in Table 3. The median overall survival after PBT for all six patients was 18 months (range: 9-34 months). Although all patients experienced disease progression after PBT for PALN recurrence, re-enlargement of the PALNs treated with PBT was not observed in four patients, which indicates effective local control of PALN recurrence following PBT.
Discussion
This is the first study to investigate the feasibility of PBT for PALN recurrence in patients with gynecological cancers after pelvic irradiation. It offers critical insights into advancing treatment options for this challenging clinical scenario. Re-irradiation was traditionally considered challenging due to the increased risk of radiation-associated complications [4]. However, recent advances in radiotherapeutic techniques, including PBT, have expanded treatment options for recurrence at previously irradiated sites [7].
When irradiation of a PALN recurrence after pelvic irradiation is considered, the lower line of irradiation to the PALN recurrence may overlap the upper line of pelvic irradiation, necessitating careful dose management in the overlapping field. In this study, PBT was chosen for PALN recurrence to avoid adverse events and ensure treatment completion. The unique characteristics of PBT enable a rapid dose escalation at a specific depth while sparing normal tissues [10]. Specifically, the irradiation dose decreases immediately upon entering the body, increases rapidly at the target depth, and ceases thereafter. This allows for increased dose concentration of the tumor and reduced exposure to normal organs. The dose-reduction benefits of PBT are well-documented, with reductions of approximately 32% for the small bowel and 56% for the colon compared to intensity-modulated radiotherapy (IMRT) with X-rays [11]. While PBT to a PALN minimizes unnecessary irradiation to surrounding organs, particularly the intestinal tract and bone marrow, it offers superior sparing of normal tissues compared to X-ray-based techniques. The APROVE (Adjuvant PROton therapy for cerVical and Endometrial cancer) trial, a prospective, single-center, single-arm, phase II trial, assessed the feasibility of postoperative adjuvant pelvic irradiation with PBT in patients with cervical and endometrial cancer, enrolling 25 patients [12]. The results of the study, with a median follow-up of 25.1 months, demonstrated that no patients developed gastrointestinal or urological toxicity of grade 3 or higher, indicating that the treatment was well-tolerated. In the present study, sigmoid perforation was considered associated with peritoneal dissemination since no abnormalities in the sigmoid were observed on colonoscopy immediately prior to perforation. Additionally, all patients who developed rectal hemorrhage and hematuria exhibited findings of radiation-induced proctitis on colonoscopy and radiation-induced cystitis on cystoscopy. These findings were localized within the region of X-ray therapy and outside the PBT field, suggesting that adverse events were less likely to be associated with PBT.
Pelvic irradiation is reportedly more likely to cause myelosuppression, as approximately 60% of adult hematopoietic stem cells are located within the lumbar spine and pelvis [13]. Moreover, extensive radiotherapy has been identified as a risk factor for myelosuppression [14]. In this study, two patients underwent chemotherapy after PBT, and no grade 4 hematologic toxicities were observed, indicating that PBT is unlikely to adversely affect subsequent treatments.
In this study, the local control rate was 66.7% (4/6), and the rate of severe complications (grade 3 or higher) was 33.3% (2/6). Russell et al. reported on re-irradiation using external beam radiotherapy and/or brachytherapy for patients with recurrent cervical cancer who developed recurrence within a previously irradiated pelvic lesion [15]. Among 18 patients treated with external beam radiotherapy and/or brachytherapy, the median dose of whole-pelvis external beam radiotherapy as initial treatment was 43 Gy (range: 24-54 Gy). For patients receiving external beam alone (n=7), the median dose was 62 Gy (range: 39-72 Gy), while for those treated with external beam plus brachytherapy (n=9), the median dose was 40.6 Gy (range: 9-55.2 Gy). Excluding two patients treated with brachytherapy alone, the local control rate was 50% (8/16), with follow-up ranging from 10 to 45 months. However, complications were reported in seven patients (43%), including chronic radiation proctitis (n=2), chronic radiation cystitis (n=1), aseptic necrosis of the femoral neck (n=2), small bowel obstruction requiring surgery (n=1), and rectovaginal fistula (n=1). The results from Russell et al. [15] suggest that using X-rays to deliver sufficient therapeutic doses increases the risk of adverse events. These findings highlight the need for novel radiotherapy modalities capable of delivering high-dose, targeted treatment to disease sites while minimizing adverse events. A study using stereotactic body radiotherapy (SBRT) for recurrent cervical cancer in patients previously irradiated to the pelvis reported a local control rate of 80% (68/85). Chronic toxicity occurring six weeks or more after SBRT was observed in 14 patients (16%) [16]. Additionally, a small study involving 20 patients treated with heavy ion beams, a type of particle beam therapy, reported a three-year local control rate of 61.4%, with no grade 3 or higher adverse events [17]. In the present study, all patients completed PBT as planned, and four of the six patients showed no re-enlargement of PALN. In the two patients who experienced PALN re-enlargement after PBT, the time from completion of initial treatment to recurrence was shorter (four and six months) compared to the other patients (median: 19 months; range: 11-24 months). In a study of re-irradiation using X-rays reported by Russell et al., the median interval from initial treatment to re-irradiation was 14 years (range: 1-37 years) [15]. This suggests that the interval between initial radiotherapy and recurrence may influence radiotherapy sensitivity. If sufficient time elapses following the initial treatment, PBT appears capable of delivering adequate therapeutic doses without significantly increasing the risk of adverse events. However, the effect may be due not only to PBT but also to other irradiation treatments.
This study has some limitations. First, its retrospective nature may have introduced selection bias. Second, data were collected from a single institution, and the sample size was small. Third, the follow-up duration may have been insufficient to comprehensively evaluate safety and effectiveness, as five of the six patients had already died. Further studies with larger cohorts and longer follow-up periods are necessary to confirm the feasibility of PBT for re-irradiation. Despite these limitations, however, this study provides valuable evidence supporting the feasibility of PBT for PALN recurrence.
Conclusions
PBT is a feasible treatment option for patients with PALN recurrence after pelvic irradiation. The interval between the completion of initial radiotherapy and recurrence appears to influence radiotherapy sensitivity. Thus, when sufficient time elapses after initial treatment, PBT may offer an effective and safe therapeutic approach for gynecologic cancer patients with suspected overlap of irradiated fields. Future studies with larger, multicenter cohorts and longer follow-up periods are essential to validate these findings and establish evidence-based guidelines for the use of PBT in re-irradiation settings. Future research should explore the long-term outcomes and comparative efficacy of PBT versus other advanced radiotherapy techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frequency and characteristics of isolated para-aortic lymph node recurrence in patients with uterine cervical carcinoma in Japan: a multi-institutional study Gynecol Oncol Niibe Y Kazumoto T Toita T 43543810320061667769110.1016/j.ygyno.2006.03.034 · doi ↗ · pubmed ↗
- 2The incidence of isolated para-aortic nodal metastasis in completely staged endometrial cancer patients Gynecol Oncol Chiang AJ Yu KJ Chao KC Teng NN 12212512120112119473710.1016/j.ygyno.2010.11.026 · doi ↗ · pubmed ↗
- 3Prospective assessment of the prevalence of pelvic, paraaortic and high paraaortic lymph node metastasis in endometrial cancer Gynecol Oncol Kumar S Podratz KC Bakkum-Gamez JN 384313220142412092610.1016/j.ygyno.2013.10.002PMC 4381544 · doi ↗ · pubmed ↗
- 4ESTRO/ACROP IORT recommendations for intraoperative radiation therapy in locally recurrent rectal cancer Clin Transl Radiat Oncol Calvo FA Sole CV Rutten HJ 41482420203261309110.1016/j.ctro.2020.06.007PMC 7320231 · doi ↗ · pubmed ↗
- 5A systematic review of publications on charged particle therapy for hepatocellular carcinoma Int J Clin Oncol Igaki H Mizumoto M Okumura T Hasegawa K Kokudo N Sakurai H 4234332320182887134210.1007/s 10147-017-1190-2 · doi ↗ · pubmed ↗
- 6Concurrent chemoradiotherapy using proton beams for unresectable locally advanced pancreatic cancer Radiother Oncol Hiroshima Y Fukumitsu N Saito T 374313620193101512710.1016/j.radonc.2019.03.012 · doi ↗ · pubmed ↗
- 7Proton radiotherapy for gynecologic neoplasms Acta Oncol Verma V Simone CB 2nd Wahl AO Beriwal S Mehta MP 125712655520162750071010.1080/0284186 X.2016.1205218 · doi ↗ · pubmed ↗
- 8Common Terminology Criteria for Adverse Events (CTCAE) v 4.0 12 2024 Institute NC 2009 https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_40