Inflammatory myofibroblastic tumor of the right renal pelvis: A case report
Xiaorui Zhu, Xueli Dong, Hongzhou Sheng, Renbin Deng, Xianzhong Duan

TL;DR
This case report describes a rare tumor in the kidney of a 54-year-old man, diagnosed through imaging and treated with surgery.
Contribution
The novelty lies in reporting an inflammatory myofibroblastic tumor in the renal pelvis, a rare location for this tumor type.
Findings
A mass in the right renal pelvis was identified using CT and MRI.
The patient underwent laparoscopic radical nephroureterectomy for treatment.
Abstract
Inflammatory myofibroblastic tumor(IMT) is an uncommon soft tissue neoplasm rarely reported in the urinary tract. A 54-year-old male presented to our institution with low back and abdominal pain, hematuria, and lower urinary tract symptoms for 2 months. We performed abdominal contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI), which showed a mass in the right renal pelvis-inferior calyx. Then, we performed the laparoscopic radical nephroureterectomy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
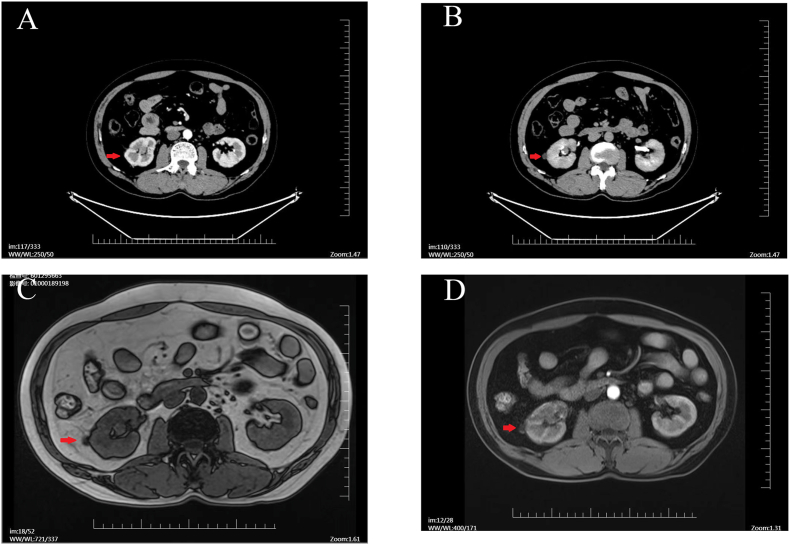 Figure 1
Figure 1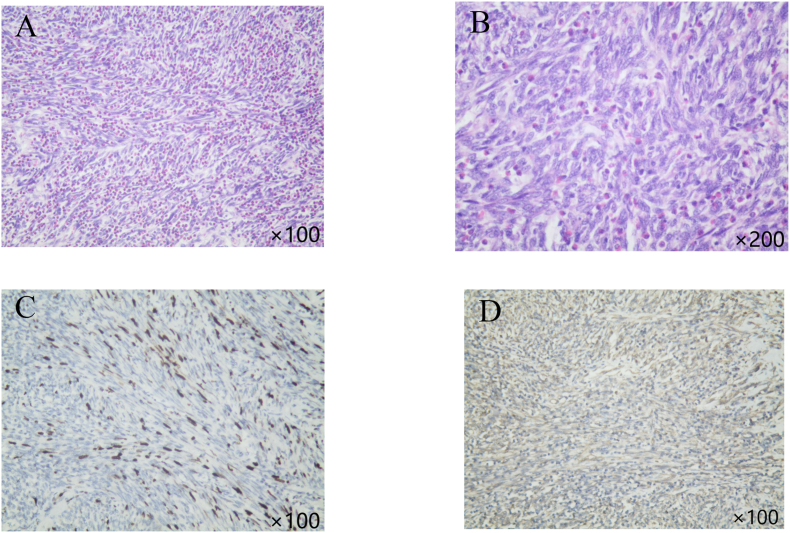 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Pancreatitis Pathology and Treatment · Case Reports on Hematomas
Introduction
1
IMT is a rare mesenchymal tumor, commonly found in the lungs and rarely in the urinary tract, especially the renal pelvis.1 Initially considered a benign inflammatory process, IMT is now recognized for its potential malignancy due to chromosomal abnormalities in the p21-23 region of chromosome 2.2 Herein, we report a case of a patient with right renal pelvis IMT who underwent laparoscopic radical nephroureterectomy.
Case report
2
In April 2023, a 54-year-old male presented to our institution with low back and abdominal pain, hematuria, and lower urinary tract symptoms for 2 months. He denied malignancy, abdominal trauma, and a history of smoking, and a routine physical examination revealed no significant abnormalities. His initial urinalysis indicated elevated leukocytes and significant occult blood, though other laboratory values were normal. To clarify the source of hematuria and pain, we performed abdominal contrast-enhanced computed tomography (CT), which showed a mass of approximately 1.1 × 1.2 × 2.2 cm in the right renal pelvis-inferior calyx, with heterogeneous enhancement in the arterial phase, slightly diminished in the venous phase, and the renal pelvis showing a filling defect in the delayed phase(Fig. 1A and B). Considering a high probability of a malignant tumor of the renal pelvis, we performed a urine cytology, and the results were negative. Magnetic resonance imaging (MRI) was then performed, and the results indicated a soft-tissue mass in the right renal pelvis-inferior calyx with irregular morphology, weak enhancement, and diffusion-limited in the diffusion-weighted imaging (DWI) (Fig. 1C and D), which was consistent with the CT diagnosis.Fig. 1Pre-operative imaging data. A–B: CT images. C–D: MRI images.Fig. 1
The patient ultimately underwent laparoscopic radical nephroureterectomy. The postoperative histopathological examination revealed a generalized distribution of spindle cells with various types of inflammatory cell infiltration including lymphocytes and plasma cells, capillary proliferation, and local necrosis (Fig. 2A and B). Immunohistochemistry was positive for smooth muscle actin (SMA), Ki-67 (20 %), CD99, and vimentin, and negative for activin receptor-like kinase (ALK), STAT6, and CD117 (Fig. 2C and D). The patient's postoperative recovery was uneventful, with no recurrence or metastasis noted. The renal function of the postoperative patient rose from 73.0 μmol/L to 148.3 μmol/L. There was no further increase in the following months.Fig. 2Immunohistochemistry. A–B: Immunohistochemistry for Ki-67. C–D: Immunohistochemistry for Vimentin.Fig. 2
Discussion and conclusion
3
The etiology and pathogenesis of IMT remain elusive at present which may be attributed to chronic inflammation, surgery, trauma, and chromosomal aberrations.1 Renal IMT lacks characteristic features in clinical manifestations and imaging exams, with approximately 38%–54 % of patients presenting with low back pain or abdominal pain and 28%–29 % presenting with gross or microscopic hematuria,3 due to the presence of extensive fibrous tissue components in the solid mass of IMT, it shows mild enhancement in the arterial phase on enhanced CT scan and low signal intensity in the T2 phase on MRI examination.4 Patients are therefore difficult to discriminate preoperatively from renal pelvic malignancies, a fact that often leads to over-surgical treatment. Although there is no clear standard for the treatment of renal IMT, radical surgical resection is primarily performed.5 In our case, the middle-aged male displayed symptoms and imaging akin to renal pelvis cancer. Following a laparoscopic radical nephroureterectomy, he experienced no severe complications or signs of recurrence, suggesting that surgery is an effective IMT treatment. However, its long-term prognosis requires further study.
CRediT authorship contribution statement
Xiaorui Zhu: Writing – original draft, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Xueli Dong: Validation, Software, Project administration, Methodology. Hongzhou Sheng: Validation, Supervision, Methodology, Investigation, Conceptualization. Renbin Deng: Writing – review & editing, Software. Xianzhong Duan: Writing – review & editing, Supervision, Project administration, Investigation.
Consent to participate
Informed written consent was obtained from patients to participate in this study.
Ethics approval
Ethics approval was granted from The Second People's Hospital of Baoshan.
Consent for publication
All authors have agreed to publish this paper.
Funding
This study is funded by the 10.13039/501100007846Yunnan Provincial Department of Education Science Research Fund Project (grant no. 2022J1574).
Declaration of competing interest
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang G.H.Guo X.Y.Liang G.Z.Wang Q.Kidney inflammatory myofibroblastic tumor masquerading as metastatic malignancy: a case report and literature review World J Clin Cases 7242019 Dec 26 20194366437610.12998/wjcc.v 7.i 24.4366 PMC 694033631911920 · doi ↗ · pubmed ↗
- 2Coffin C.M.Patel A.Perkins S.Elenitoba-Johnson K.S.Perlman E.Griffin C.A.ALK 1 and p 80 expression and chromosomal rearrangements involving 2p 23 in inflammatory myofibroblastic tumor Mod Pathol 1462001 Jun 200156957610.1038/modpathol.388035211406658 · doi ↗ · pubmed ↗
- 3Pothadiyil A.J.Bhat S.Paul F.Mampatta J.Srinivas M.Inflammatory myofibroblastic tumor of the kidney: a rare renal tumor J Clin Diagn Res 10112016 Nov 2016 D 17D 1810.7860/JCDR/2016/22465.8856 PMC 519833728050384 · doi ↗ · pubmed ↗
- 4Han Y.Yang G.Du J.Tan Y.Zhang H.The MRI features of renal inflammatory pseudotumor: a case report and literature review Medicine (Baltim)102122023 Mar 24e 3328710.1097/MD.0000000000033287 PMC 1003602536961141 · doi ↗ · pubmed ↗
- 5Ariafar A.Ahmed F.Khorshidi A.Torabi-Nezhad S.Hosseini S.H.Inflammatory myofibroblastic tumor of the right kidney mimicking a locally advanced renal carcinoma: a case report J Kidney Cancer VHL 942022 2022141810.15586/jkcvhl.v 9i 4.238PMC 976041536578280 · doi ↗ · pubmed ↗