Big data analysis of influenza vaccination and liver cancer risk in hypertensive patients: insights from a nationwide population-based cohort study
Chun-Chih Chiu, Wen-Rui Hao, Kuan-Jie Lin, Chun-Chao Chen, Tsung-Yeh Yang, Yu-Ann Fang, Tsung-Lin Yang, Yu-Hsin Lai, Ming-Yao Chen, Min-Huei Hsu, Cheng-Hsin Lin, Hsin Hsiu, Huan-Yuan Chen, Tzu-Hurng Cheng, Nai-Hsuan Chen, Ju-Chi Liu

TL;DR
A nationwide study found that getting the flu vaccine is linked to a lower risk of liver cancer in people with high blood pressure.
Contribution
This study is the first to show a dose-dependent protective effect of influenza vaccination against liver cancer in hypertensive patients.
Findings
Flu vaccination was associated with a 44% lower risk of liver cancer in hypertensive patients.
The protective effect increased with more vaccination doses.
The association remained consistent across age, sex, and comorbidities.
Abstract
previous studies have indicated that influenza vaccination may be associated with reduced risks of certain types of cancer. However, the protective effect of influenza vaccination against primary liver cancer in individuals with hypertension remains unclear. In this cohort study, 37,022 patients over 55 years of age who received a diagnosis of hypertension at any time between January 1, 2001, and December 31, 2012, were enrolled from the National Health Insurance Research Database. The patients were divided into a vaccinated and an unvaccinated group. Categorical and continuous variables were analyzed using the chi-square test and t test, respectively, and the correlation between influenza vaccination and liver cancer in patients with hypertension was analyzed using time-varying COX model. Propensity score method was performed to reduce selection bias. Compared with the unvaccinated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
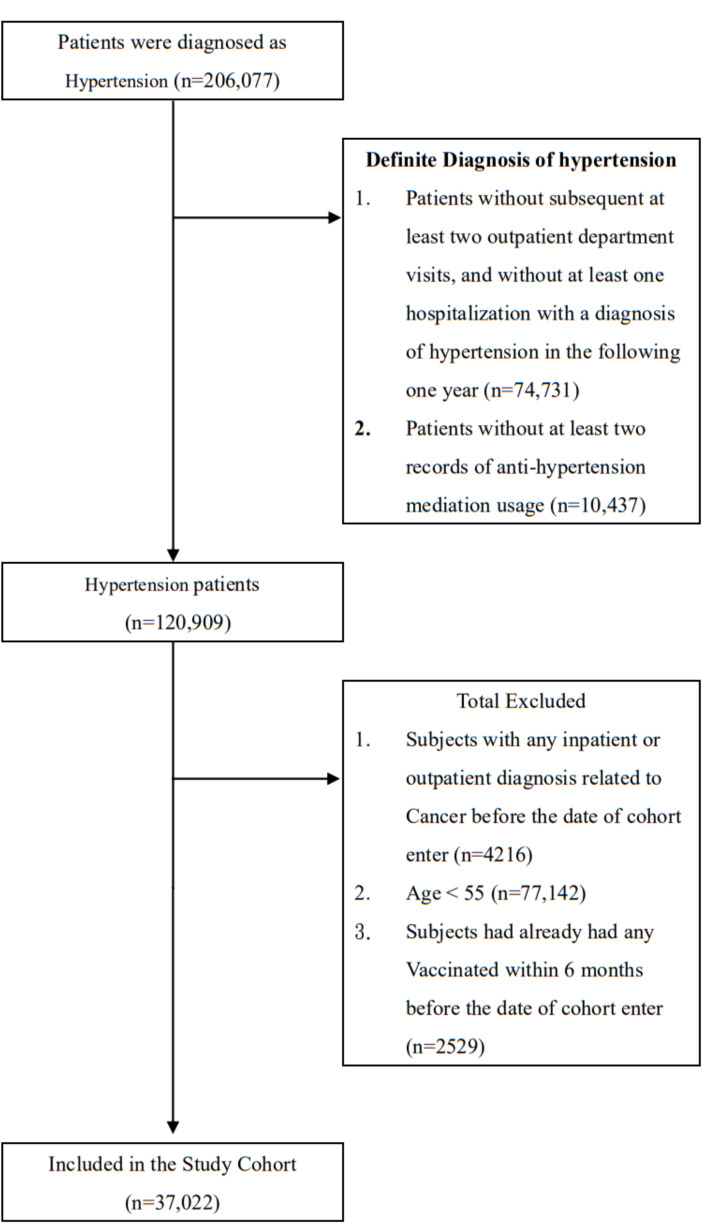 Figure 1
Figure 1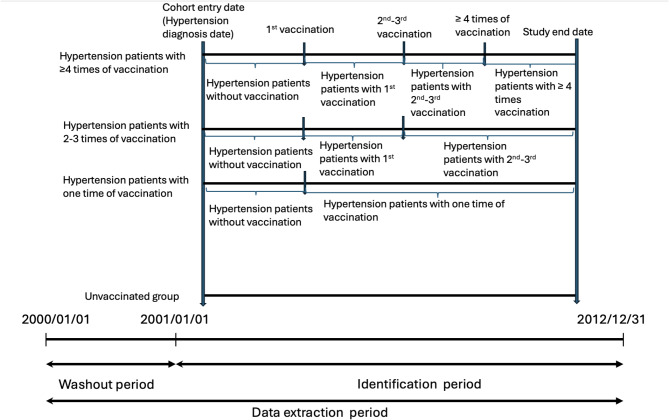 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfluenza Virus Research Studies · interferon and immune responses · Cytokine Signaling Pathways and Interactions
Background
Hypertension is a chronic disease that is serious and highly prevalent, especially given aging populations worldwide. More than 1 billion people worldwide have been estimated to have hypertension [1, 2]. In Taiwan, hypertension has a prevalence of 24.1% [3]. Elevated blood pressure is a risk factor for several conditions, such as cardiovascular disease, chronic kidney disease, and stroke [4]. Hypertension is also associated with an increased risk of cancer [5, 6].
Primary liver cancer is a common cancer in the world, especially in Taiwan [7]. According to the Health Promotion Administration, the age-standardized incidence rate of liver cancer in Taiwan was 26.14 per 100,000 individuals in 2020, which is significantly above than the global average (9.3 per 100,000 individuals) [8, 9]. Liver cancer is the second leading cause of cancer-related death in Taiwan, with a standardized mortality rate of 17.9 per 100,000 individuals [10]. According to previous studies, many risk factors have been associated with the incidence of liver cancer, such as infection with the hepatitis virus, exposure to aflatoxins, cigarette consumption, drinking alcohol, and diabetes [11–13]. Elevated blood pressure has also been connected to an elevated risk (with a relative risk of 1.55) and grim outlook of liver cancer [6, 14]. This association may be linked to chronic inflammation, cellular apoptosis, and collagen enzyme dysregulation [6, 15–18].
Influenza is a highly contagious seasonal epidemic infection that causes an abrupt onset of high fever, myalgia, and respiratory symptoms [19]. This seasonal infection is responsible for the death of more than 290,000 individuals each year worldwide [19, 20]. It increases hospitalization, morbidity, and mortality rates and places an additional economic burden on patients, especially for senior citizens and individuals with chronic medical conditions [19, 20]. Past statistics also disclosed that virus infection is positive associated with cancer development [21]. Therefore, multiple studies have attempted to clarify the relationship between influenza and cancer and seek strategies to prevent infection.
According to previous studies, influenza vaccination reduces infection, hospitalization, and illness severity [22, 23]. Furthermore, vaccination could reduce the inflammation status and oxidative stress from virus infection [24]. These pathogeneses may also exist in the mechanism of the liver cancer formation [25]. While the exact mechanisms remain unknown, this study focuses on impact of influenza vaccine on the occurrence of liver cancers among a Taiwanese population with hypertension by applying the data from Taiwan’s National Health Insurance Research Database (NHIRD).
Method
Established in 1995, the National Health Insurance program provides comprehensive healthcare to over 98% of the Taiwanese citizens [26]. This study was conducted using data obtained from the NHIRD (2001–2012). To protect personal privacy, all information obtained from the NHIRD was processed through delinking and deidentifying procedures. During data collection, an agreement was signed to ensure the privacy of the patients’ and care providers’ information. The approval for this study was obtained from the Joint Institutional Review Board of Taipei Medical University (approval no. N201804043).
Patient selection and definition of the primary endpoint
The study cohort included all patients who received a diagnosis of hypertension in accordance with the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM, codes 401.X and 402.X) over a period of 12 years from January 1, 2001, to December 31, 2012. Patients without at least two subsequent outpatient department visits and one instance of hospitalization for hypertension in the following year or without at least two records of antihypertension medication use were excluded due to the uncertainty of hypertension diagnosis (Fig. 1). To exclude patients who had cancer before the selection procedure, this study implemented a 1-year (2000) washout period. This study excluded patients under 55 years. As stipulated by the Taiwanese government, vaccination is free for individuals older than 65 years or high-risk individuals aged 50–65 years, specifically individuals who have cardiovascular disease, renal disease, compromised immunity, a body mass index of 30 or greater, or type 2 diabetes mellitus [27]. Besides, in order to eliminate the interference effects caused by recent vaccinations, patients who received influenza vaccination within half a year before the enrollment date were excluded. In this study, we used ICD-9-CM code V048 and vaccine drug codes to examine the vaccination history of our participants. We also set the primary endpoint as the occurrence of primary liver cancer (ICD-9-CM code 155.X) in patients with hypertension during the follow-up period. All patients were followed up until they received a new diagnosis of liver cancer, withdrew from the National Health Insurance program, were lost to follow-up, or died or until December 31, 2012.
Fig. 1. Data selection process
Potential confounders
Possible confounding factors, such as sociodemographic characteristics (age, sex, urbanization level, and monthly income), comorbidities (Charlson Comorbidity Index [CCI], diabetes mellitus [ICD-9-CM, codes 250.X], dyslipidemia [ICD-9-CM, codes 272.X], heart failure [ICD-9-CM, codes 428], acute myocardial infarction [ICD-9-CM, codes 410], atrial fibrillation [ICD-9-CM, codes 427.31], ischemic heart disease [ICD-9-CM, codes 414.9], angina [ICD-9-CM, codes 413], peripheral vascular disease [ICD-9-CM, codes 443.9], cerebrovascular diseases [ICD-9-CM, codes 430–438], renal failure [ICD-9-CM, codes 585.X], hepatitis B virus [ICD-9-CM, codes 070.2X, 070.3X], hepatitis C virus [ICD-9-CM, codes 070.41, 070.44, 070.51, 070.54], metabolic dysfunction-associated fatty liver disease [MAFLD] [ICD-9-CM, codes 571.8, 571.9], cirrhosis [ICD-9-CM, codes 571]), antihypertension medications (antihypertensive drugs [WHO-ATC, codes C02, C02A, C02B, C02C, C02D, C02K, C02L, and C02N], diuretics [WHO-ATC, codes C03], beta blockers [WHO-ATC, codes C07], calcium channel blockers [WHO-ATC, codes C08], and renin–angiotensin–aldosterone system inhibitors [RAASIs] [WHO-ATC, codes C09]), and other medication use (statins [WHO-ATC, codes C10AA], metformin [WHO-ATC, codes A10BA02], and aspirin [WHO-ATC, codes B01AC06 and N02BA01]), were analyzed for each patient included in the study. The reason we select statins, metformin, and aspirin as covariates is that some previous studies have indicated they may have a protective effect against the occurrence of cancer [27–29]. Besides, we categorized the concurrent medications based on the number of the prescription days (< 28 days, 28–365 days, or > 365 days) during the observation period.
Statistical analysis
To minimize selection bias and evaluate the effects of vaccination, we first estimated the baseline propensity scores (PS) using a logistic regression model to predict the probability of receiving influenza vaccine in each patient. In further time-varying logistic regression model analysis, PS adjusting was used to account for covariates between the vaccinated and unvaccinated groups [30, 31]. Categorical and continuous variables were analyzed using the chi-square test and t test, respectively. Time-varying COX model was used to evaluate the hazard ratios (HRs) and 95% confidence intervals (CIs) of liver cancer between vaccinated and unvaccinated patients with hypertension. Subsequently, we categorized the hypertension patients into four groups according to their vaccination status (unvaccinated patients, patients who received one vaccine dose, patients who received two or three vaccine doses, and patients who received four or more vaccine doses) to calculate the dose–response effect. The effect of changing vaccination status in each patient was considered. Therefore, a time-varying COX model was used to evaluate the hazard ratios (HRs) and 95% confidence intervals (CIs) of liver cancer between vaccinated and unvaccinated patients with hypertension. Among patients who received vaccines two to three times, the time period before the second vaccination and after the first vaccine would be classified into patients with first-time vaccination. Similarly, among patients who received more than four times of vaccination, the time period would be classified into patients with one time of vaccination and patients with two to three times of vaccination before the second time of vaccination and before the fourth time of vaccination (Fig. 2). Data were then stratified by potential confounding factors, namely age, sex, comorbidities, and medication use. Additionally, we divided the patients into two groups based on the follow-up period: over 10 years and under 10 years. Ultimately, sensitivity analysis was conducted to explore the distinctions and similarities between influenza vaccination and the occurrence of liver cancer in patients with hypertension. All statistical analyses were conducted using IBM SPSS Statistics version 22.0 (IBM, Armonk, NY, USA) and SAS version 9.4 (SAS Institute, Cary, NC, USA). A p value less than 0.05 indicated statistical significance.
Fig. 2. Time-varying analysis in unvaccinated patients and patients who received 1, 2–3 and more than 4 times of vaccination
Results
Baseline characteristics
From 2001 to 2012, there were a total of 206,077 patients diagnosed with hypertension. Some patients were excluded due to the uncertainty of the hypertension diagnosis (n = 85,168), diagnosis of neoplasm (ICD-9-CM, codes 140–239) before the selection procedure (n = 4,216), being under 55 years (n = 77,142) and receiving influenza vaccination within half a year before the enrollment date (n = 2,529). Finally, there were 37,022 patients included in our study. Among the 37,022 patients with hypertension enrolled in this cohort, 15,697 were vaccinated (42.4%) and 21,325 were unvaccinated (57.6%). The Statistics Power of the study was > 0.999. The two groups significantly differed in terms of age and sex distribution, medication history, and level of urbanization (Table 1). Dyslipidemia, heart failure, acute myocardial infarction, ischemic heart disease, angina, peripheral vascular disease, cerebrovascular diseases, renal failure, hepatitis C virus and cirrhosis was more common among vaccinated than unvaccinated patients (p < .001). Comorbidity-associated medications, such as statin, metformin, and aspirin, were used at a lower rate and duration in the unvaccinated than vaccinated group (Table 1).
Table 1. Attributes of the Enrolled PopulationAll patients(n = 37022)Unvaccination(n = 21325)Vaccination(n = 15697) P ^a^
n % n % n %Age,* years (Mean ± SD)*66.37 ± 8.0864.04 ± 8.0569.52 ± 6.99< 0.00155–6418,51150.0013,90765.21460429.33< 0.00165–7412,61834.08488422.90773449.27≥ 75589315.92253411.88335921.40 Sex Female18,37349.6310,37848.67799550.93< 0.001 Charlson Comorbidity Index 016,84345.59995146.66689243.91< 0.0011988426.70562226.36426227.152569515.38321315.07248215.81≥ 3460012.43253911.91206113.13 Comorbidities Diabetes790421.35454221.30336221.420.782Hyperlipidemia28,89578.0516,48777.3112,40879.05< 0.001HF629817.01408819.17221014.08< 0.001AMI7081.914542.132541.62< 0.001AF554514.98328015.38226514.430.011Ischemic heart disease14,83140.06907042.53576136.70< 0.001Angina501113.54305414.32195712.47< 0.001Peripheral vascular disease434311.73272512.78161810.31< 0.001Cerebrovascular diseases12,18032.90593327.82624739.80< 0.001Renal failure528414.27341816.03186611.89< 0.001Hepatitis B virus6901.864121.932781.770.258Hepatitis C virus14493.917493.517004.46< 0.001MAFLD736119.88415419.48320720.430.023Cirrhosis15714.248473.977244.610.003 Anti-hypertension medications Beta blocking agents19,04351.4410,21747.91882656.23< 0.001Calcium channel blockers25,89169.9314,10566.1411,78675.08< 0.001Diuretics18,45049.84931843.70913258.18< 0.001RAASI22,17859.9011,89655.7810,28265.50< 0.001Other antihypertensive drugs715419.32329115.43386324.61< 0.001 Co-drugs Statin drugs< 28 days27,28473.7016,08575.4311,19971.34< 0.00128–365 days612416.54347216.28265216.89>365 days36149.7617688.29184611.76Metformin drug< 28 days29,67480.1517,30081.1312,37478.83< 0.00128–365 days27977.5517248.0810736.84>365 days455112.29230110.79225014.33Aspirin drug< 28 days21,74558.7413,76564.55798050.84< 0.00128–365 days845822.85451121.15394725.14>365 days681918.42304914.30377024.02 Level of Urbanization Urban25,03067.6115,42172.31960961.22< 0.001Suburban799221.59414619.44384624.50Rural400010.8017588.24224214.28 Monthly income (NT$) 0432711.69215010.08217713.87< 0.0011-1920011,47731.00607828.50539934.4019,200–25,00011,83231.96606628.45576636.73≥25,001938625.35703132.97235515.00^a^ Comparison between Unvaccination and VaccinationHF, heart failure, AMI, acute myocardial infarction, AF, atrial fibrillation, MAFLD, metabolic dysfunction-associated fatty liver disease, RAASI, renin-angiotensin-aldosterone system inhibitor
HRs of liver cancer in the vaccinated and unvaccinated groups
Table 2 demonstrates the incidences of liver cancer in patients with hypertension as distinguished by vaccination status. After potential confounders were adjusted for, the results indicated that the incidence of liver cancer was notably reduced in the vaccinated group compared to the unvaccinated group (Incidence rate of unvaccinated = 345.7, Incidence rate of vaccinated = 179.1; HR = 0.56, 95% CI = 0.46–0.64; p < .001). The protective effect was consistent across different age and sex groups, the HR was 0.53 in women (95% CI = 0.39–0.68; p < .001) and 0.58 in men (95% CI = 0.44–0.74; p < .001).
Table 2. Risk of Liver Cancer among Unvaccinated and Vaccinated in Study CohortAll patients(N = 37022)Unvaccinated(Total follow-up 96626.9 person-years)Vaccinated(Total follow-up 94366.2 person-years)Adjusted HR†(95% C.I.)No. ofPatientsWith CancerIncidence Rate(per 10^5^ person-years)(95% C.I.)No. ofPatientsWith CancerIncidence Rate(per 10^5^ person-years)(95% C.I.) Whole cohort liver cancer334345.7(308.6,382.7)169179.1(152.1,206.1)0.56(0.46, 0.64)Age, 55-64*^a^liver cancer196314.8(270.8,358.9)38125.0(85.3,164.8)0.50(0.34, 0.69)Age, 65-74*^b^liver cancer94401.2(320.1,482.3)90196.0(155.5,236.5)0.55(0.40, 0.72)Age, ≥ 75*^c^liver cancer44402.1(283.3,521.0)41227.0(157.5,296.4)0.57(0.39, 0.82)** Female ^d^ liver cancer136279.1(232.2,326.0)70143.3(109.7,176.8)0.53(0.39, 0.68)*** Male ^e^ liver cancer198413.4(355.8,470.9)99217.6(174.7,260.4)0.58(0.44, 0.74)***^a^Total follow-up 62254.4 person-year for unvaccinated and 30393.7 for Vaccinated^b^Total follow-up 23430.8 person-year for unvaccinated and 45908.6 for Vaccinated^c^Total follow-up 10941.7 person-year for unvaccinated and 18063.9 for Vaccinated^d^Total follow-up 48727.6 person-year for unvaccinated and 48864.1 for Vaccinated^e^Total follow-up 47899.3 person-year for unvaccinated and 45502.1 for VaccinatedC.I.: confidence interval *: P < .05 **: P < .01 *: P < .001HR: hazard ratio†**Main model is adjusted for Age, Sex, CCI Index, Diabetes, Hyperlipidemia, HF, AMI, AF, Ischemic heart disease, Angina, Peripheral vascular disease, Cerebrovascular diseases, Renal failure, Hepatitis B virus, Hepatitis C virus, Cirrhosis, Beta blocking agents, Calcium channel blockers, Diuretics, RAASI, Other antihypertensive drugs, Statin, Metformin, Aspirin, level of urbanization, monthly income in propensity score
Sensitivity analysis of the relationship between the number of vaccine doses and the risk of liver cancer
As shown in Table 3, sensitivity analysis was conducted with covariate adjustments, and the vaccinated group was stratified by the total number of vaccine doses. The result revealed not only the decreased HR of liver cancer in different groups after vaccination, but also the dose-dependent protective effects. When more than two vaccine doses were administered, the risk of liver cancer significantly decreased (Incidence Rate = 214.8, adjusted HR = 0.60, 95% CI = 0.51–0.78; Incidence Rate = 173.6, adjusted HR = 0.48, 95% CI = 0.38–0.65; and Incidence Rate = 128.1, adjusted HR = 0.39, 95% CI = 0.30–0.51 for one dose, two or three doses, and four or more doses, respectively).This protective effect was also observed in individuals with comorbidities, including those with a high CCI index, diabetes, and dyslipidemia. Table 4 demonstrated the risk of liver cancer among unvaccinated and vaccinated in study cohort stratified into 10-year follow-up periods.
Table 3. Sensitivity analysis of adjusted HRs of vaccination in risk reduction of Liver CancerUnvaccinatedVaccinatedP for Trend12–3≥ 4Adjusted HR(95%C.I.)Adjusted HR(95%C.I.)Adjusted HR(95%C.I.)Adjusted HR(95%C.I.) Follow-up duration
(person-years) 96626.935842.937444.821078.5 Number of Events 334776527 Incidence Rate
(per 10 ^5^ person-years) 345.7214.8173.6128.1 Main model† 1.000.60(0.51, 0.78)**0.48(0.38, 0.65)0.39(0.30, 0.51)< 0.001 Main model† + MAFLD 1.000.59(0.50, 0.77)0.47(0.37, 0.64)0.38(0.30, 0.50)< 0.001Age, years55–641.000.43(0.29, 0.75)*0.42(0.28, 0.70)0.49(0.29, 0.98)*0.08665–741.000.81(0.55, 1.13)0.45(0.34, 0.67)0.31(0.24, 0.45)< 0.001≥ 751.000.52(0.29, 0.99)*0.55(0.33, 0.94)*0.41(0.22, 0.71)< 0.001SexFemale1.000.60(0.40, 0.88)*0.45(0.32, 0.64)0.35(0.26, 0.52)< 0.001Male1.000.61(0.41, 0.87)*0.52(0.39, 0.73)0.44(0.33, 0.61)< 0.001CCI Index^+^01.000.42(0.26, 0.86)*0.59(0.40, 0.90)*0.37(0.27, 0.60)0.03411.000.75(0.45, 1.28)0.32(0.19, 0.59)0.41(0.30, 0.69)< 0.00121.000.67(0.42, 1.24)0.52(0.31, 0.91)0.48(0.33, 0.81)< 0.001≥ 31.000.68(0.43, 1.26)0.44(0.24, 0.79)0.27(0.20, 0.49)< 0.001DiabetesNo1.000.58(0.42, 0.84)0.43(0.32, 0.69)0.40(0.30, 0.54)< 0.001Yes1.000.64(0.35, 1.13)0.60(0.45, 1.01)0.37(0.26, 0.64)< 0.001HyperlipidemiaNo1.000.55(0.41, 0.80)*0.50(0.38, 0.66)0.40(0.30, 0.53)< 0.001Yes1.000.86(0.47, 1.51)0.42(0.23, 0.85)0.35(0.25, 0.60)< 0.001Hepatitis B virusNo1.000.63(0.49, 0.87)**0.47(0.37, 0.64)0.40(0.32, 0.53)< 0.001Yes1.000.54(0.21, 0.96)*-Hepatitis C virusNo1.000.63(0.51, 0.89)0.45(0.36, 0.61)0.40(0.30, 0.51)< 0.001Yes1.000.50(0.23, 1.96)0.47(0.18, 2.14)0.621CirrhosisNo1.000.65(0.52, 0.90)*0.46(0.37, 0.62)0.39(0.30, 0.51)< 0.001Yes1.000.46(0.20, 1.77)0.44(0.25, 2.06)0.596Other antihypertensive drugsNo (< 28 days)1.000.60(0.45, 0.80)*0.42(0.32, 0.58)0.38(0.29, 0.52)< 0.001Yes (≥ 28 days)1.000.68(0.37, 1.53)0.87(0.50, 1.61)0.41(0.30, 0.55)0.095DiureticsNo (< 28 days)1.000.61(0.46, 0.92)*0.40(0.30, 0.58)0.29(0.20, 0.45)< 0.001Yes (≥ 28 days)1.000.60(0.44, 0.96)*0.59(0.42, 0.88)0.46(0.36, 0.67)< 0.001Beta blocking agentsNo (< 28 days)1.000.62(0.42, 0.96)*0.48(0.32, 0.71)0.32(0.23, 0.46)< 0.001Yes (≥ 28 days)1.000.59(0.41, 0.94)*0.48(0.32, 0.70)0.43(0.32, 0.65)< 0.001Calcium channel blockersNo (< 28 days)1.000.50(0.31, 0.85)*0.40(0.24, 0.64)0.36(0.28, 0.53)< 0.001Yes (≥ 28 days)1.000.68(0.50, 1.02)0.55(0.39, 0.76)0.40(0.31, 0.56)< 0.001RAASINo (< 28 days)1.000.59(0.40, 0.90)*0.50(0.35, 0.74)0.39(0.29, 0.52)< 0.001Yes (≥ 28 days)1.000.61(0.41, 0.92)*0.47(0.32, 0.70)0.40(0.30, 0.54)< 0.001Statin drugs<28 days1.000.66(0.49, 0.91)*0.45(0.34, 0.68)0.39(0.28, 0.54)< 0.00128–365 days1.000.35(0.19, 1.07)0.34(0.16, 0.83)*0.30(0.18, 0.66)< 0.001>365 days1.000.62(0.24, 4.23)1.14(0.41, 3.97)0.41(0.08, 1.90)0.415Metformin drug< 28 days1.000.65(0.49, 0.90)*0.43(0.34, 0.59)0.39(0.30, 0.54)< 0.00128–365 days1.000.45(0.24, 1.26)0.44(0.25, 0.63)**0.041>365 days1.000.66(0.45, 1.81)0.91(0.60, 1.83)0.54(0.42, 0.76)*0.201Aspirin drug< 28 days1.000.67(0.50, 0.94)*0.43(0.33, 0.64)0.33(0.23, 0.48)< 0.00128–365 days1.000.49(0.23, 0.99)0.40(0.25, 0.72)0.39(0.26, 0.57)< 0.001>365 days1.000.48(0.15, 1.36)0.82(0.49, 1.67)0.57(0.42, 1.23)0.232C.I.: confidence interval *: P < .05 **: P < .01 *: P < .001HR: hazard ratio†**Main model is adjusted for Age, Sex, CCI Index, Diabetes, Hyperlipidemia, HF, AMI, AF, Ischemic heart disease, Angina, Peripheral vascular disease, Cerebrovascular diseases, Renal failure, Hepatitis B virus, Hepatitis C virus, Cirrhosis, Beta blocking agents, Calcium channel blockers, Diuretics, RAASI, Other antihypertensive drugs, Statin, Metformin, Aspirin, level of urbanization, monthly income in propensity scoreMAFLD, Metabolic Dysfunction-Associated Fatty Liver Disease
Table 4. Risk of Liver Cancer among Unvaccinated and Vaccinated in Study Cohort stratified into 10-year follow-up periodsAll patients< 10 years> 10 yearsfollow-upCancerfollow-upCancerfollow-upCancerUnvaccinated96626.933466462.632030164.314Vaccinated94366.216972288.815822077.411135842.97723476.07612366.912–337444.86527734.2559710.610**≥** 421078.52721078.527--Adjusted HR10.56(0.46, 0.64)***0.45(0.35, 0.73)***1.02(0.68, 1.81)Adjusted HR20.60(0.51, 0.78)**0.67(0.53, 0.94)*0.17(0.04, 1.36)Adjusted HR30.48(0.38, 0.65)***0.41(0.29, 0.57)***2.01(0.90, 5.26)Adjusted HR40.39(0.30, 0.51)0.26(0.17, 0.51)-C.I.: confidence interval *: P < .05 **: P < .01 *: P < .001HR: hazard ratio†**Main model is adjusted for Age, Sex, CCI Index, Diabetes, Hyperlipidemia, HF, AMI, AF, Ischemic heart disease, Angina, Peripheral vascular disease, Cerebrovascular diseases, Renal failure, Hepatitis B virus, Hepatitis C virus, Cirrhosis, Beta blocking agents, Calcium channel blockers, Diuretics, RAASI, Other antihypertensive drugs, Statin, Metformin, Aspirin, level of urbanization, monthly income in propensity score
Discussion
Major findings
The key discoveries of this cohort study based on the population are as follows. First, patients with hypertension who received influenza vaccine had a low incidence of liver cancer. Second, the larger the number of vaccine doses administered was, the greater the reduction in the risk of liver cancer was.
Mechanism of liver cancer development in patients with hypertension
According to previous studies, patients with hypertension have an increased risk of liver cancer [6]. Several candidate mechanisms underlying the association between hypertension and liver cancer have been proposed. One of these mechanisms is the renin–angiotensin–aldosterone system (RAAS), which is a crucial vasoactive factor that regulates blood pressure. This system exists in both the circulatory system and local tissues, including the heart, liver, and kidneys [18, 32]. RAAS dysregulation results in not only hypertension but also proinflammatory and profibrotic sequelae, with the production of an intermediate product. These sequelae increase the risk of liver fibrosis and hepatocarcinogenesis [32]. Furthermore, patients with hypertension exhibit increased vascular endothelial growth factor (VEGF) expression. VEGF contributes to cancer progression by affecting blood vessel permeability, proliferation, and endothelial cell growth [6, 33]. Another mechanism linking hypertension to liver cancer is metabolic syndrome, which, similar to hypertension, stimulates the production of reactive oxygen species (ROS) and results in inflammation. These sequelae may influence the regulation of the extracellular matrix (ECM) and tissue repair, induce a malignant phenotype, and trigger tumor development [6, 34, 35]. Matrix metalloproteinases (MMPs), a group of enzymes that degrade collagen in the ECM, also serve as a link between hypertension and cancer. Recent studies have indicated a correlation between MMPs and hypertension through insulin resistance and mechanical stress [34, 36]. The stiffening and degradation of the ECM and the regulation of inflammation by MMPs play a role in the development of cancer [37].
Relationship between the risk of liver cancer and influenza vaccination
The primary purpose of vaccination is to provide protection against infection or severe illness. Additionally, it is be pointed that human papillomavirus vaccine and hepatitis B vaccine also prevent people from cancer. Influenza vaccination has also been reported to be associated with a lower risk of lung cancer [38]. In patients with influenza, the number of inflammatory cytokines increases in their circulatory system, resulting in cellular necrosis and oncogenic signaling cascades [18, 39]. This process also induces inflammation and ROS production, which not only cause cellular damage but also affect the ECM, as is the case in hypertension [38, 40]. Consequently, cell proliferation, polarity, differentiation, migration, and adhesion are all affected in the ECM [6]. Inappropriate remodeling of the ECM may exacerbate the risk of cancer [41]. In addition, MMPs play a role in immune responses to infection. However, MMP overactivation following infection may increase the host’s vulnerability to pathogen attack, tissue damage, and proto-oncogene activation [6, 42]. Hence, vaccination against influenza may protect patients from infection and liver cancer.
Effect of influenza vaccination in different subgroups
Overall, our findings suggested that influenza vaccination has a stronger protective effect in women than in men. According to a previous study, women have a lower risk of liver cancer than men presumably because estrogen reduces the concentration of inflammatory cytokines [43]. Both estrogen and influenza vaccine may have a synergic effect that increases the level of protection. Patients who take blood pressure medication over a short period have a low risk of liver cancer because their hypertension may be less severe than patients who do not take such medication. Thus, vaccination can effectively control inflammation and the production of ROS and MMPs. However, the dose-dependent effect of influenza vaccine seems to be more pronounced in individuals aged above 65, presumably because the immune system tends to weaken with age, making it less responsive to vaccines [44, 45]. Consequently, additional vaccine doses may be required to stimulate memory cell function. As a result, implementing a consistent and well-planned vaccination policy is imperative for elderly individuals with hypertension.
Limitations
This study has some limitations. First, we identified patients with hypertension on the basis of ICD-9-CM codes, which may have resulted in some misclassification. Thus, we incorporated drug, outpatient, and hospitalization data for greater accuracy. Second, the NHIRD does not report on personal behavioral data (e.g., cigarette and alcohol use), blood pressure data, or biochemical data. We were also unable to differentiate between different types of liver cancer, such as hepatocellular carcinoma and cholangiocarcinoma, to evaluate the effect of vaccination on each category. However, we discovered that vaccination against influenza was associated with a reduced risk of liver cancer. We also performed PS adjusting to minimize bias due to potential confounders. Third, because of vaccination policies in Taiwan, we only enrolled patients aged above 55. Therefore, our experimental results may not be generalizable to all age groups. Fourth, this was not a prospective randomized blinded study and thus could not provide causal evidence. Fifth, the chosen cohort for this study spans from 2001 to 2012. It is necessary to analyze more recent data in future studies to confirm the findings of the current research. In addition, there were limited patients with a follow-up period more than 10 years, future study is warranted for validating the long-term effect of vaccine.
Conclusion
In hypertensive patients, getting vaccinated against influenza is linked to a lowered risk of liver cancer. However, additional research is required to investigate the mechanism underlying this association.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Hypertension 25 August 2021 [Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension
- 2Connaughton M, Dabagh M. Association of Hypertension and Organ-Specific Cancer: a Meta-analysis. Healthc (Basel). 2022;10(6).10.3390/healthcare 10061074 PMC 922290435742125 · doi ↗ · pubmed ↗
- 3Health Promotion Administration. 2020 Annual Cancer Incidence Rate Health Promotion Administration 01 February 2023 [Available from: https://reurl.cc/9V Gg Aj
- 4Ministry of Health and Welfare. 2021 Annual Report on Causes of Death 19 August 2022 [Available from: https://reurl.cc/E Grqj R
- 5World Health Organization. Influenza (Seasonal) 12 January 2023 [Available from: https://reurl.cc/e X Oz RQ
- 6Dhanasekaran R, Bandoh S, Roberts LR. Molecular pathogenesis of hepatocellular carcinoma and impact of therapeutic advances. F 1000 Res. 2016;5:F 1000 Faculty Rev-879.10.12688/f 1000 research.6946.1PMC 487099227239288 · doi ↗ · pubmed ↗
- 7Jiang W, Hu J-W, He X-R, Jin W-L, He X-Y. Statins: a repurposed drug to fight cancer. J Experimental Clin Cancer Res. 2021;40(1).10.1186/s 13046-021-02041-2PMC 830626234303383 · doi ↗ · pubmed ↗
- 8Laronha H, Caldeira J. Structure and function of human matrix metalloproteinases. Cells. 2020;9(5).10.3390/cells 9051076 PMC 729039232357580 · doi ↗ · pubmed ↗