Age and sources of information variations and similarities on awareness of treatment and prevention of stroke among public and outpatients in Sub-Saharan Africa: a cross-sectional questionnaire study in Botswana
Ookeditse Ookeditse, Kebadiretse K. Ookeditse, Thusego R. Motswakadikgwa, Gosiame Masilo, Yaone Bogatsu, Baleufi C. Lekobe, Mosepele Mosepele, Henrik Schirmer, Stein H. Johnsen

TL;DR
This study in Botswana finds that public awareness of stroke treatment is higher than among outpatients, with age and information sources playing key roles.
Contribution
This is the first study in sub-Saharan Africa comparing stroke awareness between outpatients and the public based on age and information sources.
Findings
Awareness of medical therapy as acute stroke treatment was lower among outpatients compared to the public across all ages.
HIV/AIDS history and healthy diet were associated with lower awareness of both stroke treatment and prevention.
Educational campaigns should target age groups and use diverse information sources to improve stroke awareness.
Abstract
In this cross-sectional study from Botswana, we investigated awareness of acute stroke treatment and prevention among stroke-risk outpatients and the public based on age and sources of information, in addition to association of stroke risk factors with this awareness. Questionnaires on awareness of acute stroke treatment and prevention were administered by research assistants to a representative selection of outpatients and the public. The response rate was 93.0% for the public and 96.6% for outpatients. Public respondents had a mean age of 36.1 ± 14.5 years (age range 18–90 years) and 54.5% were females, while outpatients had a mean age of 37.4 ± 12.7 years (age range 18–80 years) and 58.1% were females. Awareness of medical therapy as acute stroke treatment was inadequate among outpatients (75.5% for public vs 43.4% for outpatients among all-age, p < 0.001), due to awareness…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
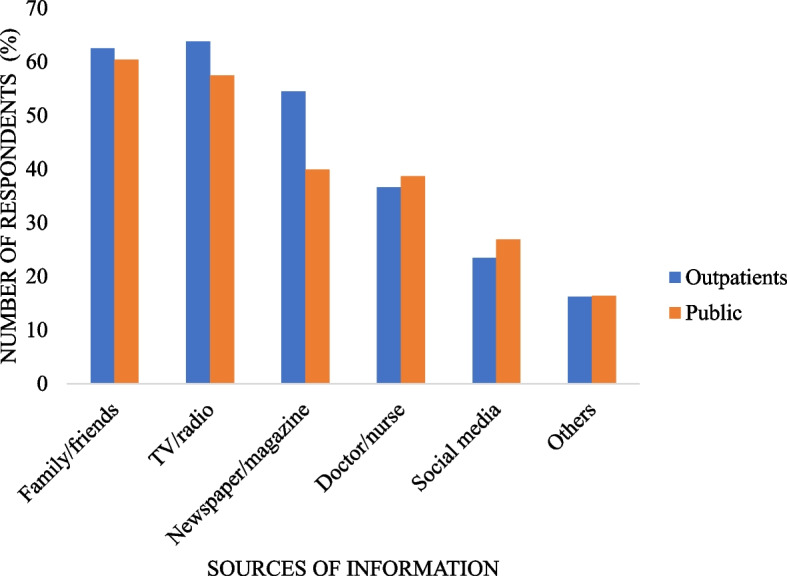 Figure 1
Figure 1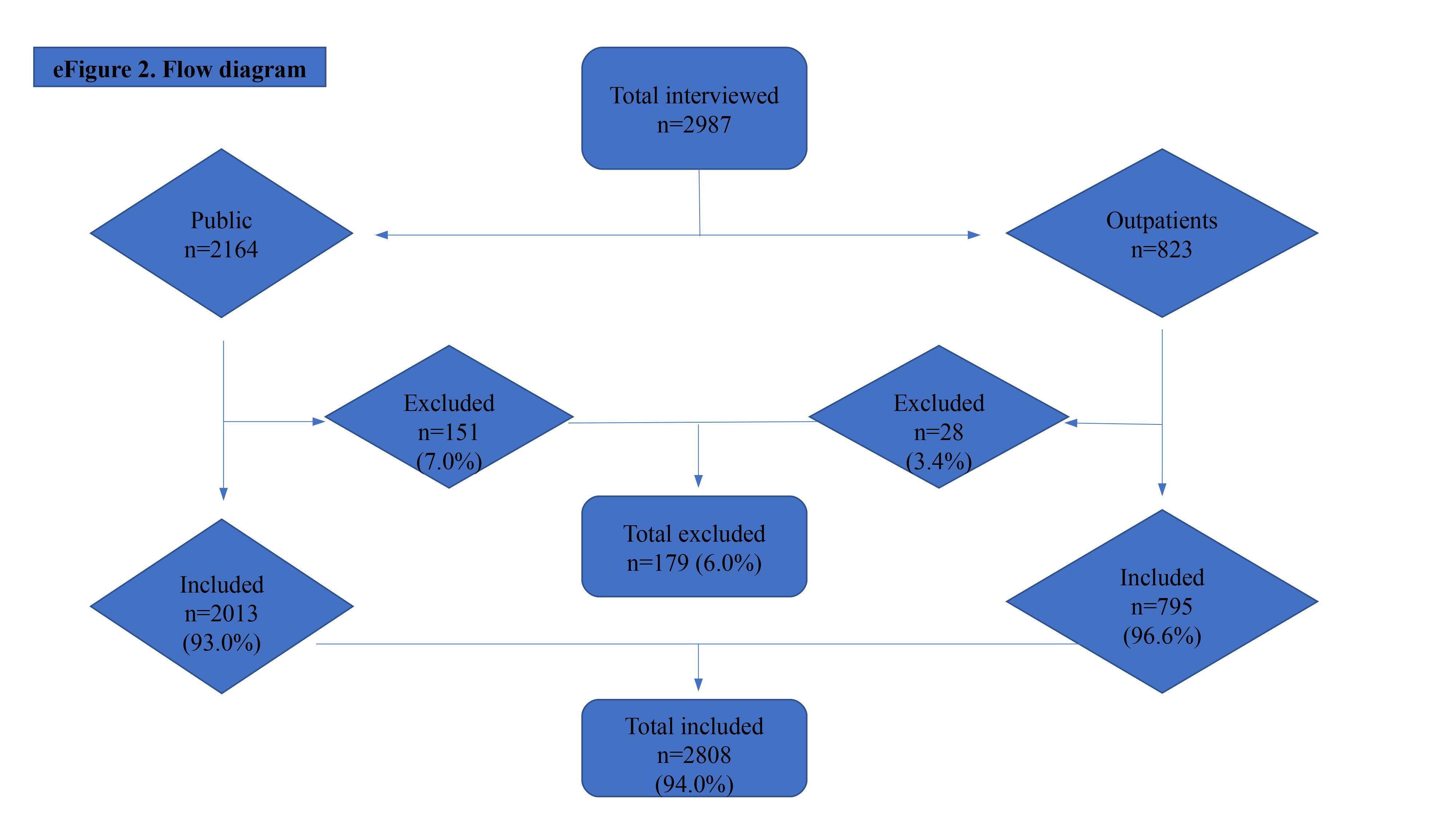 Figure 2
Figure 2- —UiT The Arctic University of Norway (incl University Hospital of North Norway)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Global Public Health Policies and Epidemiology
Introduction
Stroke was the sixth most common cause of death in Africa in 2019, with an increasing trend from eight position in 2000, according to World Health Organization (WHO) estimates [1]. Globally, the highest age-standardized incidence of stroke is in Africa with the incidence of stroke increased in east Asia and southern sub-Saharan Africa (SSA) from 1990 to 2016 [2, 3].
The emergence of revascularization methods (intravenous thrombolysis and/or thrombectomy) as an effective treatment for acute ischemic stroke, have increased the focus on stroke as an urgent and emergency disease as these treatments are time-dependent, as they improve clinical outcomes and dependency in disability-adjusted life-years (DALYs) [4–8]. Some studies showed patients as the most predominant barrier in stroke care, (up to 91% as prehospital delay in thrombolytic therapy) while one systematic review study demonstrated very low rates of thrombolysis (19%) in low- and middle-income countries (LMIC) compared to at least 50% in high-income countries (HIC) [9–13].
Majority of studies have focused on knowledge of stroke symptoms and risk factors, while a few on awareness of treatment and prevention [14–25]. There is none that we know of that has focused on awareness based on both age and sources of information concurrently in Sub-Saharan Africa or worldwide.
Objectives
- To determine awareness of treatment and prevention of stroke among outpatients and the public based on age and sources of information.
- To investigate if respondents’ sociodemographic and stroke risk factors are associated with stroke awareness.
Methods
Study design
Participants were recruited from Greater Gaborone which is located in the southeastern part of Botswana (is an upper middle-income country under LMIC in SSA), comprises six (6) districts and is the most populated area in the country.
Sampling of study places and population
All names of the four (4) districts in Greater Gaborone except Gaborone City and Lobatse town were put in a box, and two (2) names were blindly selected from the box as study places in addition to Gaborone city and Lobatse town. This similar method was also applied for healthcare facilities and communities in the districts. For Gaborone city, all areas were categorized into three socio-economic groups i.e., low, middle and high income. Names of more than three (3) areas with similar socio-economic category were put in a box and three (3) names were blindly selected to represent that specific category. If there were only two areas in the same category, they were both included.
The study sampled a variety of two groups of respondents, namely the public with/without stroke risk factors and representing the general public, and medical outpatients with at least one stroke risk factor (history of hypertension, stroke, heart diseases, obesity, overweight, diabetes, and Human immunodeficiency virus (HIV/AIDS), smoking, family history of stroke/ heart diseases, sedentary lifestyle, psychiatric disorders, and unhealthy diet). Public respondents were recruited from their homes or workplaces in both rural and urban areas. Outpatients from both primary and secondary healthcare facilities while waiting for or after their medical consultation.
We did not calculate sample size since there are no studies with data on prevalence and/or incidence of stroke in Botswana that could have helped us to calculate it. Therefore, we aimed at recruiting at least 70% of those targeted during data collection period.
Trained research assistants interviewed respondents verbatim. Each interviewer conducted a standardized, structured, one-to-one interview, according to a multi-sectioned questionnaire designed to guide interview and avoid bias. For the public, no more than two respondents from the same family/compound/ company were interviewed. The interviewer only intervened when asked to clarify any question, without giving correct answers. We sampled only odd numbers for outpatients queuing at healthcare facilities and households for the public in each area. For the public, we further sampled from different socio-economic levels i.e., high, moderate and low socioeconomic areas within Greater Gaborone.
Inclusion criteria
For the general public, respondents residing or working in Greater Gaborone, with or without any stroke risk factors. No more than two (2) respondents from same family, compound or company were included. Outpatients with at least one stroke risk factor visiting healthcare facilities in Greater Gaborone during study period but not admitted. Respondents aged ≥ 18 years. Respondents who understood English or local language, Setswana, and capable of consenting. Only respondents from the randomly selected places and not from the pilot study place were included.
Exclusion criteria
Respondents with cognitive/speech difficulties.
Data collection instrument
The survey instruments were adapted from previous surveys [14–25] with some modifications to reflect the recent American Heart Association/American Stroke Association (AHA/ASA) guidelines and European Stroke Organization guidelines [26, 27]. We tested the questionnaire in a pilot study with a sample of twenty-five respondents and some changes were made in the wording of questions based on the result of the pilot study. The questionnaire instruments were anonymous, electronic-based, written, and administered in English or local language (Setswana), consisting of both open- and closed-ended in nature and categorized into five sections (eFigure 1).
Sect. 1 included sociodemographic factors of respondents.
Sociodemographic characteristics: Variables included in this study were age (18–34 years, 35–49 years and ≥ 50 years), gender (male and female), education level (none/ unknown/ primary, secondary and tertiary), marital status (married/cohabiting and other), medical insurance (yes and no), and residing/ working together status (yes and no).
Sect. 2 comprised closed-ended questions on awareness of acute stroke treatment while Sect. 3 was made of both open- and closed-ended questions on awareness of stroke prevention.
Awareness of acute stroke treatment: It was assessed in 2 closed-ended questions. The first one: “Is acute stroke treatable?” Answers included yes, no, and no idea. The second question with 4 answers as follows: “Do you know any ways that can treat acute stroke?” Answers included no idea, rehabilitation, lifestyle, or medicine. We then dichotomized the responses into medicine vs other options.
Awareness of stroke prevention: It was assessed by both open- and closed-ended questions. “Is stroke preventable?” Answers included yes, no, or no idea. “Does reducing/treating stroke risk factors reduce likelihood of stroke?” Answers included no idea, no, or yes. We then dichotomized the responses into yes vs other options. “Do you know any ways that can reduce stroke risk factors?” The first part without answers and the second part with multiple choice answers: no idea, none, lifestyle, or medicine. Answers were then trichotomized into lifestyle vs medicine vs others.
Each correct answer in each Sect. 2 and 3 scored 1 point and was considered being aware. Each incorrect, unanswered, or unknown answer scored 0 point and was considered being unaware.
Section 4 and 5 comprised respondents’ stroke risk factors and sources of stroke information respectively.
Respondents’ stroke risk factors
Refer to previous study [28].
Information on physical activity at work, at home, during recreational or sporting activities, and leisure-time activities was obtained using part of the International Physical Activity Questionnaire with comparable variables [29]. Participants were asked about the specific activities that they regularly perform that increase breathing rate for at least 10 min, total duration per day, number of days in a week, and whether the individual perceived the activity as heavy, moderate, light, or no activity. For each participant, recorded activities were converted to metabolic equivalent task (MET)-minutes per week (min/wk) [29]. People participating in activities of less than 3.5 MET-min/wk were classified as no activity (sedentary lifestyle), 3.5- < 600 MET-min/wk as low, 600- < 3000 MET-min/ wk as moderate, and ≥ 3000 MET-min/wk as high level of physical activity.
Respondents were asked if they perceived their weight as underweight, normal, overweight or obese. We further measured weight and height, calculated BMI, and classified as defined by the WHO and National Institutes of Health (NIH) i.e., underweight as BMI < 18·5 kg/m^2^, normal BMI 18.5- < 25 kg/m^2^, overweight 25- < 30 kg/m^2^, and obesity as ≥ 30 kg/m^2^ [30, 31]. Height was measured twice to the nearest millimeter using a fixed, non-elastic plastic stadiometer, and the average height calculated. Body weight was measured in kilograms (to the second decimal place) using an auto-zeroing digital weight scale for adults dressed in light clothes and without shoes. Safeway auto-zeroing digital weight scales (Safeway Scale, South Africa) were used after calibration.
Sources of stroke information
Refer to previous study [28]. Sources of information were then stratified by awareness of acute stroke treatment and prevention.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or 95% confidence interval (CI). Categorical and ordinal variables were expressed as absolute frequency (n) and proportion (%) of the overall sample or subgroups. Outpatients and public groups’ awareness of stroke stratified by age and sources of information was compared using the chi-square test. Odds ratios were used to analyze awareness of both acute stroke treatment and prevention [32].
Mann–Whitney U/ Kruskal–Wallis H was used to assess association of respondents’ sociodemographic and stroke risk factors with awareness of stroke prevention and treatment. Bonferroni correction was applied for multiple comparisons. Statistical tests were two-tailed and reported statistically significant at p < 0.05. All statistical analyses were completed using SPSS 29 statistical software (SPSS Inc., Chicago, Illinois, USA).
Results
We interviewed 2987 respondents in a cross-sectional study from June-October 2019. We excluded 179 participants (151 from the public and 28 outpatients) because of missing either consent or substantial information that could be useful for the study (eFigure 2). We had a valid response of 2808 respondents (94.0%), comprising 2013 from the public (93.0%) and 795 outpatients (96.6%). The public had a mean age of 36.1 ± 14.5 years (age range 18–90 years), while outpatients had 37.4 ± 12.7 years (range 18–80 years). Public and outpatients comprised 54.8% and 57.2% females respectively. More information on respondents’ characteristics is elucidated in Table 1. Table 1. Sociodemographic and stroke risk factors among respondentsTotalPublicOutpatientsn = 2808n = 2013n = 795n (%)n (%)n (%)pSociodemographic factors****Gender Female1559(55.5)1104(54.8)455(57.2) Male1249(44.5)909(45.2)340(42.8)0.251Age category (years)missing 6missing 5missing 1 18–341501(53.6)1118(55.7)383(48.2) 35–49842(30.0)586(29.2)256(32.2) ≥50459(16.4)304(15.1)155(19.5) < 0.001Education level Primary or below363(12.9)257(12.8)106(13.3) Secondary1518(54.1)1108(55.0)410(51.6) Tertiary923(32.9)645(32.0)278(35.0) Unknown4(0.1)3(0.1)1(0.1)0.405Medical insurance Yes420(15.0)92(4.6)328(41.3) No2388(85.0)1921(95.4)467(58.7) < 0.001Marital status Married/cohabiting982(35.0)723(35.9)259(32.6) Others1826(65.0)1290(64.1)536(67.4)0.095Residing/working together Yes1121(39.9)954(47.4)167(21;0) No1687(60.1)1059(52.6)628(79.0) < 0.001Self-reported risk and other factors****History of hypertension Yes276(9.8)158(7.8)118(14.8) No2532(90.2)1855(92.2)677(85.2) < 0.001History of CVDS Yes196(7.0)116(5.8)80(10.1) No2612(93.0)1897(94.2)715(89.9) < 0.001Family history of stroke/heart diseases Stroke372(13.2)285(14.2)87(10.9) Heart diseases347(12.4)221(11.0)126(15.8) Both heart diseases and stroke389(13.9)202(10.0)187(23.5) None1700(60.5)1305(64.8)395(49.7) < 0.001BMI Underweight53(1.9)31(1.5)22(2.8) Normal2429(86.5)1850(91.9)579(72.8) Overweight215(7.7)120(6.0)95(11.9) Obesity111(4.0)12(0.6)99(12.5) < 0.001Healthy dietary status No1080(38.5)772(38.4)308(38.7) Yes1691(60.2)1213(60.3)478(60.1) Unknown37(1.3)28(1.4)9(1.1)0.855Alcohol consumption Current668(23.8)415(20.6)253(31.8) Former46(1.6)25(1.2)21(2.6) No2086(74.3)1569(77.9)517(65.0) Unknown8(0.3)4(0.2)4(0.5) < 0.001Smoking status Current337(12.0)198(9.8)139(17.5) Former43(1.5)22(1.1)21(2.6) No2421(86.2)1788(88.8)633(79.6) Unknown7(0.2)5(0.2)2(0.3) < 0.001Intensity of physical activity None2157(76.8)1573(78.1)584(73.5) Light105(3.7)62(3.1)43(5.4) Moderate483(17.2)337(17.0)140(17.6) High63(2.2)35(1.7)28(3.5) < 0.001History of HIV/AIDS Yes567(20.3)328(16.3)239(30.1) No2241(79.8)1685(83.7)556(69.9) < 0.001History of psychiatric diseases Yes89(3.2)0(0)89(11.2) No2719(96.8)2013(100.0)706(88.8) < 0.001Calculated risk factors****Physical activity intensity (Met min/week) Physical inactive2169(77.2)1575(78.2)594(74.7) Low (> 3,5–600)112(4.0)75(3.7)37(4.7) Moderate (> 600–3000)436(15.5)294(14.6)142(17.9) High (> 3000)91(3.2)69(3.4)22(2.8)0.078BMI Underweight (< 18.5)105(3.7)77(3.8)28(3.5) Normal (18.5 < 25)1169(41.6)877(43.6)292(36.7) Overweight (25 < 30)669(23.8)475(23.6)194(24.4) Obesity (≥ 30)856(30.5)579(28.8)277(34.8) Unknown9(0.3)5(0.2)4(0.5)0.005*NA *not applicable, *CVDS *cardiovascular diseases (diabetes, dyslipidemia, or heart diseases)Psychiatric diseases: depression or anxiety, *BMI *Body Mass Index, P:calculated using chi-squared
Awareness of acute stroke treatment
About 9 out of 10 respondents (88.7%) were aware of acute stroke treatment (90.8% of outpatients vs 87.9% of public), while 66.4% recognized medical therapy as acute stroke treatment (75.5% of public vs 43.3% of outpatients, p < 0.001) (Table 2). For all respondents, the odds of being aware of both acute stroke treatment and medical therapy as a way of acute treatment was 1873 times (for public 2949 vs for outpatients 133 times) higher than being aware of acute stroke treatment only (p < 0.001) (eTable 1). Table 2. Public and outpatients awareness of acute treatment and prevention of stroke stratified by ageTotalOutpatientsPublicAge (years)n(%)n(%)n(%)pAwareness of acute stroke treatmentAll2492(88.7)721(90.8)1766(87.9)0.60618–341323(88.1)345(90.1)978(87.5)0.74235–49757(89.9)232(90.6)525(89.6)0.920 > 50407(88.7)144(92.9)263(86.5)0.627Awareness of medical therapy as acute stroke treatmentAll1864(66.4)344(43.3)1517(75.5) < 0.00118–341016(67.7)168(43.9)848(75.8) < 0.00135–49549(65.2)106(41.4)443(75.6) < 0.001 > 50296(64.5)70(45.2)226(74.3)0.006Awareness of stroke preventionAll2089(74.4)647(81.5)1437(71.6)0.05518–341124(74.9)305(79.6)819(73.3)0.38335–49619(73.5)208(81.3)411(70.1)0.228 > 50341(74.3)134(86.5)207(68.1)0.135Awareness of stroke risk factor prevention as stroke preventionAll2471(88.0)751(94.6)1714(85.4)0.10218–341334(88.9)363(94.8)971(86.9)0.32135–49737(87.5)242(94.5)495(84.5)0.316 > 50394(85.8)146(94.2)248(81.6)0.337Spontaneously recalling at least one way of preventing stroke risk factorsAll932(33.2)246(31.0)686(34.2)0.35318–34531(35.4)133(34.7)398(35.6)0.86035–49288(34.2)76(29.7)212(36.2)0.284 > 50113(24.6)37(23.9)76(25.0)0.865Identifying lifestyle changes/medicine as a way of prevention of stroke risk factorsAll2648(94.3)765(96.3)1877(93.5)0.62018–341414(94.2)365(95.3)1049(93.8)0.85735–49810(96.2)252(98.4)558(95.2)0.759 > 50418(91.1)148(95.5)270(88.8)0.621Identified none of the ways of preventing stroke risk factorsAll160(5.7)29(3.7)131(6.5)0.03118–3487(5.8)18(4.7)69(6.2)0.45035–4932(3.8)4(1.6)28(4.8)0.082 > 5041(8.9)7(4.5)34(11.2)0.084Spontaneously recalled ways of preventing stroke risk factors****Physical activityAll661(23.5)183(23.0)478(23.8)0.80018–34384(25.6)102(26.6)282(25.2)0.74235–49197(23.4)55(21.5)142(24.2)0.587 > 5080(17.4)26(16.8)54(17.8)0.867Healthy dietAll358(12.8)100(12.6)258(12.8)0.91018–34218(14.5)56(14.6)162(14.5)0.96535–4999(11.8)28(10.9)71(12.1)0.743 > 5041(8.9)16(10.3)25(8.2)0.613Avoid/reduce high alcohol intakeAll132(4.7)36(4.5)96(4.8)0.85118–3482(5.5)23(6.0)59(5.3)0.71135–4936(4.3)11(4.3)25(4.3)0.980 > 5014(3.1)2(1.3)12(3.9)0.232Cessation of smokingAll106(3.8)31(3.9)75(3.7)0.88118–3463(4.2)17(4.4)46(4.1)0.85535–4933(3.9)12(4.7)21(3.6)0.602 > 5010(2.2)2(1.3)8(2.6)0.481Avoid stressAll69(2.5)18(2.3)51(2.5)0.76918–3437(2.5)10(2.6)27(2.4)0.87435–4927(3.2)6(2.3)21(3.6)0.496 > 505(1.1)2(1.3)3(1.0)0.844Medication adherence/follow-ups/education from healthcare professionalsAll59(2.1)20(2.5)39(1.9)0.51218–3432(2.1)10(2.6)22(2.0)0.61835–4921(2.5)7(2.7)14(2.4)0.843 > 506(1.3)3(1.9)3(1.0)0.558Reducing fatty foods intakeAll57(2.0)12(1.5)45(2.2)0.36918–3432(2.1)6(1.6)26(2.3)0.50835–4919(2.3)5(2.0)14(2.4)0.774 > 506(1.3)1(0.6)5(1.6)0.505Reducing salt consumptionAll33(1.2)10(1.3)23(1.1)0.85918–3415(1.0)4(1.0)11(1.0)0.93435–4911(1.3)4(1.6)7(1.2)0.751 > 507(1.5)2(1.3)5(1.6)0.818Eating more fruits and vegetablesAll15(0.5)1(0.1)14(0.7)0.11918–3412(0.8)0(0.0)12(1.1)0.05935–493(0.4)1(0.4)2(0.3)0.930 > 500(0.0)0(0.0)0(0.0)NALose weightAll7(0.2)2(0.3)5(0.2)0.99118–345(0.3)2(0.5)3(0.3)0.63835–491(0.1)0(0.0)1(0.2)0.552 > 501(0.2)0(0.0)1(0.3)0.552*NA *not applicable, p: calculated using chi-squared
Awareness of stroke prevention
A total of 2089 respondents (74.4%) were aware of stroke prevention (81.5% of outpatients vs 71.6% of public), 88.0% were aware that stroke risk factors’ prevention (reducing/ treating stroke risk factors) reduced the likelihood of stroke (94.6% outpatients vs 85.4% public), while 33.2% recalled spontaneously at least one way of preventing stroke risk factors (31.0% of outpatients vs 34.2% of public) (Table 2).
About 9 out of 10 outpatients (96.3%) and 93.5% of public identified either lifestyle changes or medicine/medication as a way of preventing stroke risk factors, while 3.7% of outpatients vs 6.5% of public (p < 0.05) could not identify any means of preventing stroke risk factors.
About 1 out of 4 respondents (23.5%) spontaneously recalled physical activity which was the highest way recalled (23.8% of public vs 23.0% of outpatients), while 0.2% recalled losing weight to maintain normal weight as lowest (0.3% of outpatients vs 0.2% of public) way of preventing stroke risk factors (Table 2).
For all respondents, odds of being aware of both prevention of stroke and reducing or treating stroke risk factors was 21 times (for public 22 vs for outpatients 14 times) higher than of being aware of stroke prevention only (p < 0.001) (eTable 1).
Sources of stroke information
Highest sources of information were TV/radio (63.8% for outpatients vs 57.5% for public) and family/friends (62.5% for outpatients vs 60.4% for public) while the lowest was others category (16.2% for outpatients vs 16.4% for public)) (Fig. 1). Outpatients were more likely than the public to get stroke information from newspaper/magazine (54.5% vs 39.9%, p < 0.001).Fig. 1. Sources of stroke information among the public and outpatients
Regarding medical therapy as acute stroke treatment among almost all ages, the public was more likely than outpatients to get stroke information (p < 0.001) from almost all sources of information (Table 3). For stroke prevention, both groups demonstrated awareness rates of at least 67% for almost all sources except for others category among the public (63.0%). Outpatients were more likely than the public to get stroke information from family/ friends (83.9% vs 70.5%, p < 0.05). Table 3. Respondents awareness differences of acute stroke treatment and prevention by sources of stroke information stratified by agePublic****OutpatientsAge(years)n = 2008No. aware (% aware)n = 794No. aware (% aware)pMedical therapy as acute treatment****Family or friends All1216938(77.1)496238(48.0) < 0.001 18–34651497(76.3)241121(50.2)0.002 35–49370292(78.9)14764(43.5) < 0.001 ≥50195149(76.4)10853(49.1)0.041Tv or radio All1152953(82.5)506190(37.5) < 0.001 18–34650543(83.5)22884(36.8) < 0.001 35–49337276(81.9)17966(36.9) < 0.001 ≥50165131(79.4)9940(40.4)0.005Newspaper or magazine All799675(84.5)432162(37.5) < 0.001 18–34463407(87.9)20481(39.7) < 0.001 35–49256209(81.6)15452(33.8) < 0.001 ≥508059(73.8)7429(39.2)0.041Social Media (Internet, Facebook, WhatsApp) All542456(84.1)18759(31.7) < 0.001 18–34312269(86.2)10940(36.7) < 0.001 35–49194159(82.0)5714(24.6) < 0.001 ≥503628(77.8)205(25.0)0.055Doctor or nurse All777674(86.7)290112(38.6) < 0.001 18–34438399(91.1)13958(41.7) < 0.001 35–49245201(82.0)9732(33.0) < 0.001 ≥509474(78.7)5422(40.7)0.040Others (school, patients, experience) All330185(56.1)12974(57.4)0.906 18–34208122(58.7)8348(57.8)0.952 35–497842(53.8)2214(63.6)0.705 ≥504421(47.7)2412(50.0)0.918Stroke prevention****Family or friends All1216857(70.5)496416(83.9)0.042 18–34651476(73.1)241200(83.0)0.293 35–49370250(67.6)147122(83.0)0.198 ≥50195131(67.2)10894(87.0)0.182Tv or radio All1152896(77.8)506435(86.0)0.228 18–34650526(80.9)228189(82.9)0.843 35–49337248(73.6)179155(86.6)0.266 ≥50165122(73.9)9991(91.9)0.273Newspaper or magazine All799645(80.7)432388(89.8)0.241 18–34463393(84.9)204176(86.3)0.898 35–49256187(73.0)154142(92.2)0.144 ≥508065(81.3)7470(94.6)0.535Social Media (Internet, Facebook, WhatsApp) All542420(77.5)186160(86.0)0.427 18–34312256(82.1)10993(85.2)0.823 35–49194138(71.1)5749(86.0)0.434 ≥503626(72.2)2018(90.0)0.614Doctor or nurse All777608(78.2)290246(84.8)0.454 18–34438367(83.8)139116(83.5)0.976 35–49245173(70.6)9784(86.6)0.288 ≥509468(72.3)5446(85.2)0.549Others (school, patients, experience) All330208(63.0)12999(76.7)0.263 18–34208127(61.1)8368(81.9)0.177 35–497858(74.4)2217(77.3)0.922 ≥504423(52.3)2414(58.3)0.828p: calculated using chi-squared
Respondents’ awareness differences of medical therapy as acute stroke treatment, and prevention by sources of stroke information stratified by age
Odds of being aware of medical therapy as acute stroke treatment due to getting information from family/friends were 1.7 times higher for outpatients while 1.2 times higher for the public than being aware without getting information from this source (eTable 2). Odds were also at least 2 times higher for the public due to getting information from doctor/nurse, newspaper/magazine, TV/radio, and social media while for outpatients, odds were 0.7 times or less lower due to getting information from these sources.
Odds of being aware of stroke prevention due to getting information from TV/radio and newspaper/magazine were at least 2 times higher (2 times for the public vs 2.2 times higher for outpatients, and 2.2 times for the public vs 3.5 times higher for outpatients respectively) than being aware without getting information from these sources (eTable 2).
Odds were also more than 1 time higher for outpatients due to getting information from family/friends while for the public due to getting information from doctor/nurse and social media.
Association of sociodemographic factors with awareness of acute stroke treatment (medical therapy) and prevention
Lower awareness of acute stroke treatment (p < 0.05) was associated with medical insurance, not residing/working together, history of hypertension, history of CVDS, family history of both stroke and heart diseases, healthy diet, current drinkers, former drinkers, current smokers, history of HIV/AIDS, light and moderate physical intensity (Table 4). Lower awareness of stroke prevention (p < 0.05) was associated with female gender, no medical insurance, married/cohabiting status, residing/ working together, family history of stroke, healthy diet, history of HIV/AIDS, history of psychiatric diseases, underweight, normal weight, and overweight. Table 4. Mann–Whitney U/ Kruskal–Wallis H- Association of awareness of acute stroke treatment and prevention with sociodemographic factors among respondentsMedical therapy as acute treatment****PreventionMean (95% CI)Mean (95% CI)Sociodemographic factors****Gender Female0.66(0.64–0.68)0.73(0.71–0.75) Male0.67(0.64–0.69)0.76(0.74–0.79)p0.6360.038d0.039Age category (years) 1. 18–340.68(0.65–0.70)0.75(0.73–0.77) 2. 35–490.65(0.62–0.68)0.74(0.71–0.77) 3. ≥ 500.64(0.60–0.69)0.74(0.70–0.78)p0.3000.767dEducation level 1.Primary, or unknown0.68(0.63–0.73)0.73(0.68–0.78) 2. Secondary0.67(0.64–0.69)0.74(0.71–0.76) 3. Tertiary0.65(0.62–0.68)0.76(0.73–0.79)p0.4970.313dMedical insurance Yes0.44(0.40–0.49)0.83(0.79–0.86) No, unknown0.70(0.68–0.72)0.73(0.71–0.75)p < 0.001 < 0.001d0.1960.079Marital status Married/ cohabiting0.67(0.64–0.70)0.71(0.69–0.74) Others0.66(0.64–0.68)0.76(0.74–0.78)p0.5500.010d0.049Residing/working together Yes0.74(0.71–0.76)0.70(0.67–0.72) No0.61(0.59–0.64)0.77(0.75–0.79)p < 0.001 < 0.001d0.1280.087Self-reported risk factors****History of hypertension Yes0.61(0.55–0.66)0.74(0.69–0.79) No, unknown0.67(0.65–0.69)0.74(0.73–0.76)p0.0300.847d0.041History of CVDS Yes0.59(0.52–0.66)0.77(0.71–0.83) No0.67(0.65–0.69)0.74(0.73–0.76)p0.0270.478d0.042Family history of stroke/heart diseases 1. None0.69(0.67–0.71)0.76(0.74–0.78) 2. Both heart diseases and stroke0.58(0.53–0.63)0.79(0.75–0.83) 3. Heart diseases0.63(0.58–0.68)0.71(0.66–0.76) 4. Stroke0.67(0.62–0.72)0.66(0.61–0.71)p < 0.001; 1 vs 2 < 0.001 < 0.001; 1 vs 4 < 0.001, 2 vs 4 < 0.001d0.0060.008Healthy dietary status No, unknown0.69(0.66–0.72)0.78(0.76–0.80) Yes0.65(0.62–0.67)0.72(0.70–0.74)p0.016 < 0.001d0.0450.067Alcohol consumption 1. No, unknown0.69(0.67–0.71)0.74(0.72–0.76) 2. Current0.59(0.55–0.62)0.76(0.73–0.79) 3. Former0.50(0.35–0.65)0.76(0.63–0.89)p < 0.001; 1 vs 3 = 0.019, 1 vs 2 < 0.0010.502d0.011Smoking status 1. No, unknown0.68(0.66–0.70)0.75(0.73–0.77) 2. Current0.54(0.49–0.60)0.71(0.66–0.76) 3. Former0.60(0.45–0.76)0.74(0.61–0.88)p < 0.001; 1 vs 2 < 0.0010.362d0.009History of HIV/AIDS Yes0.50(0.45–0.54)0.64(0.60–0.68) No, unknown0.71(0.69–0.73)0.77(0.75–0.79)p < 0.001 < 0.001d0.1790.115History of psychiatric diseases Yes0.75(0.66–0.84)0.65(0.55–0.75) No0.66(0.64–0.68)0.75(0.73–0.76)p0.0710.043d0.038Calculated risk factors****Intensity of physical activity 1. None, unknown0.69(0.67–0.70)0.75(0.73–0.77) 2. Light0.56(0.47–0.66)0.67(0.58–0.76) 3. Moderate0.59(0.55–0.64)0.73(0.69–0.77) 4. High0.63(0.53–0.73)0.78(0.69–0.87)p < 0.001; 1 vs 2 = 0.044, 1 vs 3 = 0.0010.180d0.007BMI 1. Underweight (< 18.5)0.65(0.55–0.74)0.62(0.52–0.71) 2. Normal, unknown (18.5 < 25)0.65(0.62–0.67)0.71(0.69–0.74) 3. Overweight (25 < 30)0.66(0.62–0.69)0.74(0.70–0.77) 4. Obesity (≥ 30)0.70(0.67–0.73)0.81(0.78–0.83)p0.111 < 0.001; 1 vs 4 < 0.001, 2 vs 4 < 0.001, 3 vs 4 = 0.010d0.011*NA *not applicable, *CVDS *cardiovascular risk factors (diabetes, dyslipidemia, stroke, or heart diseases), d: effect sizePsychiatric diseases: depression or anxiety, BMI: Body Mass Index, MI: myocardial infarction
Discussion
In this study, awareness of acute stroke treatment was adequate among respondents, with both the public and outpatients scoring more than 85% among all ages and without any significant differences. Despite this, only 3 out of 5 respondents (66.4%) recognized medical therapy as a way of acute stroke treatment i.e., 43.4% of outpatients vs 75.5% of public for all-age due to similar trend for all ages. These rates are lower compared to a Canadian study by Metias et al. comparing 2 cohorts (2010 and 2015), that showed public and patients had higher awareness rates of 87.9% in 2010 and 82.5% in 2015 [17]. Our findings for outpatients however, demonstrated higher awareness than in some patients’ studies [15, 16, 18–20] that showed rates between 3.6–26.2%. It is uncertain why the public had more awareness than outpatients when one would have expected outpatients to have better awareness since they are more frequently in contact with healthcare professionals. The reasons could be due to that outpatients are already preoccupied with their diseases as only few of our outpatients had stroke in this study, while the public have probably more time to learn about various diseases. The other reason could be that the public get stroke information from other sources which outpatients do not use or have access to.
We found that awareness of stroke risk factors’ prevention (closed-ended question) was adequate for outpatients and the public among all ages (lowest score about 80%) while awareness in an open-ended question was inadequate for both respondents among all ages (highest score less than 37%). In both groups, 81 −95% identified at least one way of preventing stroke risk factors while only one third spontaneously recalled at least one. Even though awareness of stroke prevention was sufficient, there was low awareness of spontaneously recalling means of preventing stroke risk factors. Some previous patients’ studies [21–25] have shown variations in awareness rates (21.7–90.8%).
Physical activity (regular exercises) was spontaneously recalled by 23.0% of outpatients, reducing/avoiding excessive alcohol drinking by 4.5%, quitting smoking by 3.9%, reducing fatty foods intake by 1.5%, whereas only 0.1% recalled eating more fruits/ vegetables. In an Ethiopian closed-ended study among hypertensive patients [21], the corresponding numbers were 27.1%, 62.7%, 51.7%, 24.1%. and 7.8%. Also, the awareness of medication adherence/treating or controlling cardiovascular diseases (2.5%) and good weight control (0.3%) were much lower in our study compared to the Ethiopian study [21]. Although some of the differences could be attributed to different study population (mixture of various cardiovascular diseases vs. hypertensives), the low numbers clearly indicate a great need for improved public health and lifestyle information in Botswana.
Among all ages, the public had significantly higher awareness than outpatients for medical therapy as acute stroke treatment among those who got stroke information from all sources i.e., doctors/ nurses, social media, newspapers/magazines, TV/ radio, and family/ friends.
Outpatients’ awareness by different sources of information ranged between 24.6% and 63.6%, which is insufficient, compared to the public who had the lowest awareness rates of 47.7–58.7% for others category, while others were more than 73%. This demonstrates that all sources of information can be used effectively to relay stroke information as shown among the public. This calls for more effort and using the best tools for each age group among outpatients to effectively educate them about stroke if we are to reduce stroke morbidities and mortalities. Awareness rates of stroke prevention by sources of information were high, with outpatients among all-age having a higher rate than the public among those who got stroke information from family/ friends. Despite this, the public among all-age had awareness rate of 70.5% which is sufficient. This could be due to that outpatients listen to and trust mostly those who are closest to them when they are sick.
Our study did not show any association of awareness of medical therapy as acute stroke treatment with age, gender, or education. This contrasts some studies that showed association with young age [15, 18], high education [15, 20], and male gender [18], even though some questions were about the treatment of stroke not specifying acute stroke treatment and were open-ended. The differences can also be explained by differences in the study population, the definition of young age, and the question in our study did not specify the type or name of the medication.
We found that lower awareness of stroke prevention was significantly associated with female gender and being married/cohabiting, which contrasts an Indian study that did not show any association [22]. Our study did not demonstrate any associations with age, which also contrasts the afore-mentioned Ethiopian and Indian studies [21, 22]. Neither did we find any association between awareness and education. This resonates with the Indian study [22] but not with a Chinese study that showed an association with education [24]. Our study showed a significant association of lower awareness of stroke prevention with a healthy diet which contrasts the Indian study that did not show any association with diet [22]. The differences can be explained by differences in the study population (age, region, time of study, type of patients), the way awareness was assessed i.e., based on either a single question or multiple questions, and the nature of questions (either closed- or open-ended).
Strength and limitations
Our study adds to the sparse literature worldwide on awareness of stroke prevention and acute treatment among outpatients and the public concurrently. This is the first study to access awareness of stroke treatment and prevention after stratifying for age and in addition to sources of information. All information from the questionnaires was collected through standardized face-to-face interviews. In our study assessment of awareness of stroke prevention and acute treatment was performed through closed-ended questions, while awareness of means of stroke risk factors’ prevention was assessed with both open- and closed-ended questions even though closed-ended questions might overestimate the real level of awareness, as revealed by one previous study [33].
There are some limitations to this study. First, not all means of stroke/ risk factors’ prevention were included in this study and should not be weighted equally because some are easily identifiable and more common than others. Second, some subgroups had small samples, therefore, reducing statistical power to calculate differences. Third, self-reported factors/characteristics are prone to bias. Fourth, for acute stroke treatment we did not specify the type of medication or should have given more options for types of medications. Fifth, we could not cover all areas of stroke prevention and treatment as it is a broad topic e.g., thrombectomy, rehabilitation, etc. Lastly, there may be differences in sociodemographic and stroke risk factors between responders and non-responders that we are unable to account for. Despite all these limitations, a reasonably high response rate of 94% was attained and therefore these results represent current knowledge of both outpatients and the public in greater Gaborone.
Conclusion
Despite adequate awareness of stroke prevention among respondents and adequate awareness of acute stroke treatment among the public for closed-ended questions, there are still gaps in awareness that need to be addressed among various subgroups and even after adjusting for age. The results call health policymakers and other stakeholders for urgent awareness campaigns targeting all these subgroups associated with low awareness as it might help increase the rate of thrombolysis and /thrombectomy, and reduce risk factors through lifestyle interventions and medical adherence hence reduce stroke mortality and morbidity in Sub-Saharan Africa. To increase the numbers reaching time dependent therapy the population needs to know stroke symptoms, i.e. FAST, as awareness of rehabilitation and lifestyle will probably not have magnitude effect on the number available for reperfusion therapy but can have on recovery of poststroke.
Supplementary Information
Additional file 1.Additional file 2.Additional file 3.Additional file 4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Global health estimates 2019: Leading cause of death and disability: A visual summary of global and regional trends in 2000–2019. Geneva: World Health Organization; 2020. https://www.who.int/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019.
- 2GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019:18: 439–5810.1016/S 1474-4422(19)30034-1PMC 649497430871944 · doi ↗ · pubmed ↗
- 3Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. New England J Med. 2008:359:1317–29.10.1056/NEJ Moa 080465618815396 · doi ↗ · pubmed ↗
- 4Wahlgren N, Ahmed N, Davalos A, Hacke W, Millán M, Muir K, et al. Thrombolysis with alteplase 3–4.5 h after acute ischaemic stroke (SITS-ISTR): an observational study. Lancet 2008:372:1303–9.10.1016/S 0140-6736(08)61339-218790527 · doi ↗ · pubmed ↗
- 5Wardlaw JM, Murray V, Berge E, Del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database System Rev. 2009:CD 000213. https://www.scirp.org/reference/referencespapers?referenceid=737327.10.1002/14651858.CD 00021312917889 · doi ↗ · pubmed ↗
- 6Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010:375(9727):1695–1703.10.1016/S 0140-6736(10)60491-620472172 · doi ↗ · pubmed ↗
- 7Fransen PS, Berkhemer OA, Lingsma HF, Beumer D, Van Den Berg LA, Yoo AJ, et al. Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands Investigators. Time to reperfusion and treatment effect for acute ischemic stroke: a randomized clinical trial. JAMA Neurol. 2016:73(2):190–196.10.1001/jamaneurol.2015.388626716735 · doi ↗ · pubmed ↗
- 8Baatiema L, de-Graft Aikins A, Sav A, Mnatzaganian G, Chan CKY, Somerset S. Barriers to evidence-based acute stroke care in Ghana: a qualitative study on the perspectives of stroke care professionals. BMJ Open. 2017:7(4):e 015385.10.1136/bmjopen-2016-015385 PMC 571966328450468 · doi ↗ · pubmed ↗