A Dilemma in the Diagnosis of Group A Streptococcus (GAS) Meningitis Versus Drug-Induced Aseptic Meningitis: A Case Report
Rahul Sharma, Nadim Jaafar, Navami Guru, Edward Oh, Siddartha Guru

TL;DR
This case report describes a diagnostic challenge between GAS meningitis and drug-induced aseptic meningitis in a patient with S. pyogenes bacteremia.
Contribution
The paper presents a unique clinical case highlighting diagnostic uncertainty in GAS meningitis versus drug-induced aseptic meningitis.
Findings
CSF tests were inconclusive for bacterial meningitis despite GAS bacteremia.
The patient's meningitis symptoms improved after avoiding NSAIDs and receiving antibiotics.
A four-week course of ceftriaxone was administered to treat possible GAS meningitis.
Abstract
Group A Streptococcus (GAS), also called Streptococcus pyogenes, is a rare cause of adult meningitis. In recent years, many outbreaks of invasive S. pyogenes infections in Europe, involving the emm1.0 subtype of the M1UK lineage, have led to a rising prevalence of GAS meningitis. We present a case with a diagnostic dilemma involving a 55-year-old female with otitis media, S. pyogenes bacteremia, and symptoms of meningitis. However, cerebrospinal fluid (CSF) tests were not completely consistent with bacterial meningitis, with normal glucose levels on CSF analysis, no organism seen on gram stain, and no growth on CSF culture. Drug-induced aseptic meningitis (DIAM) was considered, given the patient's use of ibuprofen prior to admission, and thus, non-steroidal anti-inflammatory drugs (NSAIDs) were avoided during her hospitalization. The GAS bacteremia was treated with intravenous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
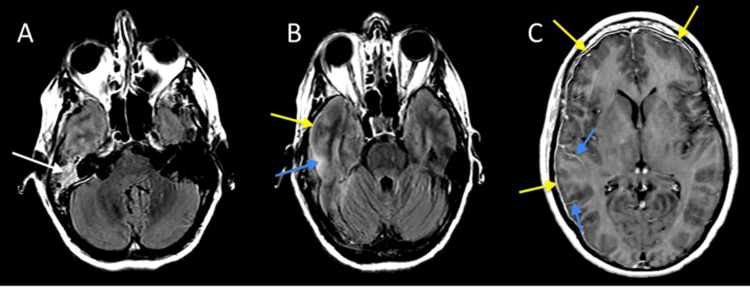 Figure 1
Figure 1| Vitals | Values |
| Temperature | 37.7ºC |
| Blood pressure | 144/86 |
| Heart rate | 109 heartbeats per minute |
| Respiratory rate | 16 breaths per minute |
| SpO2 | 97% on room air |
| Labs | Values | Reference |
| White blood cell count | 33.64 x 103/uL | 4.00 - 11.00 x 103/uL |
| Bands manual | 37.8% | 3 - 17% |
| Hemoglobin | 12.4 g/dL | 12.5 - 15.0 g/dL |
| Platelets | 290 x 103/uL | 150 - 450 x 103/uL |
| Creatinine | 0.56 mg/dL | 0.40 - 1.10 mg/dL |
| Lactic acid | 1.4 mmol/L | 0.5 - 1.9 mmol/L |
| CSF studies | Result | Normal values | Interpretation |
| Glucose | 96 mg/dL | 40 - 70 mg/dL | High |
| Total protein | 164.4 mg/dL | 15 - 45 mg/dL | High |
| WBC | 7188/cumm | 0 - 6/cumm | High |
| RBC | 0/cumm | 0/cumm | Normal |
| Neutrophil % | 96% | 0% | High |
| HSV PCR | Not detected | - | - |
| VZV PCR | Not detected | - | - |
| West Nile antibodies IgM | IgM < 0.6 | IgM < 0.6 | Normal |
| West Nile antibodies IgG | IgG < 1.3 | IgG < 1.3 | Normal |
| VDRL | Non-reactive | - | - |
| Gram-stain | No organisms or PMNs | - | - |
| Bacterial culture | No growth | - | - |
| Fungal culture | No growth | - | - |
| Acid-fast bacilli culture | No growth | - | - |
| Antibiotics | Minimum inhibitory concentration (MIC) | Result |
| Amoxicillin | <=0.25 mcg/mL | Susceptible |
| Cefepime | <=0.0625 mcg/mL | Susceptible |
| Cefotaxime | <=0.0625 mcg/mL | Susceptible |
| Ceftriaxone | <=0.0625 mcg/mL | Susceptible |
| Clindamycin | 0.0625 mcg/mL | Susceptible |
| Erythromycin | 0.0625 mcg/mL | Susceptible |
| Levofloxacin | 1.0 mcg/mL | Susceptible |
| Linezolid | 1.0 mcg/mL | Susceptible |
| Meropenem | <=0.0625 mcg/mL | Susceptible |
| Penicillin | <=0.03125 mcg/mL | Susceptible |
| Vancomycin | 0.5 mcg/mL | Susceptible |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Bacterial Infections and Vaccines
Introduction
Group A Streptococcus (GAS), also known as Streptococcus pyogenes, is a gram-positive, beta-hemolytic bacterium that is present on the skin and mucosal surfaces. It commonly causes pharyngitis, skin and soft tissue infections, and otitis media, but can cause invasive infections such as necrotizing fasciitis, bacteremia, and, rarely, meningitis [1]. Invasive GAS infections, including meningitis, have risen over the past two decades in the US, with approximately 9,700 cases in 1997 to about 27,400 cases in 2022 [2]. There is no surveillance data specifically for GAS meningitis currently in the US, but the prevalence of GAS meningitis has been increasing worldwide [3,4]. Drug-induced aseptic meningitis (DIAM) can present similarly to bacterial meningitis, with symptoms of fever, meningeal symptoms, headaches, and altered mental status. Cerebrospinal fluid (CSF) studies usually show numerous neutrophils and elevated protein, making it difficult to differentiate from bacterial meningitis.
Case presentation
A 55-year-old female with a history of hypertension and paroxysmal atrial fibrillation developed right-sided ear pain and fullness about two weeks prior to admission. About 10 days prior to admission, she noticed mild hearing difficulties and, hence, presented to urgent care, where she was diagnosed with otitis media and cerumen impaction. She was prescribed oral amoxicillin and ofloxacin ear drops. Despite being on antibiotics for one week, she had worsening symptoms, including a new onset headache. Her primary care physician referred her to ENT and asked her to continue the antibiotics. The patient reported consuming excessive amounts of ibuprofen to control her headaches and ear pain. The day prior to admission, she became confused with progressively worsening lethargy; her husband was concerned, so he brought her to the Emergency Department (ED) for further evaluation.
In the ED, she was afebrile, normotensive, and tachycardiac (Table 1), and on physical examination, she was alert and oriented but slow to respond to questions. She had decreased hearing in the right ear, and on evaluation with an otoscope, there was debris and drainage in the right external auditory canal. A limited view of the tympanic membrane was noted, but she was able to discern mild erythema of the tympanic membrane. A few hours later, in the ED, she developed a fever of 39.2°C, triggering a full sepsis work-up. At the time, she denied photophobia or neck stiffness. Labs revealed leukocytosis with bandemia, mild anemia, and normal lactic acid and creatinine levels (Table 2).
Two sets of peripheral blood cultures were drawn prior to broad-spectrum antibiotics for empiric meningitis coverage with ceftriaxone, vancomycin, acyclovir, and ampicillin, together with dexamethasone. Less than 30 minutes after initiating antibiotics, a lumbar puncture was performed. The CSF showed 7188/cumm white blood cells (WBCs) with 96% neutrophilic predominance, elevated glucose of 96 mg/dL, and elevated protein of 164 mg/dL (Table 3). The serum glucose level at the time of lumbar puncture was 128 mg/dL. The CSF gram stain was negative. In addition to normal glucose levels, these findings were consistent with aseptic meningitis, particularly DIAM, given the use of ibuprofen prior to admission. Thus, a recommendation was made to hold any further non-steroidal anti-inflammatory drugs (NSAIDs) and continue empiric antibiotics until further CSF studies resulted.
Overnight, she remained febrile, and early in the morning on hospital day (HD) 2, she had worsening confusion and concern for right-sided weakness. The stroke response team was activated; the computed tomography (CT) of the head without contrast and CT perfusion of the head and neck showed no evidence of infarction, acute bleed, mass lesion, or large vessel occlusions. Magnetic resonance imaging (MRI) of the brain, with and without contrast, done later that day, showed complicated right mastoiditis/otitis with suspected adjacent early right temporal cerebritis and findings raising the possibility of asymmetric leptomeningitis and pachymeningitis/reactive dural thickening, right greater than left, with no empyema or abscess (Figures 1A-1C). She had no right-sided weakness a few hours later that day on the exam but continued to be confused. The Lyme serologies, Legionella, and streptococcal urine antigens were all negative.
MRI brain with contrast(A) Axial T2 FLAIR MRI of the brain at the level of the temporal bones demonstrates right mastoid-middle ear hyperintensity (white arrow), consistent with otomastoiditis. (B) Axial T2 FLAIR MRI of the brain just superior to Figure 1A shows pachymeningeal thickening with hyperintensity (yellow arrow), consistent with pachymeningitis, sulcal, with adjacent temporal lobe parenchymal hyperintensity (blue arrow), indicating leptomeningitis and early cerebritis. (C) Axial contrast-enhanced T1-weighted MRI (Figures 1A-1B) demonstrates pachymeningeal (yellow arrows) and leptomeningeal (blue arrows) enhancement over the cerebral hemispheres, indicating pachymeningitis and leptomeningitis.FLAIR MRI, Fluid-Attenuated Inversion Recovery Magnetic Resonance Imaging
On HD 3, the CSF cultures remained negative, but blood cultures from admission grew ampicillin-sensitive S. pyogenes, with susceptibilities as seen in Table 4. The antibiotics were narrowed to intravenous ampicillin 2 g every four hours and acyclovir. Repeat blood cultures were obtained.
On HD 4, CSF herpes simplex virus polymerase chain reaction (HSV PCR), varicella zoster virus polymerase chain reaction (VZV PCR), and enterovirus PCR were all negative, so the acyclovir was stopped. Her mental status improved and she was no longer febrile.
On HD 5, a transesophageal echocardiogram (TEE) to rule out endocarditis showed no evidence of vegetation, and repeat blood cultures from HD 3, at 48 hours, were negative.
In anticipation of discharge, the ampicillin was switched to intravenous ceftriaxone 2 g every 12 hours for the convenience of less frequent dosing, with a plan for a total duration of four weeks of antibiotics from negative blood cultures, due to concern for GAS meningitis/cerebritis based on clinical suspicion and imaging, even though the CSF studies were not suggestive of bacterial meningitis/cerebritis.
Discussion
GAS meningitis has historically been a rare entity in the US [5]. However, in recent years, there has been an upsurge of invasive GAS infections, including meningitis. Denmark and the Netherlands have reported a surge in GAS infections from a specific M1UK lineage of the emm1.0 subtype since 2022 [3,4]. The origin of the M1UK lineage is believed to have arisen as a consequence of the 2008 pharyngitis guidelines in the UK [6]. Over half of the cases between January and March 2023 in the UK were from the emm1.0 strain, with 90% caused by the M1UK variant lineage. In the US, isolates from 122 invasive GAS-reported infections in 2022 were of the emm1.0 subtype [2]. The Centers for Disease Control and Prevention (CDC) data does not specify if these are of the M1UK variant; however, given the global trend, it is a possibility. Our patient could have had the emm1.0 subtype M1UK variant strain, but we were unable to confirm this, given the limited testing availability at our facility.
The dilemma in this case stems from the discordance between the clinical presentation and the microbiological and laboratory data. The evidence supporting meningitis from GAS included the following: (1) the clinical presentation of right-sided otitis media/externa from GAS, which is consistent with previous GAS meningitis infections, where 43% of the cases were preceded by acute otitis media [7]; (2) the MRI shows adjacent right temporal cerebritis, asymmetric leptomeningitis, and pachymeningitis/reactive dural thickening; (3) the presence of invasive GAS infection with bacteremia; and (4) some CSF studies supported bacterial meningitis, including the elevated WBC count with neutrophilic predominance and high protein count.
The evidence that supports the possibility of an alternative cause of meningitis, such as DIAM, included the following: (1) CSF glucose was elevated to 96, while serum glucose levels at the time of lumbar puncture were 128 mg/dL; (2) CSF gram stains showed no organisms, and there was no growth on CSF cultures despite the patient having GAS bacteremia at the same time and intravenous antibiotics being initiated only 30 minutes before the lumbar puncture; and (3) the patient reported consuming a large volume of high-dose ibuprofen prior to admission.
DIAM is a rare cause of meningitis, with fewer than 200 cases reported [8]. Patients usually present with fevers, headaches, meningeal signs, nausea, vomiting, and altered mental status [9]. CSF findings may vary, though they more commonly reveal polymorphonuclear pleocytosis (though lymphocytic and eosinophilic predominance can also be present), variably high protein levels but normal glucose levels, and negative CSF gram stain and cultures [10]. NSAIDs are the most common cause of DIAM, accounting for about 32% of the cases, with ibuprofen being the most common among the NSAIDs [10,11]. There are multiple hypotheses on the mechanisms by which DIAM occurs with different medications. NSAIDs are postulated to combine with a CSF protein, which acts as a hapten, triggering an inflammatory response limited to the meninges [12]. Treatment involves drug cessation, which helps resolve symptoms within 2-14 days [11].
A case report on ibuprofen-induced DIAM noted that rechallenging patients with ibuprofen resulted in generalized malaise, headache, chills, rigors, fevers, and nuchal rigidity within hours. Cessation of the NSAIDs, together with treatment with methylprednisolone and Tylenol, resulted in the resolution of symptoms within 24 hours [13].
In our case, empiric antibiotics were started to cover meningitis, but CSF studies were consistent with aseptic meningitis. Concerned about possible DIAM from ibuprofen ingested by the patient, NSAIDs were avoided throughout the hospitalization. Higher doses of antibiotics were also used, which would cover bacterial infections in the central nervous system. The patient's mental status improved after one week of antibiotics and discontinuation of NSAIDs. Since the interventions were introduced at the same time, the reason for the clinical improvement is difficult to pinpoint. Future use of ibuprofen and meningitis-like symptoms in this patient would confirm that this episode was likely DIAM.
Conclusions
Historically, GAS meningitis has been rare, but there has been a recent surge globally, which is hypothesized to be secondary to the emm1.0 M1UK variant. DIAM can present similarly to bacterial meningitis, especially in patients who have received ibuprofen, which is the most common cause of DIAM. Our case highlights the importance of keeping a broad differential when evaluating patients for meningitis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1History of streptococcal research Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet] Ferretti JJ Köhler W Oklahoma City (OK)University of Oklahoma Health Sciences Center 2016 https://pubmed.ncbi.nlm.nih.gov/26866208/26866208 · pubmed ↗
- 2Centers for disease control and prevention 9 2024 2024 https://www.cdc.gov/abcs/bact-facts/data
- 3Group A Streptococcus meningitis in adults, Denmark Emerg Infect Dis Nielsen H Storgaard M Helweg-Larsen J 193719392920233747828910.3201/eid 2909.230627 PMC 10461673 · doi ↗ · pubmed ↗
- 4Group A Streptococcal meningitis with the M 1UK variant in the Netherlands JAMA van der Putten BC Vlaminckx BJ de Gier B Freudenburg-de Graaf W van Sorge NM 1791179232920233702715010.1001/jama.2023.5927 PMC 10082416 · doi ↗ · pubmed ↗
- 5The epidemiology of invasive group A Streptococcal infection and potential vaccine implications: United States, 2000-2004 Clin Infect Dis O'Loughlin RE Roberson A Cieslak PR 8538624520071780604910.1086/521264 · doi ↗ · pubmed ↗
- 6Rapid expansion and international spread of M 1(UK) in the post-pandemic UK upsurge of Streptococcus pyogenes Nat Commun Vieira A Wan Y Ryan Y 39161520243872992710.1038/s 41467-024-47929-7PMC 11087535 · doi ↗ · pubmed ↗
- 7Group a Streptococcal meningitis in adults: report of 41 cases and a review of the literature Clin Infect Dis van de Beek D de Gans J Spanjaard L Sela S Vermeulen M Dankert J 0634200210.1086/33994111941569 · doi ↗ · pubmed ↗
- 8Dual drug-induced aseptic meningoencephalitis: more than a suggestion SAGE Open Med Case Rep Coletti Moja M Riva G Catalfamo E 211799202110.1177/2050313 X 211021179 PMC 818221434158945 · doi ↗ · pubmed ↗