Efficacy of an Abdominal Surgery Simulator in Didactic Medical Training: A Randomized Controlled Trial
Shea E Fincher, Victoria M Koniuk, Michael S Benavidez, Madison C Benefield, Danielle L Drew, Dean M Hasan, Nicholas Minner, Tara C Prakash, Michael J Parks, Tom Lindsey

TL;DR
A low-cost abdominal surgery simulator was tested in medical training but did not significantly improve exam scores, though it provided valuable learning experiences.
Contribution
A low-cost abdominal surgery simulator was developed and tested for pre-clinical medical education.
Findings
The simulator did not significantly improve post-assessment scores compared to traditional methods.
Students using the simulator gained exposure to surgical and anatomical concepts.
Future plans include integrating the simulator into pre-clinical education and evaluating its impact during surgical rotations.
Abstract
Introduction Many medical students do not have access to hands-on surgical experience throughout the pre-clinical curriculum. To address this issue, we developed a low-cost abdominal surgery simulator for use during instructive years and tested its efficacy through a proof-of-concept, randomized controlled trial. Our goal is to help medical students integrate foundational anatomy with surgical pathology, enhancing their understanding and translating to academic success on board-relevant topics. Methods Second-year students at Edward Via College of Osteopathic Medicine-Carolinas Campus (VCOM-CC) were split into two groups. The control group utilized the traditional curriculum, while the experimental group used the curriculum along with the simulator in instructive and integrative sessions. We created pre- and post-assessments comprised of gastrointestinal anatomy relevant to United…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
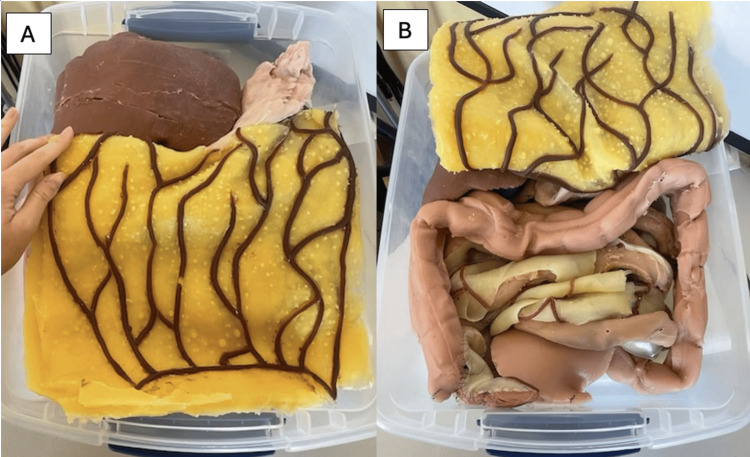 Figure 1
Figure 1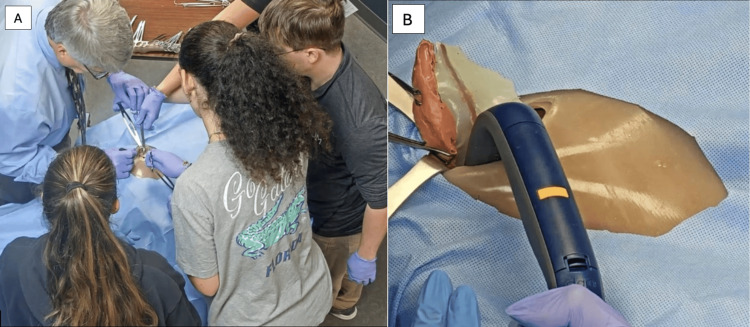 Figure 2
Figure 2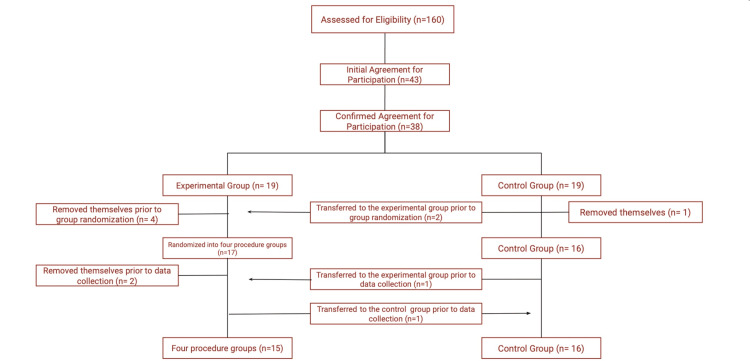 Figure 3
Figure 3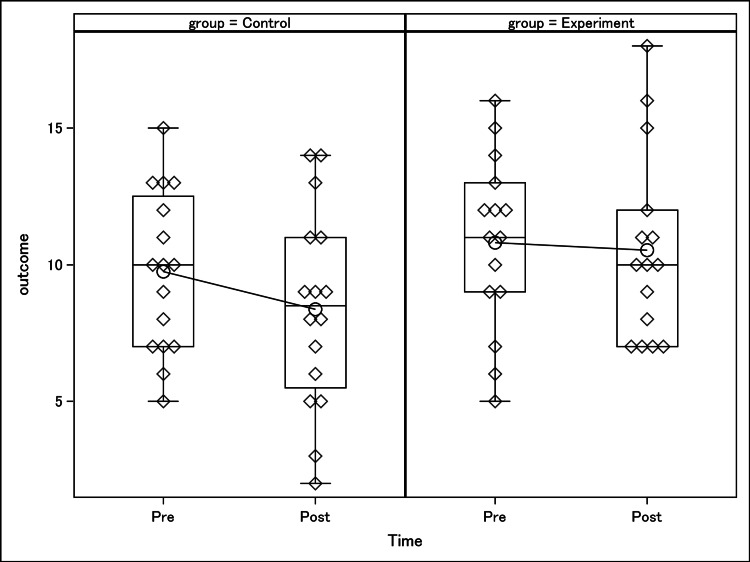 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSimulation-Based Education in Healthcare · Surgical Simulation and Training · Innovations in Medical Education
Introduction
The goal of simulation technology is “to facilitate learning through immersion, reflection, feedback, and practice, minus the risks inherent in a similar real-life experience” [1]. There are few opportunities outside of the operating room that allow for creating a realistic learning environment for medical students in the field of surgery. Simulation learning provides hands-on, focused training, with immediate feedback in a controlled and safe setting [2,3]. A randomized trial conducted in 2014 concluded that first- and second-year residents with access to comprehensive and supervised laparoscopic simulator training significantly improved their cognitive, technical, and non-technical skills compared to their colleagues without such training [4]. This study also suggested that exposure to surgical simulation before residency would enhance pre-clinical medical students’ confidence and learning, thus positively affecting their future surgical rotations [4]. Additional studies have found that technical skills learned in the simulation setting are transferable to clinical practice and provide a superior learning environment for students [5,6]. In 2013, the American College of Surgeons, the Association of Program Directors in Surgery, and the Association for Surgical Education (ACS/APDS/ASE) collectively created a resident preparatory curriculum in response to studies suggesting that first-year residents were not adequately prepared for the tasks and responsibilities of residency [2]. They piloted this curriculum in 49 schools in 2013 and made it available to all schools in 2015 [2]. Today, the ACS/APDS/ASE list of critical content is still used to strengthen the skills of fourth-year medical students entering surgical residencies [7]. As a component of the critical content list, operative anatomy is an element that can be learned most realistically through simulation-based learning during medical school.
Synthetic reality allows a unique and reproducible learning experience in an environment that eliminates potential patient risk. Simulation-based learning also allows students to learn without the distraction of multitasking and feeling overwhelmed. A study in 2009 revealed that interactive learning with simulators enhanced retention by 45% compared to audiovisual learning [8,9]. The shift toward experiential medical training offers students a unique opportunity to learn through various styles. However, high-fidelity simulations, which are computerized and complex configurations of realistic structures, are much more expensive to manufacture. As a result, they are difficult for school systems to acquire and integrate into their curricula [2]. Repetitive practice with simulations is essential for effective skill improvement, and the devices must be accessible during learners’ schedules and available at patient-care facilities and institutions [10]. Therefore, despite advancements in this domain of medical technology, hands-on surgical experience is neither accessible nor available to many medical students receiving didactic education.
To combat this, we created a low-cost abdominal surgery simulator for use during instructional years. By utilizing the simulator, we hope to enhance medical students’ procedural knowledge and success by integrating foundational anatomy with surgical pathology. As the subject of our project, we propose that medical students who use the simulator will gain a better understanding of abdominal anatomy and will demonstrate superior academic performance on assessments and performance during clinical rotations.
Materials and methods
Trial design
To evaluate the effectiveness of an abdominal surgical simulator on medical students' performance in high-yield gastrointestinal (GI) anatomy, we first developed content-based assessments. The assessments were focused on relevant information pertaining to the Comprehensive Osteopathic Medical Licensing Examination (COMLEX) Level 1 and the United States Medical Licensing Examination (USMLE) Step 1 board examinations that Doctor of Osteopathic Medicine (DO) and Doctor of Medicine (MD) medical students, respectively, must pass before entering supervised clinical rotations. This pilot study was a single-center, balanced randomization with 1:1 allocation, parallel-group study conducted on second-year medical students at the Edward Via College of Osteopathic Medicine-Carolinas Campus (VCOM-CC). Before commencing this study, we obtained IRB approval through the VCOM Institutional Review Board (IRB #2023-046), ensuring this study adhered to ethical standards and that participants’ rights were safeguarded throughout the research process.
After trial commencement, the simulation event was rescheduled from March 4, 2024, to April 8, 2024. This change was performed due to scheduling conflicts with the intended study population on the original simulation date. No other changes were made, including the eligibility criteria or trial design.
Participants
This pilot study recruited medical students attending VCOM-CC. The criteria for inclusion were second-year medical students at VCOM-CC in good academic standing. The exclusion criteria included second-year medical students on this research team. All participants were over 18 years of age. To recruit participants, a clinical faculty member sent a recruitment email to the target study population, second-year medical students at VCOM-CC. The recruitment email described the study’s purpose, expected time commitment, and study logistics. Students interested in joining the study entered their name and professional email into the attached interest form. Once the interest form was closed, a study investigator sent an informed consent form to students who responded. The informed consent form was approved by the VCOM IRB and delineated the research, the study’s purpose, and the risks and benefits of participating. Additional verbal consent was obtained on-site for participants engaging in the simulation event.
The intended sample size for the study was 50 second-year VCOM-CC medical students. The study was available to all 160 students in the VCOM second-year class, in which 43 students initially joined the study and 31 continued participation throughout the study. The minimum number of students for the study was eight, allowing for one student per experimental group module and the remaining four students in the control group. No interim analyses were performed during this project. The project was run continuously, and there were no stopping points.
Interventions
Simulator Development
In this project, we developed a low-cost abdominal surgery simulator using Smooth-On silicone materials and 3D-printed organ models to simulate surgical training during clinical years. The final simulator, shown in Figure 1 without the skin overlay, included all pertinent abdominal cavity anatomy to perform multiple open abdominal surgeries. Structures between the diaphragm and pelvic region were represented to focus on abdominal cavity anatomy. The simulator included structures from the GI system, which began cephalically at the stomach, the female genitourinary system, and the female reproductive system. Detailed structural relationships such as the portal triad and biliary system, the ligaments supporting the uterus, and key abdominal vasculature highlighted the anatomical knowledge necessary to perform abdominal surgeries. Pertinent tissues notable in the abdominal cavity were also exhibited, such as the parietal peritoneum surrounding the entire cavity, the greater omentum, and the mesentery. The total material cost was $2,753.47, excluding the price of the 3D printer owned by the institution. Therefore, the cost-effectiveness of our fully functional abdominal surgical simulator helps to address the increasing need for low-cost real-tissue training devices. To maintain continuity and optimize functionality, the team returned the simulator to its original state before each simulated surgical case. These procedures were guided by a board-certified general surgeon in a simulated operating room.
Final simulator without the parietal peritoneum and skin overlay. The simulator with organs and omental layer as positioned for each procedure (A), and the omental layer folded superiorly to showcase the intestines (B). A silicone layer to represent the parietal peritoneum was placed directly over the pictured structures and within the lateral edges of the bin holding the simulator organs. Then, the muscle, subdermal fat, and skin layers, represented by one multitiered silicone surface, were placed over the parietal peritoneal layer and secured along the outside of the simulator bin with Velcro for the procedures.
Assessment Creation
During this study, participants completed a pre-assessment and post-assessment, each consisting of 20 multiple-choice board-relevant GI anatomy questions based on tested content on the COMLEX-USA Level 1 and USMLE Step 1 board examinations. Members of the research team created board-style questions for these assessments by referring to the VCOM-CC GI Anatomy Exam One curriculum objectives provided by the school. The objectives reflect anatomical topics tested on medical school and medical licensing examinations and correlate to structures displayed in the simulator. Researchers used this information to deduce which pertinent objectives about surgical anatomy exhibited weaker class performance. Two questions were generated for each pertinent objective and were randomly distributed between the two assessments. Therefore, the assessments exemplified similar board-relevant information and quantity of topics. The assessments also adequately reflected material examined in medical school curricula and medical licensing examinations without being identical.
Assessments were sent via email as a Google Forms link (Google, Mountain View, CA, US). To submit Google Forms, participants were required to complete every question on the assessment. Participants were not shown their performance upon completion of the assessment. These assessments were held to VCOM Honor Code standards, therefore not tolerating any outside resources or collaboration among students. The first question of the pre-assessment prompted the participants to create a self-generated identification code (SGIC), which was also input into the post-assessment. Therefore, assessments were matched to each participant, providing anonymous longitudinal data collection in the study.
Module Creation
Learning modules dedicated to each procedure were presented to participants before performing the specific simulated procedure. The research team curated these learning modules on Google Slides (Google, Mountain View, CA, US) following a case-presentation format. Each module presented pertinent information, such as the History of Present Illness, a Review of Symptoms, Vitals, Physical Exam, Laboratory Values, Imaging, Differential Diagnosis, and Plan. The Plan section of each module included a short video illustrating the procedure, found on free resources such as YouTube (https://www.youtube.com). Each module also included high-yield clinical and anatomical quick facts surrounding the topic discussed. Board-relevant information was found through medical school curriculum resources such as Boards&Beyond and the First Aid for the USMLE Step 1 2023 book from McGraw Hill, UWorld Step 1 Question Bank from UWorld LLC, and VCOM lecture material. The principal investigator presented each 10-minute module immediately before the specific procedure.
Procedures
The trial included an integrative simulation event hosted at the VCOM-CC on April 8, 2024, from 1:00 pm to 5:00 pm. Participants randomly assigned to the experimental group attended this simulation event, with 15 participants in attendance. During the event, the experimental group engaged in an interactive case-based module guided by the principal investigator before each simulated surgical experience. The simulation involved four procedures using the same simulator: appendectomy, cholecystectomy, periumbilical exploratory small bowel obstruction, and hysterectomy with the Pfannenstiel incision. Participants were randomly assigned to one of these procedure groups. Each group performed their assigned procedure under the guidance of the principal investigator, a board-certified general surgeon. The simulation lab was configured to mimic an operating room environment. Participants not actively involved in the procedure synchronously observed the instruction and performance of the procedure via a live-stream video in a separate conference room. Figure 2 shows the appendectomy performed on the simulator and the live-stream shown to participants during the simulation event. Following the simulation event, the experimental group conducted a focus group discussion. This session aimed to gather immediate feedback to minimize recall bias and incorporated subjective questions to gain further insight into the students’ thought processes throughout the simulation event.
Simulated appendectomy. Performance of the procedure by the principal investigator and assigned participants in the experimental group (A). A still photograph of the live-stream projection of the appendectomy, showcasing the removal of the appendix, mesoappendix, and appendicular artery from the simulator (B).
Data collection
Data from the pre-assessment and post-assessment were collected using Google Forms links. Scores were calculated by totaling correct responses out of 20 questions. Participants were given one full day to complete each assessment. Data for the pre-assessment were collected from April 7, 2024, at 8:00 am until April 8, 2024, at 12:00 pm. The data for the post-assessment were collected from April 8, 2024, at the conclusion of the simulation event until April 9, 2024, at 5:00 pm. Each participant’s pre-assessment and post-assessment scores were labeled next to their SGIC on a Microsoft Excel sheet (Microsoft Corp., Redmond, WA). Data was only accessible to research team members.
During study development, there were no confounding variables or effect modifiers identified. This study’s design included only two variables: the independent variable, assessment scores, and the dependent variable, exposure to a surgical simulator, precluding the presence of additional variables that could serve as confounders or effect modifiers. Any potential confounding effects on the results were successfully addressed by maintaining consistent difficulty levels between the pre- and post-assessments.
Outcomes
The primary outcome of this study was the average change in scores between the pre- and post-assessment among the two groups. Analysis of collected outcomes began after completion of the post-assessment at 5:00 pm on April 9, 2024. A statistician acquired through VCOM-CC analyzed the data. There were no changes in data collection or analysis of outcomes after commencement, and outcomes remained the same throughout the study.
Randomization
Randomization of the two groups was accomplished using randomization functions in Microsoft Excel. This pilot study used simple randomization based on a 1:1 allocation ratio. Once participants were assigned to the experimental or control group, the experimental group was randomized into four equal blocks. After randomization, group designation was disclosed to participants via email, and participants allocated to the experimental group were invited to attend the simulation event. Study investigators were not blinded to group assignments.
Blinding
This study was not blinded. Participants in the experimental group were notified of their placement to attend the simulation event. Additionally, procedure assignments were revealed to participants during the simulation event. Objective outcomes were used in the study to decrease the risk of bias. Standardization occurred across all four procedural groups to ensure equal exposure to the pre-procedure modules, simulator, and procedures. All participants were presented with the same procedure-centered modules and instructed by the same principal investigator throughout the session. Each procedure was projected live into the main seminar room to ensure participants who were not physically present during the procedure were exposed to the same instruction and direct view of the procedure. Limitations of this standardization include the four procedures being inherently different. Therefore, each procedure group physically utilized the simulator for separate procedures and ultimately had a different experience with the simulator.
Statistical analysis
Analyses began by summarizing the data with counts, sample means, and standard deviations. Given the pre-post nature of the study, we calculated a change score by calculating the difference between post-outcome values and pre-outcome values. We then tested to see if the average change observed per person could be declared statistically significant. We used a two-sample t-test for this hypothesis test using a Type I error rate of 0.05. All statistics and significance tests were calculated/performed using SAS 9.4 (SAS Inc., Cary, NC, US). There were no subgroup analyses or adjusted analyses performed on this data.
Results
Participant flow
Initially, 43 students filled out the interest form, but five withdrew from the study before the randomization process. This left 38 participants, who were randomly assigned to either the experimental or the control group. Ultimately, only 31 participants remained: 15 in the experimental group and 16 in the control group. Of the 19 assigned to the experimental group, 12 attended the simulation event. Six participants withdrew from this group before data collection-four left before the groups were divided, and two left after. Additionally, one participant who was originally in the experimental group did not attend the simulation but completed both assessments, so they were moved to the control group. In the control group, one participant left before data collection. To ensure the groups were similar in size, three individuals from the control group were randomly selected to join the experimental group. A diagram illustrating these changes is presented in Figure 3. Participants left the study as previously described because of scheduling conflicts.
Diagram representing participant flow during randomization. Participant eligibility, participation, and removal from this trial occurred as shown in the figure. A total of six participants removed themselves from the experimental group, and one was transferred to the control group. A total of one participant removed himself/herself from the control group, and three were transferred to the experimental group. Final participation consisted of an experimental group of 15 participants and a control group of 16 participants.
Baseline data
Baseline demographics in the control and experimental groups were similar, with each group comprising 66.7% women and 33.3% men, and all participants were above 18 years old. Due to all participants following the same medical school curriculum, they had previous exposure to simulation-based learning experiences such as cardiac arrest, labor and delivery, and newborn evaluations. None of the students had exposure to surgical-based simulation through their medical school curriculum. Lastly, all students had relevant anatomy exposure by completing the school’s gross anatomy and didactic anatomy courses during academic pre-clinical training.
Outcomes and estimation
There were 16 individuals in the control group and 15 in the experimental group. For the control group, the average pre-intervention outcome was 9.75, with a standard deviation of 2.93, while the average post-intervention outcome was 8.375, with a standard deviation of 3.65 (Figure 4). Calculating the average change score for the control group revealed an average change of -1.375 and a standard deviation of 2.93. For the experimental group, the average outcome at pre-intervention was 10.80 with a standard deviation of 2.93, while at post-intervention, the average outcome was 10.533, with a standard deviation of 3.46 (Figure 4). Calculating the average change score for the experimental group revealed an average change of -0.267 and a standard deviation of 3.90. A two-sample t-test testing for a difference between groups in average change produced a p-value of 0.3246. Based on the p-value, we conclude there is not sufficient evidence with a two-tailed Type I error rate of 0.05 to conclude the average change differs between groups.
This graph compares the mean test scores between pre-simulation and post-simulation assessments between the control group and the experimental group. A two-sample t-test testing for the difference between groups in average change produced a p-value of 0.3246. Based on the p-value, we conclude there is not sufficient evidence with a two-tailed Type I error rate of 0.05 to conclude the average change differs between groups.
Ancillary analyses
There were no additional analyses performed.
Adverse events
The study involved no harm or unintended effects from participation.
Discussion
The purpose of this study was to evaluate the effectiveness of an open surgical simulation experience by analyzing the average change in performance on pre- and post-assessments between two groups. Assessments used in this study were built to determine participants' understanding of board-relevant abdominal anatomical concepts. This simulation aimed to replicate a real-life operative room experience for exposure to applicable abdominal structures and relationships as examined throughout undergraduate medical curricula. Through this randomized controlled trial, participants who engaged in the scenario-based training did not demonstrate a difference in average score change between assessments compared to traditional training methods. Both groups showed a decrease in average scores from pre- to post-assessment. However, the experimental group, which participated in the integrated simulation event, experienced a smaller decline in average scores than the control group. These results imply that simulation may effectively improve comprehension and performance on knowledge-based material.
This trial analyzed simulator efficacy for improving academic performance on assessments in contrast to recent studies examining simulator effectiveness on clinical competency, reasoning, and skill. A comprehensive narrative review conducted in 2023 focused on the use of surgical simulation for developing skills and preparing surgery residents for real-life scenarios concluding their usefulness in these competencies [11]. Additional literature published in 2010 surveyed the preferences of internal medicine residents regarding the content, features, and learning experience of simulators [12]. Survey responses also indicated that simulator and instructor-integrated learning subjectively improved clinical techniques, understanding of equipment, and troubleshooting [12]. This survey poses a significant challenge to the objectives of this study, which hypothesized that working with the simulator would improve understanding of knowledge-based components during didactic years. Though this study did not prove statistical significance in the parameter of analysis chosen, it may demonstrate benefit in improving medical student confidence and perceived preparation for post-didactic surgical clinical rotations.
The aforementioned comprehensive narrative review conducted in 2023 primarily involved the use of simulation training during surgical graduate medical education [11]. In contrast, this trial implemented simulation exposure to medical students during their pre-clinical undergraduate medical education. While there is no existing literature indicating that specific demographics will benefit more from simulation training than others, the applicability of the conclusions drawn from this research may not be generalizable to populations with differing knowledge bases and clinical backgrounds.
In June 2024, a comprehensive literature review was performed to determine the impact of simulation-based training (SBT) during medical education [13]. This literature review is comparable in the demographic focus and intended purpose of this study and similarly used parameters of clinical proficiency to analyze the impact of SBT in medical education [13]. Additionally, this review noted that comprehensive post-simulation debriefing sessions, involving targeted feedback on performance, potential mistakes, and areas of improvement, were critical to reinforce learning and correct errors in simulated experiences [13]. Though this trial did feature a post-simulation debrief, the gathering did not provide formal feedback on performance to reinforce learning for the participants. As simulator uses described in this review were similar to this study, implementing a thorough post-simulation discussion would help foster reflective practice and contribute to individual and team development.
The operative simulation experience of this study was organized into small procedure group sizes, providing participants with direct instruction and visualization of anatomical structures. A survey of internal medicine residents on preferences for simulation experiences described an ideal teacher-learner ratio of 1:4 for active engagement and immediate feedback during simulation exercises [12]. This preference aligns with the small group format used in this trial, further supporting the value of the aforementioned operative simulator experience.
Additional pilot studies with a design similar to ours, incorporating both simulation and training modules, demonstrated that students who engaged with both components improved their technical skills and overall surgical performance [14]. The training modules used in this trial provided an overview of surgical techniques and a detailed anatomical and pathophysiological understanding of the diseases represented in the simulator. Furthermore, the training modules in this study were strategically built to address content focused on the study's pre- and post-assessments and high-yield content for board licensing examinations. In contrast, effectiveness in other published trials underscored the importance of surgical proficiency and skill, focusing their training modules on these specific areas [14].
Overall, this study stands out from other studies of similar caliber by concentrating on parameters of effectiveness related to academic performance combined with practical surgical experience. These differences highlight the need for further investigation into the utility of simulated operative experience for a better understanding of operative anatomical concepts in pre-clinical medical education.
Limitations
One significant limitation of this study is its small sample size, which affects its internal and external validity, making it difficult to generalize the findings. The limited sample size was primarily due to the time commitment required for the complete simulation experience. The experimental group had to commit to a four-hour simulation experience, which likely deterred potential participants from joining and remaining in the study. In future studies, we aim to increase the sample size by scheduling the simulation event at a convenient time for the students. The simulation event in this study took place while second-year medical students were preparing for board examinations. Consulting students to determine the best time to hold the simulation could optimize the event timing and minimize scheduling conflicts. Overall, acquiring a larger sample size would greatly increase the power of the study.
Another limitation of this simulation-based research study is the limited applicability of simulated procedures to real-life operating room situations. Simulation-based learning has constraints in transferring to real-world scenarios, as it is a controlled environment, posing a challenge for learners to apply the skills learned in simulation to their workplace. In addition, we recognize the cost of obtaining and adequately compensating faculty for these purposes may limit the study's reproducibility. A final limitation lies in the simulator’s functionality, as its failure during a simulation event could significantly impact the study. Due to the nature of the simulator, it is challenging to control for inherent limitations in this study design. Future studies may incorporate standardization protocols to minimize the risk of simulation malfunction.
Generalizability
The generalizability of this pilot randomized controlled study is limited due to its relatively small sample size. The small sample size also affects the study’s internal and external validity. In addition, the four procedures varied between each group in our experimental group, leading to inevitable differences in instruction. To address this, we live-streamed each procedure, so each participant in the experimental group listened to and watched all four procedures in real time with the same instruction.
Conclusions
The results did not show a statistically significant average change in test scores between pre- and post-assessments among controls versus experimental groups; however, they demonstrate a subjective benefit in boosting confidence and knowledge through risk-free and hands-on experience. To fully leverage the benefits of simulation training, more research should be dedicated to integrating simulation into the curriculum to maximize its advantages. This research project contributes valid data in support of simulation training for medical education by suggesting long-term benefits despite a lack of measurable immediate improvements in learning outcomes. To better understand how different training methods affect clinical outcomes, we hope to continue exploring the role of surgical simulation in enhancing medical students' practical skills. A future key research goal is to examine how exposure to surgical simulations influences medical students' performance in clinical surgical rotations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Simulation and its role in medical education Med J Armed Forces India Datta R Upadhyay K Jaideep C 1671726820122462393210.1016/S 0377-1237(12)60040-9PMC 3862660 · doi ↗ · pubmed ↗
- 2The evolving role of simulation in teaching surgery in undergraduate medical education Surg Clin North Am Acton RD 7397509520152621096710.1016/j.suc.2015.04.001 · doi ↗ · pubmed ↗
- 3The changing face of surgical education: simulation as the new paradigm J Surg Res Scott DJ Cendan JC Pugh CM Minter RM Dunnington GL Kozar RA 18919314720081849886810.1016/j.jss.2008.02.014PMC 2676783 · doi ↗ · pubmed ↗
- 4Introduction of a comprehensive training curriculum in laparoscopic surgery for medical students: a randomized trial Surgery Gawad N Zevin B Bonrath EM Dedy NJ Louridas M Grantcharov TP 69870615620142490934810.1016/j.surg.2014.04.046 · doi ↗ · pubmed ↗
- 5The pelvitrainer for training in laparoscopic surgery-a prospective, multicenter, interdisciplinary study: Experimental research Int J Surg Ackermann J Pahls J Baumann J 10660410120223539852910.1016/j.ijsu.2022.106604 · doi ↗ · pubmed ↗
- 6Starting a simulation and skills laboratory: what do I need and what do I want?J Surg Educ Friedell ML 1121216720102065660910.1016/j.jsurg.2010.03.001 · doi ↗ · pubmed ↗
- 7Statement on surgical preresidency preparatory courses J Surg Educ American Board of Surgery; American College of Surgeons; Association of Program Directors in Surgery; Association for Surgical Education 7777787120142543396110.1016/j.jsurg.2014.05.010 · doi ↗ · pubmed ↗
- 8The use of simulation in medical education to enhance students' understanding of basic sciences Med Teach Rosen KR Mc Bride JM Drake RL 8428463120091981119010.1080/01421590903049822 · doi ↗ · pubmed ↗