The 50 most cited studies on trochleoplasty
Alexander Pfarrmaier, Romed P. Vieider, Rodrigo Sanchez, Lukas N. Muench, Lukas Willinger, Sebastian Siebenlist, Armin Runer

TL;DR
This paper reviews the 50 most cited studies on trochleoplasty, analyzing their quality and citation patterns to assess the field's research trends and gaps.
Contribution
The study provides a comprehensive analysis of the most influential trochleoplasty research, highlighting methodological quality and citation trends.
Findings
Most studies were case series or systematic reviews with low levels of evidence.
High citation counts did not correlate with higher methodological quality scores.
European institutions, especially France and Switzerland, dominated the research output.
Abstract
This study aimed to analyse the 50 most cited publications on trochleoplasty (TP), examine their bibliographic parameters and evaluate the correlations between citation count, methodological quality and other factors. In a comprehensive literature search on the Web of Science, the 50 most cited studies on TP were identified. These studies were then evaluated according to their bibliographic parameters, level of evidence (LOE), citation counts, the Modified Coleman Methodological Score (MCMS), the Methodological Index for Non‑Randomised Studies (MINORS) and the Radiologic Methodology and Quality Scale (MQCSRE). Of the top 50 list, 15 articles (30%) were published in the journal ‘Knee Surgery Sports Traumatology Arthroscopy’ (KSSTA). A total of 39 studies were published by institutes from Europe (78%), with France and Switzerland being represented 10 times each. Of eight different study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
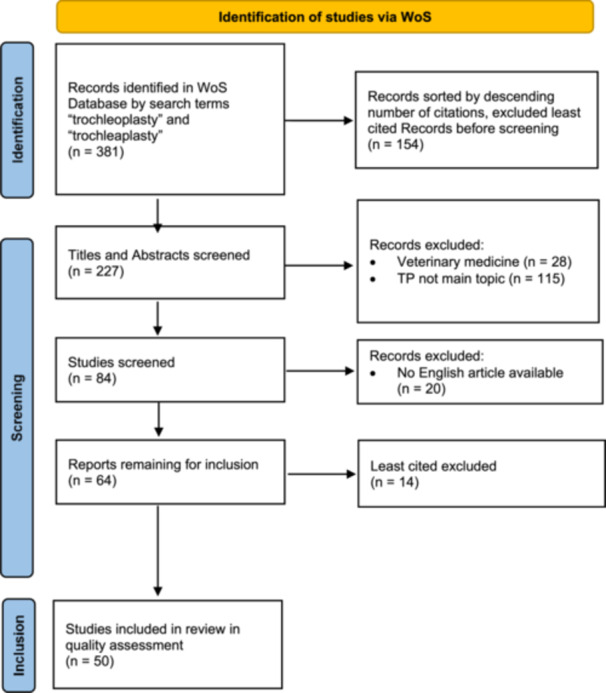 Figure 1
Figure 1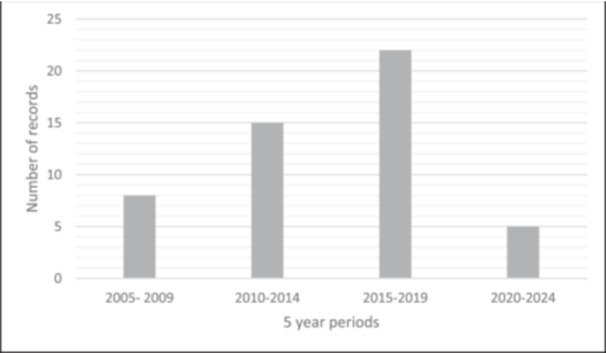 Figure 2
Figure 2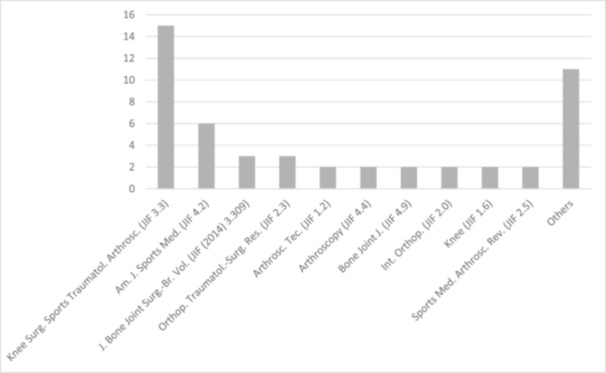 Figure 3
Figure 3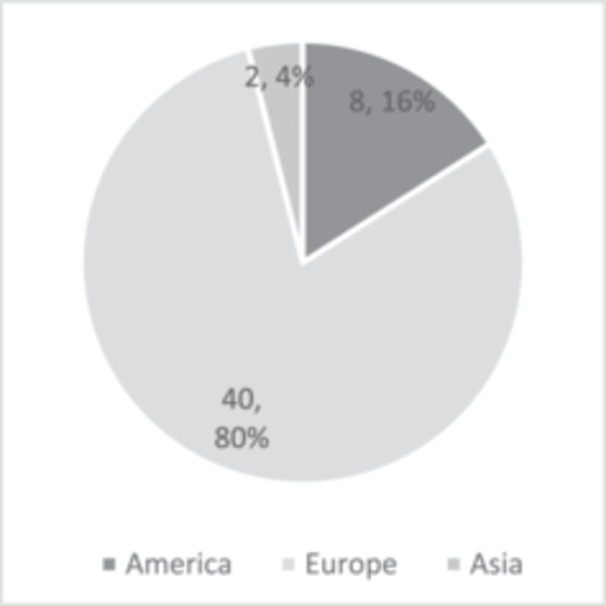 Figure 4
Figure 4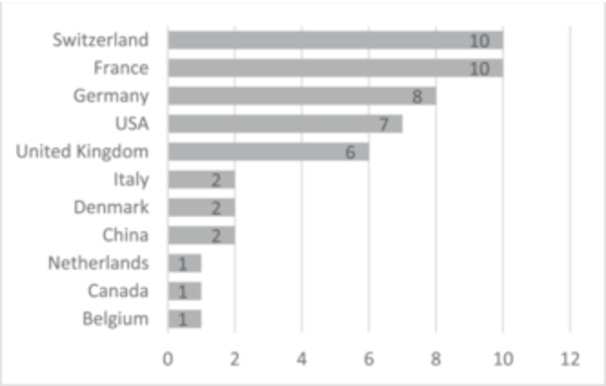 Figure 5
Figure 5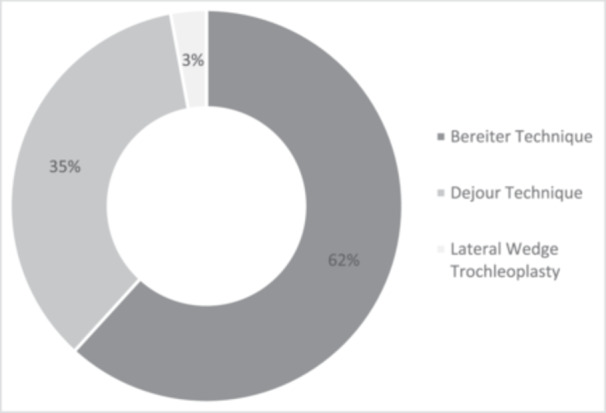 Figure 6
Figure 6| Rank (citations) |
Authors | Year | Study design | LOE | MINORS | MCMS | MQCSRE |
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1 (187) |
| 2010 | Surgical technique | 5 | N/A | N/A | N/A |
| 2 (169) |
| 2006 | Case series | 4 | 8 | 61 | 23 |
| 3 (134) |
| 2005 | Case series | 4 | 10 | 60 | 22 |
| 4 (127) |
| 2005 | Case series | 4 | 8 | 67 | N/A |
| 5 (110) |
| 2006 | Case series | 4 | 12 | 69 | 24 |
| 6 (101) |
| 2008 | Biomechanical study | 5 | N/A | N/A | N/A |
| 7 (100) |
| 2008 | Case series | 4 | 9 | 60 | 23 |
|
|
| 2013 | Case series | 4 | 10 | 49 | 20 |
| 9 (92) |
| 2013 | Case series | 4 | 12 | 69 | 24 |
| 10 (75) |
| 2014 | Case series | 4 | 12 | 59 | 23 |
| 11 (73) |
| 2011 | Case series | 4 | 11 | 81 | 24 |
| 12 (72) |
| 2017 | Systematic review and meta‐analysis | 4 | N/A | N/A | N/A |
| 13 (61) |
| 2007 | Case series | 4 | 8 | 39 | 15 |
| 14 (58) |
| 2015 | Case series | 4 | 12 | 50 | 23 |
| 15 (58) |
| 2013 | Case series | 4 | 10 | 52 | 21 |
| 16 (56) |
| 2014 | Case series | 4 | 13 | 64 | 22 |
| 17 (53) |
| 2017 | Review | 4 | N/A | N/A | N/A |
| 18 (48) |
| 2016 | Case series | 4 | 11 | 75 | 23 |
| 19 (46) |
| 2018 | Review | 4 | N/A | N/A | N/A |
| 20 (46) |
| 2014 | Review | 4 | N/A | N/A | N/A |
| 21 (46) |
| 2007 | Histological examination | 5 | N/A | N/A | N/A |
| 22 (43) |
| 2014 | Review | 4 | N/A | N/A | N/A |
| 23 (42) |
| 2010 | Case series | 4 | 9 | 69 | 24 |
| 24 (39) |
| 2014 | Review | 4 | N/A | N/A | N/A |
| 25 (38) |
| 2018 | Review | 4 | N/A | N/A | N/A |
| 26 (37) |
| 2019 | Review | 4 | N/A | N/A | N/A |
| 27 (37) |
| 2015 | Case series | 4 | 11 | 73 | 24 |
| 28 (36) |
| 2017 | Case series | 4 | 11 | 69 | 23 |
| 29 (35) |
| 2019 | Systematic review and meta‐analysis | 4 | N/A | N/A | N/A |
| 30 (34) |
| 2012 | Review | 4 | N/A | N/A | N/A |
| 31 (28) |
| 2018 | Review | 4 | N/A | N/A | N/A |
| 32 (28) |
| 2018 | Systematic review and meta‐analysis | 4 | N/A | N/A | N/A |
| 33 (25) |
| 2019 | Review | 4 | N/A | N/A | N/A |
| 34 (23) |
| 2019 | Prospective cohort study | 3 | 22 | 52 | 23 |
| 35 (20) |
| 2018 | Case series | 4 | 14 | 61 | 23 |
| 36 (18) |
| 2018 | Surgical technique | 5 | N/A | N/A | N/A |
| 37 (17) |
| 2016 | Case series | 4 | 8 | 57 | 23 |
| 38 (16) |
| 2022 | Surgical technique | 5 | N/A | N/A | N/A |
| 39 (16) |
| 2020 | Case series | 4 | 9 | 56 | 24 |
| 40 (15) |
| 2021 | Systematic review and meta‐analysis | 4 | N/A | N/A | N/A |
| 41 (15) |
| 2020 | Case series | 4 | 12 | 70 | 22 |
| 42 (15) |
| 2017 | Review | 4 | N/A | N/A | N/A |
| 43 (15) |
| 2017 | Case series | 4 | 10 | 54 | 19 |
| 44 (15) |
| 2012 | Review | 4 | N/A | N/A | N/A |
| 45 (14) |
| 2017 | Case series | 4 | 12 | 45 | 26 |
| 46 (12) |
| 2019 | Surgical technique | 5 | N/A | N/A | N/A |
| 47 (12) |
| 2010 | Case series | 4 | 10 | 56 | 23 |
| 48 (11) |
| 2017 | Case series | 4 | 15 | 63 | 22 |
| 49 (10) |
| 2021 | Biomechanical study | 5 | N/A | N/A | N/A |
| 50 (10) |
| 2011 | Case report | 5 | N/A | N/A | N/A |
| Decade of publication | 2000–2009 | 2010–2019 | 2020–2024 |
|---|---|---|---|
| MCMS | 59.33 ± 10.67 | 61.00 ± 10.06 | 63.00 ± 9.90 |
| MINORS | 9.17 ± 1.60 | 11.83 ± 3.05 | 10.50 ± 2.12 |
| MQCSRE | 21.40 ± 3.64 | 22.78 ± 1.59 | 23.00 ± 1.41 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLower Extremity Biomechanics and Pathologies · Sports injuries and prevention · Foot and Ankle Surgery
INTRODUCTION
Patellofemoral instability (PFI) is a pathology of multifactorial origin that can be caused by congenital or post‐traumatic anatomical and neuromuscular alterations [18]. It accounts for 2‐3% of all knee injuries, with an estimated incidence of 23.2/100.000 persons/year. The latter is highly age‐dependent, being 147.7/100.00 persons/year at 14‐18 years in comparison to 3.1/100.000 persons/year at ≥46 years [8, 22, 25].
Predictive factors for chronic PFI are trochlear dysplasia (TD), patella alta, TT‐TG > 20 mm, external tibial torsion, soft tissue hyperlaxity, malalignment, femoral anteversion, history of subluxation and an early onset of first patellar dislocation. Of these risk factors, TD is one of the most influential, with a hazard ratio of 18.5–23.7 [8, 18, 21, 22].
Dejour et al. [7] highlighted the critical role of TD as a significant predisposing factor in the pathogenesis of PFI, demonstrating that 96% of patients presenting with patellofemoral dislocation exhibited this anatomical abnormality. The surgical treatment of severe TD is often approached by performing a trochleoplasty (TP) with the primary goal to adjust the shape and depth of the trochlea in order to prevent patellar instability [25]. While the number of publications pertaining to TP for the treatment of PFI is increasing, a review evaluating the most impactful studies is useful to serve as a reference tool on this specific topic.
The aim of the present study was (1) to identify the 50 most cited studies on the topic of TP along with their bibliographic parameters and (2) to determine whether different factors, such as level of evidence (LOE), methodological quality, country of origin, journal of publication and different surgical techniques correlated with the citation count and citation density in the top 50 most cited studies.
MATERIALS AND METHODS
Literature search
A search of the Thomson Reuters Web of Science (WoS) database was conducted on 2 August 2024 to extract all available literature using the keywords ‘trochleoplasty’ and ‘trochleaplasty’ in the search category ‘topic’. WoS is a Clarivate™ platform that provides access to over 225 million records (as of May 2024), spanning more than 34,000 journals, books, proceedings, patents and data sets, covering a period from 1800 to the present day [1]. The WoS search yielded 381 records, published between 1970 and 2024, whose titles and/or abstracts included the terms ‘trochleoplasty’ or ‘trochleaplasty’. These records were compiled into a data sheet containing their title, author names, year of publication, journal, abstract, language and total citations (across all databases), then sorted by descending citation count. A similar search was performed using Elsevier's Scopus database for the terms ‘trochleoplasty’ and ‘trochleaplasty’ but since the results almost perfectly matched those from WoS, the ranking was based solely on the citation counts extracted from the WoS database.
Inclusion and exclusion criteria
Of the initial list of 381 extracted records, the 154 least cited studies were excluded to focus on the most relevant research for the top 50. The titles and abstracts of the remaining 175 studies were then systematically screened, starting with the most cited. Studies were included if they met the following criteria: (1) TP as the primary topic, (2) TP performed specifically for the treatment of PFI and (3) not an animal or veterinary study. This selection process ensured that only the most relevant and impactful studies were considered for the final ranking.
This process yielded 84 articles, which were further screened. Subsequently, 20 records were excluded due to the absence of English versions. Of the remaining 64 articles, the 50 most cited were selected for final analysis (Figure 1).
PRISMA flow diagram of the selection process of included records [16]. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta‐Analyses; Wos, Web of Science.
Data assessment
The included studies were evaluated based on the following criteria: first author, journal, 2023 Journal Impact Factor (JIF), Journal Citation Indicator (JCI), total citation count, study type, country of origin and year of publication. To ensure comparability between older studies, which typically accumulate more citations, and more recent articles, citation density (total citations divided by years since publication) was calculated.
Quality assessment included the LOE according to the Journal of Bone and Joint Surgery [24], the Modified Coleman Methodology Score (MCMS) [4], Methodological Index for Non‐Randomised Studies (MINORS) [20] and Radiologic Methodology and Quality Scale (MQCSRE) [2]. Interrater reliability was calculated for each score. The MCSM is a dependable tool to assess clinical studies, emphasising factors such as population size, follow‐up rates, diagnostic evaluations and rehabilitation protocols [4]. The MINORS score was created to quantify the methodological quality of observational studies, especially within the surgical fields [20]. As the main diagnostic tool for TD are radiological, such as common x‐rays, computed tomography (CT) or magnetic resonance imaging (MRI), the studies were also evaluated using the methodological quality scale designed for clinical studies involving radiologic examinations (MQCSRE) [2].
Systematic reviews (SRs), surgical techniques, cadaveric or biomechanical studies and histological examinations were not assessed, as the chosen scores were not developed for these types of studies.
Statistical analysis
Descriptive statistics were calculated using SPSS (IBM, Version 27) and displayed by graphs and tables. The normal distribution of the variables was tested using the Kolmogorov–Smirnov test, which concluded that the different variables were not normally distributed. In cases where several groups were compared, the Kruskal–Wallis test was used, and in all other cases, the Mann–Whitney U test was used to compare single groups. A value of p < 0.05 was defined as statistically significant. The LOE and Quality scores (MCMS, MINORS and MQCSRE) were determined by independent raters and subsequently assessed using Pearson's correlation coefficient. Cohen's kappa (κ) was used to determine the agreement between the raters (κ < 0: no agreement; 0–0.20 slight, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 substantial and 0.81–1 almost perfect agreement [10]).
RESULTS
Descriptive statistics
The collective citation count of the top 50 most cited studies on TP resulted in 1870 citations, averaging 37.4 ± 34.2 citations per article (Table 1). The studies were published between 2005 and 2022, with the majority (n = 37; 74%) published between 2010 and 2019. For a more detailed evaluation and better illustration, 5‐year periods were analysed, showing almost half of the articles (n = 22) published between 2015 and 2019 (Figure 2).
Absolute number of publications per 5‐year period.
The top 50 most cited articles were published in 21 journals. In total, 15 articles (30%) were published in the journal ‘Knee Surgery Sports Traumatology Arthroscopy’ (KSSTA), followed by 6 articles (12%) published in the ‘American Journal of Sports Medicine’ (Figure 3). The Bone & Joint Journal is the highest‐ranked journal, considering its JIF of 4.9 and JCI of 2.15. KSSTA ranks fifth with a JIF of 3.3 and a JCI of 1.47, while AJSM is ranked fourth by JIF (4.2) and third by JCI (1.83). The mean JIF was 3.0 ± 1.2, with 58% of the studies published in a journal with a JIF of 3.3 or higher. The mean JCI was 1.30 ± 0.56.
Distribution of the top 50 studies by the journals of publication and their Journal Impact Factor of 2021 (JIF). Knee Surgery, Sports Traumatology, Arthroscopy (Knee Surg Sports Traumatol Arthrosc), American Journal of Sports Medicine (Am J Sports Med), Journal of Bone and Joint Surgery, British Volume (J Bone Joint Surg Br), Orthopaedics & Traumatology: Surgery & Research (Orthop. Traumatol‐Surg. Res.), Arthroscopy Techniques (Arthrosc. Tec.), Arthroscopy (Arthroscopy), The Bone & Joint Journal (Bone Joint J), International Orthopaedics (Int. Orthop), Knee (Knee), Sports Medicine and Arthroscopy Review (Sports Med. Arthrosc. Rev.).
The majority of studies were published by European institutions (n = 40; 80%) (Figure 4), with France and Switzerland contributing 10 publications each, followed by Germany (n = 8) and the United Kingdom (n = 6) (Figure 5). Seven publications (14%) originated from institutions in the United States (US), and one (2%) was published by a Canadian institution. Notably, between 2000 and 2009, no studies from the US or Canada appeared in the top 50. However, between 2010 and 2019, 18.9% (n = 7) of the top studies were conducted in North America, and from 2020 to 2024, 20% (n = 1) were published by American institutions. This reflects a modest increase in North American contributions, though the change did not reach statistical significance (p > 0.05).
Continents and countries of main research conducting institute.
Continents and countries of main research conducting institute.
Case series (n = 25; 50%) and SRs and meta‐analyses (n = 16; 32%) represented the most prevalent study designs. The majority of articles were classified as LOE IV (n = 41; 82%). A comparison of LOE across the last three decades revealed no statistically significant differences (p > 0.05). Notably, there were no studies with a LOE higher than III, with only one study (n = 1; 2%) reaching this level. In 23 of the 50 studies (n = 46%), TP was the sole intervention. Several studies included TP with only one specific concomitant procedure, such as medial patellofemoral ligament (MPFL) reconstruction (n = 14, 28%), extensor apparatus balancing (n = 1), supracondylar external rotation osteotomy (n = 1) or closing wedge osteotomy of the patella (n = 1). All other studies incorporated TP alongside a heterogeneous mix of additional procedures (n = 10, 20%) within their patient cohorts.
Various techniques for performing TP have been described in the literature. SRs (n = 16) frequently did not specify the technique used in the included studies. Among the remaining studies, the Bereiter technique (n = 21; 61.8%) and the Dejour technique (n = 12; 35.3%), along with modifications of these approaches, were the most commonly represented in this review (Figure 6). Additionally, one study employed a lateral wedge TP. Notably, two studies reported the use of the Bereiter technique in an arthroscopic manner, highlighting the evolving nature of surgical approaches in this domain.
Distribution of the surgical technique described in articles.
Quality assessment
The methodological quality of 26 studies was assessed, while 24 studies—including 16 SRs and meta‐analyses, 4 articles on surgical techniques, 2 biomechanical studies, 1 histological examination and 1 case report—were excluded from evaluation, as the selected scoring systems were not designed for these study types (Table 2). The mean quality scores were 60.8 ± 9.8 for MCMS (n = 26), 11.1 ± 2.9 for MINORS (n = 26) and 22.5 ± 2.1 for MQCSRE (n = 25). Ten studies (43.5%) attained a MINORS score of 12 (or 18 for comparative studies) or higher, which is a commonly recognised threshold for high‐quality research. Interrater assessments showed fair agreement for MCMS (κ = 0.36) and moderate agreement for MINORS (κ = 0.54) and MQCSRE (κ = 0.47), indicating consistency between the two raters [10].
All mean scores, with the exception of MINORS scores from 2010 to 2019 compared to 2020 to 2024, showed an upward trend over the past three decades, as detailed in Table 2. This finding suggests an enhancement in methodological quality, particularly in studies assessed by the MINORS criteria during this time frame.
The comparison of the three quality scores between articles published by institutions based in America, Europe and Asia revealed no statistically significant differences (p > 0.05). However, Germany demonstrated a significantly higher mean MINORS score of 13.83 ± 4.67, compared to the mean score of 10.30 ± 1.49 from the rest of the countries (p = 0.028). In contrast, the other two scores, MCMS and MQCSRE, showed no statistically significant differences between countries (p > 0.05).
Citation counts
A substantial proportion of the citations (1551; 62.5%) originated from publications in three prominent journals. Of these, 803 citations (32.4%) were derived from articles published in Knee Surgery, Sports Traumatology, Arthroscopy, 444 citations (17.9%) came from The Journal of Bone and Joint Surgery (combining both the American and British volumes), and 304 citations (12.3%) were attributed to articles from The American Journal of Sports Medicine. An examination of the past three decades reveals that 37 out of 50 records (74%) were published between 2010 and 2019, corresponding to a concentration of 1561 citations (62.9%) during this decade. The average number of citations per article from this period reached 42.19 ± 33.20. In contrast, articles published between 2000 and 2009 received a significantly higher average citation count of 106.00 ± 39.45 per article, while those from 2020 to 2024 had a mean citation count of 14.40 ± 2.51 per article. These differences were statistically significant (p < 0.001).
Only marginal variations were observed when analysing citation density across the decades. The mean citation density was 6.01 ± 2.07 for articles from 2000 to 2009, compared to 4.90 ± 2.77 for the 2010–2019 period, and 4.81 ± 1.88 for articles from 2020 to 2024. These differences, however, did not reach statistical significance (p > 0.05). The study with the highest citation density, at 13.35 citations per year, was also the most cited overall (187 citations), authored by Dejour and Saggin. This indicates that while citation counts vary significantly by decade, the rate of citations accumulated per year remained relatively stable across time [6].
Interestingly, no significant correlation was found between citation count and the three study quality scores (MCMS: p = 0.543; MINORS: p = 0.122; MQCSRE: p = 0.941) or LOE (p > 0.05). Furthermore, citation counts and citation densities showed no significant variation based on the country of origin (p > 0.05). Similarly, when comparing continents (America, Europe and Asia), there were no significant differences in mean citation counts or citation density per article (p > 0.05).
A higher mean citation count was observed for studies employing the TP technique described by David Dejour compared to the thin flap technique described by Bereiter (69.8 ± 54.6 vs. 50.43 ± 44.0; p = 0.178). Dejour's TP was also cited more often per year (6.16 ± 2.97 vs. 4.42 ± 2.43; p = 0.082). However, these differences were not statistically significant.
DISCUSSION
The primary objective of the current analysis of the 50 most cited studies on TP was to assess the methodological quality of publications in this field and to determine whether the quality of these studies correlated with their citation frequency. No significant correlation between citation count and methodological study quality scores (MCMS, MINORS and MQCSRE) or LOE was discovered.
The scarcity of Levels I, II and III studies was notable, with Level IV studies comprising 82% (n = 41) of analysed studies. No randomised controlled trials were identified, and only one prospective study (2%) was included. Additionally, a significant portion of the studies were SRs and meta‐analyses (n = 16; 32%), underscoring the need for research with higher methodological quality and levels of evidence in this domain. However, should be acknowledged that this is particularly challenging in surgical fields due to strict regulatory requirements and the inherent variability in indications and concomitant procedures, which limit the feasibility of conducting randomised and controlled trials [14]. Although no significant correlation was found between citation count or JIF and the methodological quality of the studies, a substantial portion of the top 50 studies (n = 37, 74%) were published in journals ranked in the top quartile of the orthopaedic subcategory based on impact factor. This highlights the reliance on journal reputation and author prestige as proxies for research quality by orthopaedic surgeons. It underscores the need for an objective tool to assess methodological quality, as the journal may not always reflect the true rigour or scientific merit of the research [5]. Therefore, it is advisable to carefully consider the study methodologies when selecting papers for citation. The LOE within the top 50 was achieved by the study published by Balcarek and Zimmermann [3], conducting a comparative analysis of preoperative and postoperative patellofemoral morphology using MRI in patients who underwent TP and MPFL reconstruction, matched with control patients of similar age and gender. This exemplary study highlights the importance of robust methodologies in providing reliable, high‐quality scientific evidence for clinical decision‐making. It is noteworthy that the only study with this degree of scientific evidence compares radiographic parameters and not clinical outcomes.
Additionally, it was hypothesised that factors such as the country of origin, year of publication, journal of publication, and surgical techniques might correlate with citation count, citation density, and methodological quality scores in the top 50 most cited studies. A significant difference was observed only in the mean MINORS score, with papers from German institutes achieving a higher average compared to the overall mean MINORS score of studies from other countries (13.83 ± 4.67 vs. 10.30 ± 1.49; p = 0.028). Additionally, while methodological quality scores generally improved over the past three decades, the only statistically significant increase was seen in the MINORS score for studies published between 2010 and 2019, compared to the preceding decade (11.83 ± 3.05 vs. 9.17 ± 1.60; p = 0.18). This highlights a modest yet notable enhancement in the methodological rigour of studies over time.
Historically, TP has been predominantly a European‐centred topic, with the majority of studies (n = 40; 80%) originating from European institutions, particularly in France, Switzerland, the United Kingdom and Germany. Comparisons across decades suggest a growing interest from American institutions. Additionally, there has been an observable trend of increasing publications per 5‐year period, signalling a growing interest and expanding research focus on TP in recent years.
Studies utilising the TP technique first described by Dejour demonstrated a higher mean citation count (69.8 ± 54.6) compared to those using Bereiter's thin flap technique (50.43 ± 44.0); these differences were not statistically significant. Interestingly, despite the higher citation count for Dejour's technique, Bereiter's method was used in 21 of the top 50 studies, whereas Dejour's technique appeared in only 12, suggesting a broader scientific interest in Bereiter's approach. Leclerc et al. demonstrated in an SR and meta‐analysis, that Dejour's deepening TP is the most effective, with only 1 recurrence in 349 knees (0.28%) versus 18 reported recurrences (n = 18/552; 3.2%) when using Bereiter's technique [11].
Dejour and Saggin published the most cited study in our report [6], accumulating 187 citations and achieving the highest citation density, with 13.4 citations per year. The study's significant citation count likely stems from its comprehensive description of Dejour's original surgical technique for sulcus‐deepening TP. Additionally, the authors conducted an extensive review of radiologic features, surgical indications, complications, and outcomes from previous studies on TP, contributing to its influence in the field. Due to the nature of the study, it was not suitable for the selected quality scoring systems, and thus, no methodological score was recorded.
von Knoch et al. [23] ranked second with 169 citations and a yearly citation density of 9.4 with their 4‐ to 14‐year follow‐up on TP. The mean follow‐up period was comparatively long, with 8.3 years, resulting in middle of the field MINORS and MQCSRE scores of 61 and 23. Despite the study's influence, the MCMS score was notably low, scoring only 8 points and thus ranking last among the evaluated studies.
Ranking third, with 134 citations and a density of 7.1 citations per year, was the study by Schöttle et al. titled ‘Trochleaplasty for patellar instability due to TD: A minimum 2‐year clinical and radiological follow‐up of 19 knees’ [19], being in the middle to lower third in quality scores (MCMS = 10, MINORS = 60 and MQCSRE = 22). In this study, radiological features using CT scans and clinical parameters were evaluated in 16 patients at a mean follow‐up of 3 years. A low number of cases and a short follow‐up period were the main factors contributing to the lower quality scores of this study.
Overall, low MCMS was influenced by small sample sizes (only two studies with more than 80 patients [12, 13]), short mean follow‐up periods (two studies with a mean follow‐up longer than 6 years [15, 17]) and weak study designs, as only one study [3] had a LOE of III. Lower MINORS scores resulted from non‐prospective data collection and the absence of control groups, which significantly impacted the overall MINORS score. MQCSRE scores were relatively consistent; however, the lack of accountability for test‐review bias and inter‐ and intrarater reliability often contributed to lower scores.
This study has several limitations. Given the substantial number of SR, biomechanical or anatomical studies and descriptions of surgical techniques included in the final selection, only 26 studies were subjected to methodological quality assessment. Comparisons among these studies may also be confounded by variations in surgical techniques and concomitant procedures, such as MPFL reconstruction, osteotomies, or extensor apparatus balancing. Moreover, this analysis exclusively utilised search results from WoS and Scopus. A further limitation stems from the inherent subjectivity of certain items on the methodological grading scales. The MCMS score was designed to compare the methodological quality of cohort studies and tends to favour prospective cohort studies. Most of the studies in this top 50 list are case–control or retrospective cohort studies and, as a result, they may be graded up to 15 points lower due to their study type. The MINORS score favours studies with a long follow‐up period and a detailed rehabilitation protocol. Terms such as ‘well‐described’ rehabilitation protocol versus ‘described without complete detail’ within the MCMS scoring rubric introduced subjective variability. Similar problems were observed with the MINORS scale, where criteria like ‘a clearly stated aim’ or ‘follow‐up period appropriate to the aim of the study’ were evaluated to rate study quality, potentially resulting in divergent interpretations of a publication's quality by different investigators. To mitigate this bias, two investigators independently assessed all articles using both scales and reached a consensus in cases of scoring discrepancies. Furthermore, scientific writing itself inherits certain effects, which could bias the results of a study examining citation counts. Researchers often tend to cite highly cited articles more frequently in their manuscripts, creating a snowball effect that can distort the results [9]. This effect is difficult to quantify or estimate.
CONCLUSION
High citation counts did not correlate with superior methodological quality. Despite the lack of studies with high levels of evidence and robust methodological strength, there is an increasing scientific interest in TP as a treatment for patients suffering from PFI. This review of the top 50 most cited studies on TP serves as a valuable resource for orthopaedic surgeons, offering a foundational tool to evaluate the most significant and impactful academic contributions in this evolving field.
AUTHOR CONTRIBUTIONS
Conception: Armin Runer, Alexander Pfarrmaier and Romed P. Vieider. Data curation: Alexander Pfarrmaier and Rodrigo Sanchez. Data analysis: Alexander Pfarrmaier. Preparing the draft of the manuscript: Alexander Pfarrmaier, Rodrigo Sanchez and Armin Runer. Review and Editing: Alexander Pfarrmaier, Rodrigo Sanchez, Romed P. Vieider, Armin Runer, Lukas N. Muench, Lukas Willinger and Sebastian Siebenlist. Supervision: Armin Runer. All authors read and approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
No ethical approval was required for this literature review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Web of Science platform: Web of Science: Summary of Coverage (2004). https://clarivate.libguides.com/webofscienceplatform/coverage. Accessed 13 May 2024.
- 2Arrivé L , Renard R , Carrat F , Belkacem A , Dahan H , Le Hir P , et al. A scale of methodological quality for clinical studies of radiologic examinations. Radiology. 2000;217:69–74.11012425 10.1148/radiology.217.1.r 00oc 0669 · doi ↗ · pubmed ↗
- 3Balcarek P , Zimmermann F . Deepening trochleoplasty and medial patellofemoral ligament reconstruction normalize patellotrochlear congruence in severe trochlear dysplasia. Bone Joint J. 2019;101‐B:325–330.10.1302/0301-620X.101B 3.BJJ-2018-0795.R 230813785 · doi ↗ · pubmed ↗
- 4Coleman BD , Khan KM , Maffulli N , Cook JL , Wark JD . Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Scand J Med Sci Sports. 2000;10:2–11.10693606 10.1034/j.1600-0838.2000.010001002.x · doi ↗ · pubmed ↗
- 5de Sa D , Thornley P , Evaniew N , Madden K , Bhandari M , Ghert M . CH Aracteristics of research studies that i Nfluence practice: a G Eneral survey of Canadian orthopaedic Surgeons (CHANGES): a pilot survey. Springer Plus. 2015;4:62.25674510 10.1186/s 40064-015-0855-4PMC 4320200 · doi ↗ · pubmed ↗
- 6Dejour D , Saggin P . The sulcus deepening trochleoplasty‐the Lyon's procedure. Int Orthop. 2010;34:311–316.20062988 10.1007/s 00264-009-0933-8PMC 2899349 · doi ↗ · pubmed ↗
- 7Dejour H , Walch G , Nove‐Josserand L , Guier C . Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2:19–26.7584171 10.1007/BF 01552649 · doi ↗ · pubmed ↗
- 8Fithian DC , Paxton EW , Stone ML , Silva P , Davis DK , Elias DA , et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004;32:1114–1121.15262631 10.1177/0363546503260788 · doi ↗ · pubmed ↗