Sudden onset chest pain after a CT-scan of the aorta
Fabienne E. Vervaat, Thomas van Brakel, Sjoerd Bouwmeester

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
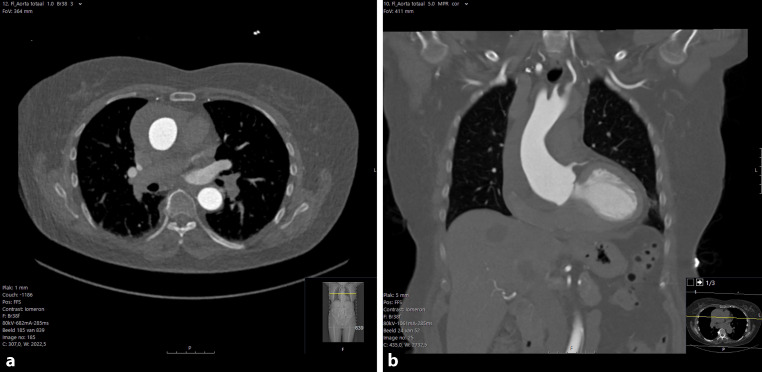 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Pericarditis and Cardiac Tamponade · Infective Endocarditis Diagnosis and Management
Answer
Given the patient’s medical history, there was an immediate suspicion of type A aortic dissection. A new CT-scan was performed and a type A intramural hematoma (IMH) was diagnosed (Fig. 1). Type A IMH is recognized and differentiated from a type A aortic dissection by a crescentic or circular aortic wall thickening in the absence of an intimal flap [1]. IMH is the cause of acute aortic syndrome in 5–25% of the cases with ~30% involving the ascending aorta and in 12% of patients an IMH can evolve into an aortic dissection [1]. The current treatment for type A IMH is comparable to that of type A aortic dissection, which is surgery [1]. Emergency surgery was performed successfully, involving biological aortic valve replacement and hemi aortic arch replacement. The patient’s post-operative recovery was uneventful, and she was discharged after ten days. During the first outpatient follow-up two months later, the patient reported being symptom-free and recovering well.Fig. 1a, b CT-scan of the aorta after symptom onset showing an intramural hematoma located at the aortic root and ascending aorta
The reference list from the paper itself. Each links out to its DOI / PubMed record.