Sudden onset chest pain after a CT-scan of the aorta
Fabienne E. Vervaat, Thomas van Brakel, Sjoerd Bouwmeester

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
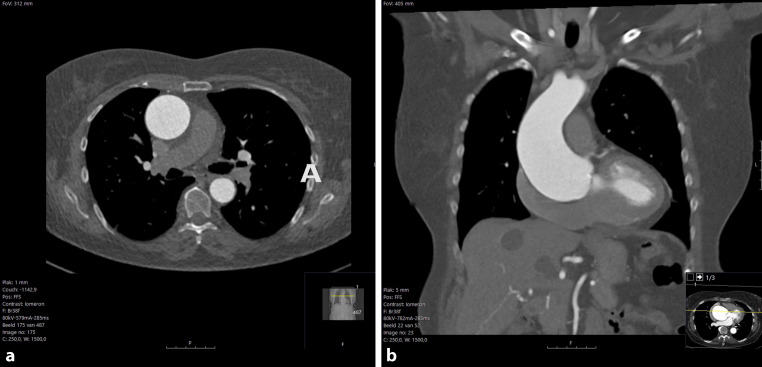 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Pericarditis and Cardiac Tamponade · Infective Endocarditis Diagnosis and Management
A 73-year-old woman presented at our emergency department with sudden chest pain. Her medical records showed a previous diagnosis of bicuspid aortic valve with secondary aortic root (45 mm) and ascending aorta (47 mm) dilatation in 2014, as well as hypertension, which was controlled with metoprolol 50 mg OD and lisinopril 20 mg OD. Since then, she had been undergoing annual CT scans or transthoracic echocardiograms for routine follow-up.
In 2021, her ascending aorta measured 49 mm on CT, while the aortic root remained at 47 mm, and the bicuspid aortic valve showed normal function on echocardiogram. By 2023, the maximal ascending aorta diameter had increased to 58 mm (Fig. 1). Six hours after the CT scan, the patient experienced sudden chest pain, prompting immediate medical attention. Upon presentation, she was conscious and responsive, with a blood pressure of 122/44 mm Hg, heart rate of 58 bpm, oxygen saturation of 100% without supplemental oxygen, capillary refill time of 3 s, and normal physical examination.Fig. 1a, b CT-scan of the aorta prior to symptom onset with dilated aortic root and ascending aorta
What is the diagnosis?
Answer
You will find the answer elsewhere in this issue.