Subcutaneous dirofilariasis
Poorvi Sharma, Nitin Gupta, Idzi Potters, Anjely Sebastian, Muralidhar Varma, Juhi Irfana Basheer, R Balakrishnan, Nancy Namrata Mahapatra, Vishwapriya M Godkhindi, Kanthilatha Pai, Anuradha Calicut Kini Rao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
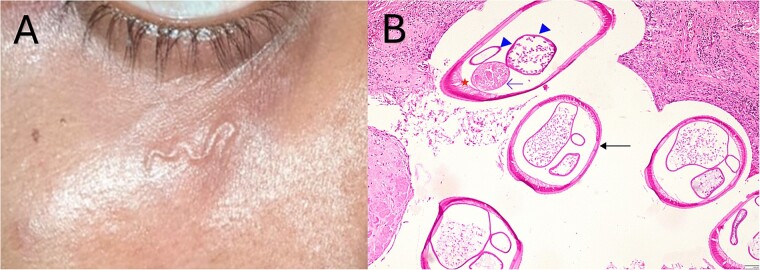 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic Diseases Research and Treatment · Body Image and Dysmorphia Studies
Clinical image
A 19-year-old male student, resident of Udupi, Karnataka, India, without any co-morbidities or history of travel, presented to a primary care physician with acute onset wiggling sensation below the right eye. This was accompanied by a subcutaneous structure resembling a worm (Fig. 1A). There was no fever, itching, pain or redness. The patient was managed conservatively with anti-inflammatory medications in the hope of a spontaneous resolution. Over a few days, a swelling developed at the site, which grew in size over three months.
Subcutaneous worm below the right eye (A); Haematoxylin and eosin stain (200X magnification) of the cross-section of the worm shows smooth longitudinally multilayered ridged cuticle sans bumps (thick arrow), internal lateral ridge with tall coelomyrian musculature (asterisk), paired reproductive tubules (arrowhead) and intestine (thin arrow) (B).
The patient presented to our tertiary care centre with a subcutaneous nodule beneath the right eye. This nodule was excised, and a worm was noted on gross examination. On histopathological examination, longitudinal ridges on a thin cuticle and coelomyarian musculature were observed (Fig. 1B), leading to the morphological identification of possible Dirofilaria repens or Dirofilaria spp Hong Kong genotype. No hypereosinophilia or microfilaremia was noted on the peripheral blood smear. No anti-parasitic medications were prescribed, and the patient remained asymptomatic on follow-up three weeks later.
Dirofilariasis is caused by a zoonotic parasite accidentally introduced into humans when an infected mosquito takes a blood meal [1]. It presents with either pulmonary involvement (Dirofilaria immitis) or as subcutaneous dirofilariasis (D. repens, D. tenuis, Dirofilaria spp. Hong Kong genotype) [2]. Subcutaneous dirofilariasis is reported in several regions of Asia, Africa, and Europe. After the third stage larva matures into adult worms, it may migrate to multiple places, leading to transient swellings, eventually forming a nodule in the eyes, peri-orbital region or other upper body parts. In human infections, a single worm is usually involved, probably due to the host’s immune system decreasing the chances of maturation of multiple worms. Consequently, microfilaremia is rare due to the lack of reproduction inside the human host [1, 3]. A gross examination of adult Dirofilaria spp shows a worm of 300–400 μm diameter and a length of around 10 cm [4]. Histopathological examination can help with the speciation, as longitudinal ridges on the cuticle are absent in Dirofilaria immitis [4]. Surgical excision is the preferred treatment. Dirofilariasis can be prevented in endemic areas by avoiding mosquito bites (minimising exposed body surface area, using insect repellents, and using insecticide-treated bed nets).
Dirofilariasis should be suspected in individuals with worm-like swelling or subcutaneous nodules, especially when they have a residence history or travel to endemic areas in Asia, Africa and Europe.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kini RG, Leena JB, Shetty P. et al. Human dirofilariasis: an emerging zoonosis in India. J Parasit Dis 2015;39:349–54. 10.1007/s 12639-013-0348-8.26064035 PMC 4456557 · doi ↗ · pubmed ↗
- 2Winkler S, Pollreisz A, Georgopoulos M. et al. Candidatus Dirofilaria hongkongensis as causative agent of human ocular Filariosis after travel to India. Emerg Infect Dis 2017;23:1428–31. 10.3201/eid 2308.170423.28726623 PMC 5547781 · doi ↗ · pubmed ↗
- 3Capelli G, Genchi C, Baneth G. et al. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasit Vectors 2018;11:663. 10.1186/s 13071-018-3205-x.30567586 PMC 6299983 · doi ↗ · pubmed ↗
- 4Matějů J, Chanová M, Modrý D. et al. Dirofilaria repens: emergence of autochthonous human infections in the Czech Republic. BMC Infect Dis 2016;16:171. 10.1186/s 12879-016-1505-3.27094256 PMC 4837637 · doi ↗ · pubmed ↗