Glandular cystitis with nephrogenic metaplasia: an unusual finding
Derqaoui Sabrine, Ibrahimi Ahmad, Jahid Ahmed, Zouaidia Fouad, Znati Kaoutar, Nouini Yassine, Bernoussi Zakia

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
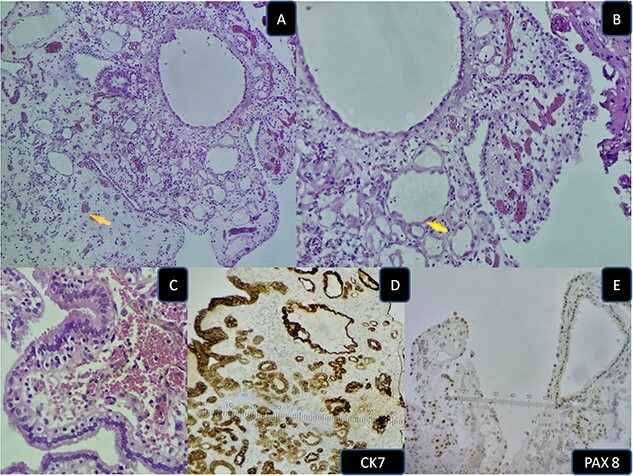 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary and Genital Oncology Studies · Urological Disorders and Treatments · Bladder and Urothelial Cancer Treatments
Nephrogenic metaplasia/adenoma is a relatively uncommon benign urothelial lesion, with a slight male predilection [1]. The pathophysiology remains unclear [2], however it has been reported in the setting of urothelial injury (trauma, calculi, bacillus Calmette-Guérin therapy) [1]. Glandular cystitis is also a reactive inflammatory urothelial lesion characterized by hyperplastic cystically dilated von Brunn nests, lined by glandular cells with or without intestinal metaplasia [3]. Histologically nephrogenic adenoma has three patterns: tubular, cystic and papillary [1]. These structures are lined by cuboidal to columnar cells, with eosinophilic cytoplasm. Hobnail or clear cells may be occasionnaly present. The cytoplasm is pink and occasionally clear [3]. Immunohistochemistry confirms the diagnosis with positivity for cytokeratin 7 (CK7), α-methylacyl-CoA racemase (AMACR) (P504S), PAX2, and epithelial membrane antigen and Pax 8 [1]. These lesions may mimic urothelial carcinoma clinically and endoscopically [1]. Herein we describe a case of 61- year-old man with a previous history bacillus Calmette-Guérin therapy for a high grade urothelial carcinoma with suspicious cystoscopic lesions. Histological examination revealed metaplastic urothelium lined by glandular tall cells arranged in tubular and papillary pattern (Fig. 1A and B), with foci of nephrogenic metaplasia (Fig. 1C). The latter consisted of cuboidal, and hobnail cells with abundant eosinophilic cytoplasm, expressing CK 7 and Pax 8 positive (Fig. 1D and E). The final diagnosis was glandular cystitis with nephrogenic metaplasia. The main differential diagnosis is nephrogenic adenoma-like clear cell carcinoma [1]. In the absence of nuclear atypia, mitosis, necrosis and infiltrative growth pattern, this diagnosis can be ruled out [3]. Other differential diagnoses include, urothelial carcinoma and prostatic adenocarcinoma [3, 4].
In conclusion, nephrogenic adenoma is a benign lesion mimicking malignancy. Careful histological examination with immunohistochemical studies allows for the right diagnosis.
Additionally, 8% of the patients have a previous history of renal transplantation3 or bacillus Calmette-Guérin therapy for urothelial carcinoma of the bladder.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kunju LP . Nephrogenic adenoma: report of a case and review of morphologic mimics. Arch Pathol Lab Med 2010;134:1455–9. 10.5858/2010-0226-CR.1.20923300 · doi ↗ · pubmed ↗
- 2Rostyslav N, Andrii N. Bladder nephrogenic adenoma as a complication of surgical correction of megaureter. Ann Pediatr Surg 2022;18:77. 10.1186/s 43159-022-00215-x. · doi ↗
- 3Harik LR, O'Toole KM. Nonneoplastic lesions of the prostate and bladder. Arch Pathol Lab Med 2012;136:721–34. 10.5858/arpa.2011-0584-RA.22742546 · doi ↗ · pubmed ↗
- 4Manini C, Angulo JC, López JI. Mimickers of urothelial carcinoma and the approach to differential diagnosis. Clin Pract 2021;11:110–23. 10.3390/clinpract 11010017.33668963 PMC 7931042 · doi ↗ · pubmed ↗