Reducing Periocular Edema: Review and Product Concept
Isha Gandhi, Robert Adler, Chase Fishman, Fariha Khan, Mark Albert

TL;DR
This paper reviews methods to reduce eye swelling and introduces a new cooling device designed for gentle and effective treatment.
Contribution
The introduction of Mod-Enswell, a novel cryotherapeutic device for periocular edema.
Findings
A variety of methods including corticosteroids and cryotherapy are reviewed for reducing periocular edema.
Mod-Enswell is proposed as a safe and effective device for focal vasoconstriction and gradual cooling.
Future studies are needed to determine the most effective strategy for treating periocular swelling.
Abstract
Prompt and gentle reduction of periocular edema is imperative. Here, we comprehensively review diverse accepted and novel strategies to mitigate periocular edema including corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), bromelain, diuretics, surgical and other non-pharmaceutical methods, and cryotherapy. We also introduce the concept for an innovative cryotherapeutic device: Mod-Enswell. Made of surgical steel, Mod-Enswell consists of a rectangular base with short pegs extending from its surface. The device was designed to induce focal vasoconstriction and gradually cool skin, features that are especially important considering the delicate nature of periocular skin. This paper explores various avenues to improve patient recovery following periocular swelling; future comparative investigations will be needed to determine the ideal strategy to reduce periocular edema.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
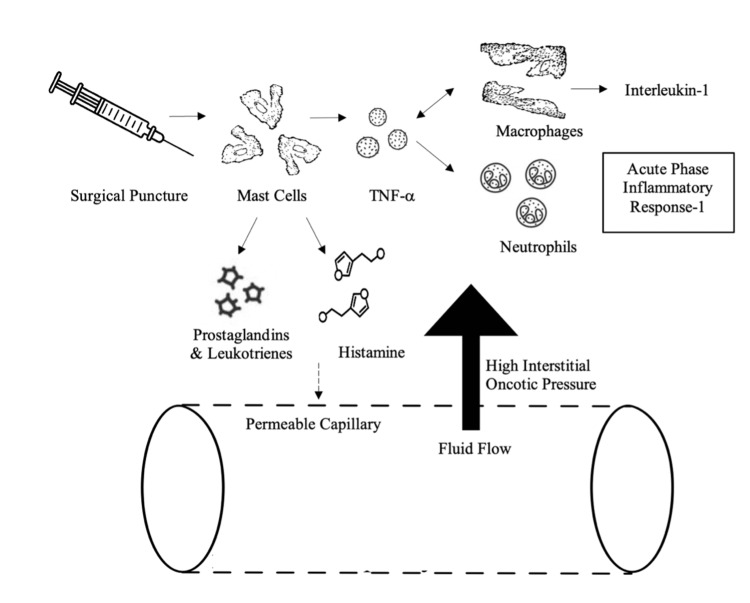 Figure 1
Figure 1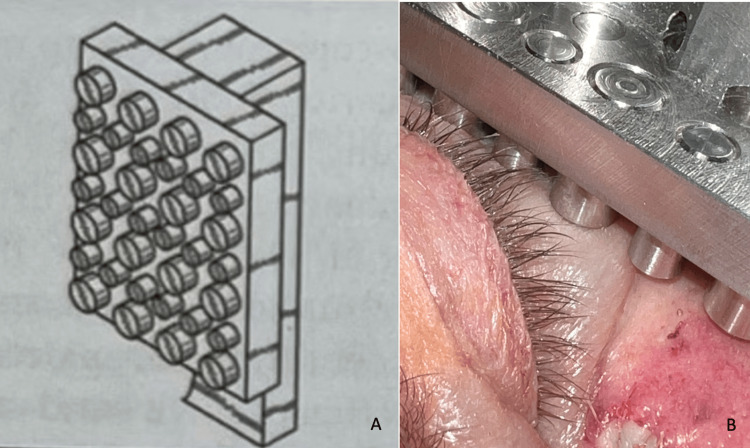 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Surface and Contact Lens · Corneal Surgery and Treatments · Mast cells and histamine
Introduction and background
Periocular trauma is a common reason for emergency room visits, with causes ranging from sports injuries and motor vehicle accidents to fireworks [1-3]. Between 2006 and 2011, ocular trauma represented 77.9% of ophthalmic presentations in emergency rooms nationally [4].
The periocular area, with skin that can be as thin as 0.2 mm, is very susceptible to inflammation and injury [4,5]. Periocular edema can have several etiologies ranging from blunt force trauma to endocrinological, immunological, infectious disease, neurological, and dermatological conditions. Sometimes, periocular edema is the sole symptom of a systemic disease, such as lupus, prior to its diagnosis [6,7]. Initial presentation of periocular edema includes symptoms such as erythema, chemosis and a fatigued appearance.
In the postoperative setting, periocular edema can present either as a result of the procedure, as an exacerbation of a previously associated condition, or due to medications during the procedure. Conditions such as cold urticaria and eyelid-dependent keratoconjunctivitis sicca are common iatrogenic causes of ocular edema [8]. General anesthesia and lidocaine have also been reported to cause periocular edema [9,10]. While post-procedural swelling can vary, edema will generally increase for 48 hours and maximize at 72 hours [5].
However, persistent periocular edema can spread to the conjunctiva, leading to progression of symptoms such as chemosis with corneal desiccation, thinning, and ulceration paired with significant visual disturbances [8]. Moreover, even small alterations in the periocular area can result in dramatic physical appearance changes. For instance, tear trough deformities can result in a sunken eye appearance, creating dark shadows and causing a fatigued appearance despite adequate rest [11].
Considering the adverse clinical outcomes associated with prolonged edema and the nature of inflammation, prompt recovery is imperative [12]. Here, we provide an overview of strategies for minimizing postoperative periocular edema and introduce the concept for a novel cryotherapy device, Mod-Enswell, for this purpose.
Review
Given the limited availability of studies focusing specifically on reducing periocular edema, our literature search was expanded to include relevant publications from 2000 to 2023. PubMed and Google Scholar were utilized to identify pertinent literature related to perioperative periocular edema. The search strategy incorporated a range of relevant keywords, including but not limited to 'postoperative edema,' 'periorbital edema,' and 'edema' to ensure comprehensive coverage of the topic. Literature selection was based on relevance to the study objectives, with a particular focus on studies addressing the management of perioperative periocular edema. Preference was given to peer-reviewed articles.
Pathogenesis of perioperative perioclular edema
Approximately two-thirds of the body’s fluid is contained within cells; the remaining third is in the extracellular compartment. Within the extracellular space, 60% resides in the interstitial fluid, with the remaining 40% in the intravascular space [13,14]. Edema occurs when there is accumulation of excess fluid within the interstitial compartment of tissues or organs [13].
Movement of fluid into the interstitium can arise from increased interstitial oncotic pressure, due to large molecules such as albumin, or from elevated hydrostatic pressure within the intravascular compartment. In a healthy physiological state, hydrostatic pressure marginally surpasses extracellular oncotic pressure, leading to a net movement of fluid into the interstitium. This fluid is subsequently collected by the lymphatic system and returned to venous circulation [13].
In response to surgical incision or puncture, the immune system releases cytokines to promote tissue repair, minimize injury, and prevent infection. Namely, mast cells release histamine and prostaglandin, inducing local vasodilation and increased vascular permeability. Mast cells, amongst other immune cells, also secrete tumor necrosis factor (TNF) which attracts macrophages to injury sites [15,16]. Macrophages subsequently release interleukin-1 (IL-1) and additional TNF, attracting neutrophils and stimulating the acute phase inflammatory response [17,18]. Prostaglandins and leukotrienes are released during this acute phase response, enhancing the permeability of the capillary membrane. The influx of immune cells and inflammatory cytokines increases interstitial oncotic pressure. This combination of heightened vascular permeability and increased interstitial oncotic pressure draws fluid into the interstitium, leading to edema (Figure 1).
Simplified Schematic of Interstitial EdemaSurgical puncture triggers mast cells to release histamine, prostaglandin, and leukotrienes which increase vascular permeability. Mast cells, amongst other immune cells, also secrete tumor necrosis factor (TNF) which attracts macrophages to injury sites. Macrophages subsequently release interleukin-1 (IL-1) and additional TNF, attracting neutrophils and stimulating the acute phase inflammatory response. Prostaglandins and leukotrienes are released during this acute phase response, enhancing the permeability of the capillary membrane. The influx of immune cells and inflammatory cytokines increases interstitial oncotic pressure. This combination of heightened vascular permeability and increased interstitial oncotic pressure draws fluid into the interstitium, leading to edema.Image credits: Isha Gandhi
In the periocular area, where the skin is very thin, this excess fluid stretches the tissues and can lead to a prominent edematous appearance. Moreover, the periocular area has a rich network of lymphatics. During states of inflammation, lymphatic drainage can be impaired, prolonging the presence of edema. Rapidly resolving periocular swelling without compromising the delicate surrounding skin is vital towards ensuring optimal healing and appearance.
Methods to reduce periocular swelling
Prevention of Periocular Edema
While management of periocular swelling in clinic can be accomplished, prevention is ideal. Occupation-related ocular injury presents a significant public health risk, with agricultural and construction workers at higher risk of developing ocular-related injury. Encouraging the use of safety goggles amongst workers most at risk is one of the foremost prevention methods, with studies demonstrating peer encouragement a significant driver of increased use of protective wear and reduction in ocular injury [19,20].
Corticosteroids
Topically applied: Topical corticosteroids are widely used, alleviating various conditions from dermatitis to alopecia areata. Their efficacy and side effects depend on their anti-inflammatory and immunosuppressive properties [21]. These topical treatments are classified by their potency, a measure of their vasoconstrictive properties, and can be considered low, medium, or high potency.
Betamethasone valerate (BMV), a medium potency corticosteroid without mineralocorticoid properties, binds to glucocorticoid receptors and subsequently DNA. This interaction results in the synthesis of anti-inflammatory proteins and inhibits the synthesis of certain inflammatory mediators [22]. Due to its anti-inflammatory properties and non-invasive application, BMV can be used to treat cutaneous periocular edema. A study conducted in 2013 emphasized the efficacy of BMV plasters in alleviating facial edema and inflammation. The study further demonstrated that patients were significantly more satisfied with a betamethasone plaster to reduce facial edema when compared to intradermally administered Acesin cream [23].
Triamcinolone, also a medium-potency corticosteroid, has comparable efficacy to betamethasone dipropionate - more potent than BMV - for the treatment of several conditions [24,25]. Yet, a study demonstrated that achieving the same therapeutic effect with betamethasone dipropionate necessitates a concentration 4.6 times greater than triamcinolone [26]. Given the delicate nature of the periocular skin, treating edema with the less potent BMV may be more beneficial than using triamcinolone in this region.
However, judicious use of BMV is imperative when treating the periocular skin due to its delicate nature. Prolonged use of topical steroids can result in decreased skin elasticity and epidermal thinning [27]. Due to the immunosuppressive and anti-inflammatory properties of topical corticosteroids, prolonged use may result in other side effects: cutaneous infections, rosacea, acne, hypopigmentation, among others. Resolution of these side effects necessitates discontinuing topical steroids, but remission can take months [21].
Systemic steroids: Perioperative corticosteroids can reduce short-term periocular edema by mitigating vascular permeability and providing anti-inflammatory effects [27].
The efficacy of dexamethasone in significantly reducing periocular edema in both the upper and lower eyelids, in comparison to placebo, has been established [5,28]. A 2018 study demonstrated that a minimal intravenous dose of dexamethasone (8 mg) can significantly alleviate periocular edema without triggering any adverse effects in rhinoplasty patients [29].
Prednisone, a glucocorticoid with a shorter half-life than dexamethasone, has also been utilized to mitigate periocular edema [5]. Although limited literature exists comparing dexamethasone and prednisone for edema reduction, trials evaluating both for asthma favored dexamethasone due to its faster action and comparatively fewer side effects [30,31].
The systemic immunosuppressive and endocrine properties of oral corticosteroids can cause several adverse effects. Short-term oral steroid use has been associated with increased intraoperative bleeding and avascular necrosis [27]. Long-term steroid use can lead to a spectrum of symptoms encompassing fatigue, psychiatric disturbances, gastrointestinal symptoms (nausea, vomiting, abdominal pain), dermatological issues (acne, facial erythema, perioral dermatitis), and an increased susceptibility to infection [32].
Given the potential side effects of steroids, first-line treatment for prolonged procedure-induced edema, such as hyaluronic acid for tear trough fillers, typically involves nonsteroidal anti-inflammatory drugs (NSAIDs) [33]. However, if persistent swelling or allergic reactions occur, systemic corticosteroids and antihistamines are recommended [34-36].
Non-steroidal Anti-inflammatory Drugs
NSAIDs are part of the first-line treatment recommendations for prolonged periocular edema following procedures [33]. NSAIDs inhibit cyclooxygenase one and two, curtailing the synthesis of prostaglandins and subsequently reducing vascular permeability and edema [37]. Notably, prior to many in-office procedures, NSAIDs should be avoided for at least five days to prevent bruising [11]. Moreover, NSAIDs are contraindicated in patients with gastrointestinal issues such as peptic ulcers, renal impairment, and NSAID hypersensitivity [37].
Bromelain
Bromelain, a protease derived from pineapples, has potential as a therapeutic agent to reduce periocular edema in the post-operative setting. It has anti-inflammatory, anti-edematous, and antithrombotic effects. A substantial amount of bromelain can be absorbed without losing its proteolytic activity or causing adverse effects [38]. Mechanistically, bromelain reduces inflammation by inhibiting bradykinin production, suppressing leukocyte migration by CD128 receptor antagonism, and enhancing IL-2 which modulates the inflammatory response through Treg activation [39]. Clinically, bromelain has significantly reduced periocular edema in rhinoplasty patients [40]. However, there have been studies that report mixed results on the efficacy of bromelain in reduction of edema, necessitating further research [41]. Notably, bromelain is contraindicated in children due to lack of clinical safety studies [42]. Thus, judicious use of bromelain for periocular edema is imperative.
Surgical and Post-procedural Techniques
Plastic surgeons have explored numerous interventions for periocular edema reduction post-rhinoplasty. A common technique is nasal packing; studies both refute and support the efficacy of this concept in reducing edema post-rhinoplasty. Sowerby et al. found decreased swelling and periocular edema post nasal packing, whereas Arfaj found increased swelling [43,44].
An additional method is periosteal elevation, by which a subperiosteal tunnel is created during lateral osteotomy rhinoplasty; however this method has also produced varied results, with studies showing both increases and decreases in post-operative periocular edema [45,46]. A promising technique that has been studied is the combination of corticosteroids with cold saline gauze compression, which demonstrated decreased edema compared to controls [47]. Additional data is needed to determine the effect of cold saline gauze independent of corticosteroid therapy.
Many practices for reducing periocular edema in plastic surgery settings, such as cryotherapy following blepharoplasty, have potential and may be applied towards other periocular edema etiologies.
Cryotherapy
Cryotherapy is well established in mitigating edema, bruising and erythema [48]. This approach induces vasoconstriction and reduces recruitment of leukocytes, such as macrophages and neutrophils [48]. By disrupting the inflammatory cascade, cryotherapy can alleviate pain and edema [49,50].
However, excessive cooling reduces blood flow, thereby compromising wound healing and extending recovery time [51]. In evaluating whole-body cryotherapy in athletes, serum studies discovered decreased levels of IL-18 and IL2RA, but also decreased ferritin, mean corpuscular hemoglobin, and mean platelet volume, which while within normal range can increase the risk of compromised wound healing [52]. Given the thin nature of periocular skin, avoiding overcooling in this area is imperative. Ice packs, often too cold for the delicate periocular skin, can exacerbate this concern. This is especially important as periocular presentations are common and require swift recovery [5,53]. Therefore, choosing a cryotherapeutic modality that capitalizes on skin-cooling advantages while avoiding its adverse side effects is imperative. Mod-Enswell is a novel device that addresses this necessary balance.
Mod-Enswell
Mod-Enswell is designed with a surgical steel rectangular base with multiple short steel pegs extending from its surface (Figure 2). A 2020 study demonstrated that surgical steel produces significantly less skin temperature cooling within 60 seconds compared to commercial ice packs [54]. This characteristic allows Mod-Enswell to leverage the benefits of skin cooling while circumventing its adverse side effects, rendering it a promising cryotherapeutic candidate for mitigating edema in the delicate periocular area.
Mod-Enswell DevicePanel A depicts a schematic model of Mod-Enswell. Mod-Enswell is designed with a surgical steel rectangular base with multiple short steel pegs extending from its surface. Panel B depicts Mod-Enswell being used on a patient.Image credits: Chase Fishman
Moreover, the undulating steel pegged surface of Mod-Enswell distributes pressure, thereby preventing the blunt pressure-induced damage that can be associated with traditional ice packs. This distributed pressure also reduces the risk of hematoma and clotting. Additionally, the pegged surface facilitates focal vasoconstriction, thus preserving the wound-healing benefits of blood flow while mitigating the inflammatory cascade [55]. Contraindications include allergy to steel and active, profuse bleeding. Adverse effects (AEs) may include discomfort and freezing cold injury. However, the risk of freezing cold injury with this device is lower compared to ice, as steel results in significantly less skin temperature reduction within 60 seconds compared to commercial ice packs [54].
Given Mod-Enswell’s potential to curtail hematoma, reduce edema, and expedite recovery, it is an ideal candidate for clinical evaluation in patients in the perioperative as well as those initially presenting with edema. This is especially significant given the minimally invasive nature of such interventions.
Conclusions
Numerous modalities have been employed to mitigate edema in medical management and procedural settings. While conventional methods such as topical corticosteroids, systemic steroids, and ice packs offer benefits, innovative options such as bromelain and Mod-Enswell have the potential to effectively address edema while reducing undesirable effects. Despite their therapeutic potential, these innovative options have not been clinically evaluated for efficacy in management of periocular edema. Comprehensive comparative investigations are necessary to ascertain the optimal approach to reduce periocular edema in this context.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Medical-attention injuries in community cricket: a systematic review BMJ Open Sport Exerc Med Mc Leod G O'Connor S Morgan D Kountouris A Finch CF Fortington LV 062020 http://10.1136/bmjsem-2019-00067010.1136/bmjsem-2019-000670 PMC 710105132231790 · doi ↗ · pubmed ↗
- 2Incidence, characteristics, and cost of eyelid lacerations in the United States from 2006 to 2014 Ophthalmol Ther Cade KL Taneja K Jensen A Rajaii F 263279122023 https://doi.org/10.1007/s 40123-022-00605-93634264810.1007/s 40123-022-00605-9PMC 9834453 · doi ↗ · pubmed ↗
- 3Firework-inflicted ocular trauma in children and adults in an urban German setting Eur J Ophthalmol Lenglinger MA Zorn M Pilger D von Sonnleithner C Rossel M Salchow DJ Bertelmann E 709715312021 https://doi.org/10.1177/11206721209020333197355110.1177/1120672120902033 PMC 8120635 · doi ↗ · pubmed ↗
- 4Ocular injury in the United States: emergency department visits from 2006-2011 Injury Haring RS Canner JK Haider AH Schneider EB 104108472016 https://doi.org/10.1016/j.injury.2015.07.0202627551210.1016/j.injury.2015.07.020 · doi ↗ · pubmed ↗
- 5Cosmetic blepharoplasty Atlas Oral Maxillofac Surg Clin North Am Niamtu J 3rd 911301220041506233810.1016/j.cxom.2003.10.002 · doi ↗ · pubmed ↗
- 6Periorbital edema as the initial manifestation of pediatric systemic lupus erythematosus Clin Med Insights Case Rep Sliman RK Saied MH 202210.1177/11795476221135430 PMC 963089536339327 · doi ↗ · pubmed ↗
- 7Periorbital edema as initial manifestation of chronic cutaneous lupus erythematosus Pan Afr Med J Erras S Benjilali L Essaadouni L 57122012 https://www.ajol.info/index.php/pamj/article/view/8269222937197 PMC 3428177 · pubmed ↗
- 8Eyelid edema Semin Plast Surg Sami MS Soparkar CN Patrinely JR Tower RN 2431212007 https://doi.org/10.1055/s-2007-9677442056765310.1055/s-2007-967744 PMC 2884828 · doi ↗ · pubmed ↗