Assessment of Serum Dynamic Thiol/Disulfide Homeostasis and Oxidative/Nitrosative Stress in Patients with Crohn’s Disease
Ancel Aysun Bağdaş, Sezgin Barutçu, Ahmet Saracaloğlu, Abdullah Tuncay Demiryürek

TL;DR
This study found that oxidative stress and thiol/disulfide imbalances are more pronounced in active Crohn’s disease, suggesting potential biomarkers for disease monitoring.
Contribution
The study introduces serum thiol/disulfide homeostasis as a novel biomarker for distinguishing active from remission phases of Crohn’s disease.
Findings
Active Crohn’s disease patients showed significantly lower antioxidant enzyme levels and higher nitric oxide levels.
Dynamic thiol/disulfide homeostasis was disrupted in active Crohn’s disease but not in remission.
Thiol/disulfide ratios could serve as potential biomarkers for active disease phases.
Abstract
Crohn’s disease (CD) is a major subtype of chronic relapsing inflammatory gastrointestinal disorders. In this study, we assessed the possible contributions of serum oxidative/nitrosative stress and dynamic thiol/disulfide homeostasis to CD pathogenesis. Patients with active CD (A-CD) at onset (n = 38), CD patients in the remission (R-CD) (n = 38), and healthy controls (n = 38) were prospectively included in this study. Serum oxidative/nitrosative parameters as well as total thiol and native thiol levels were analyzed. We observed significant augmentation in nitric oxide (NO) levels in both A-CD and R-CD patients compared to healthy controls. We detected marked reductions in the 3-nitrotyrosine levels in the patient groups. Glutathione, glutathione peroxidase, and myeloperoxidase levels were observed to be significantly lower in both the active and remission groups (P < .001). In the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1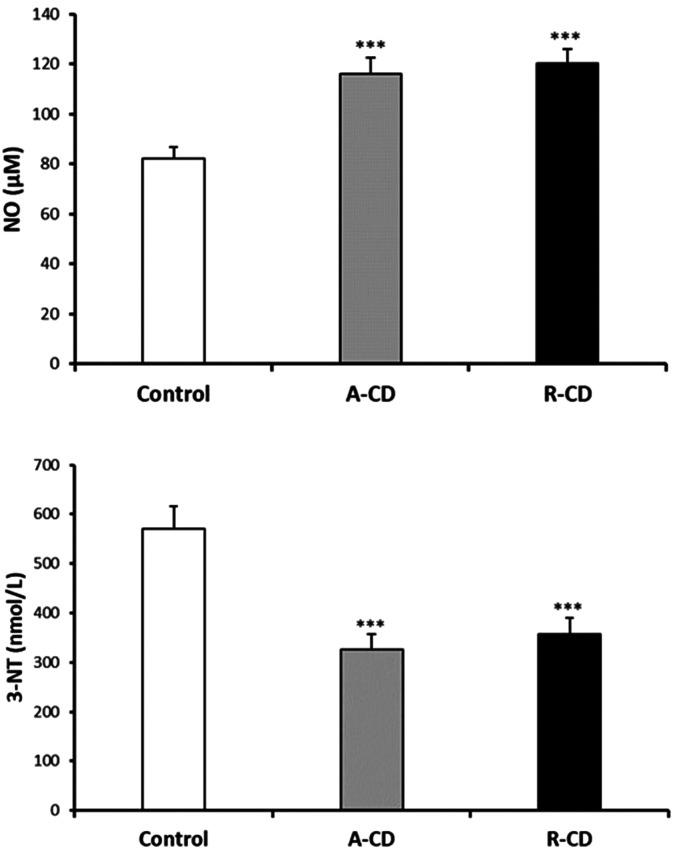 Figure 2
Figure 2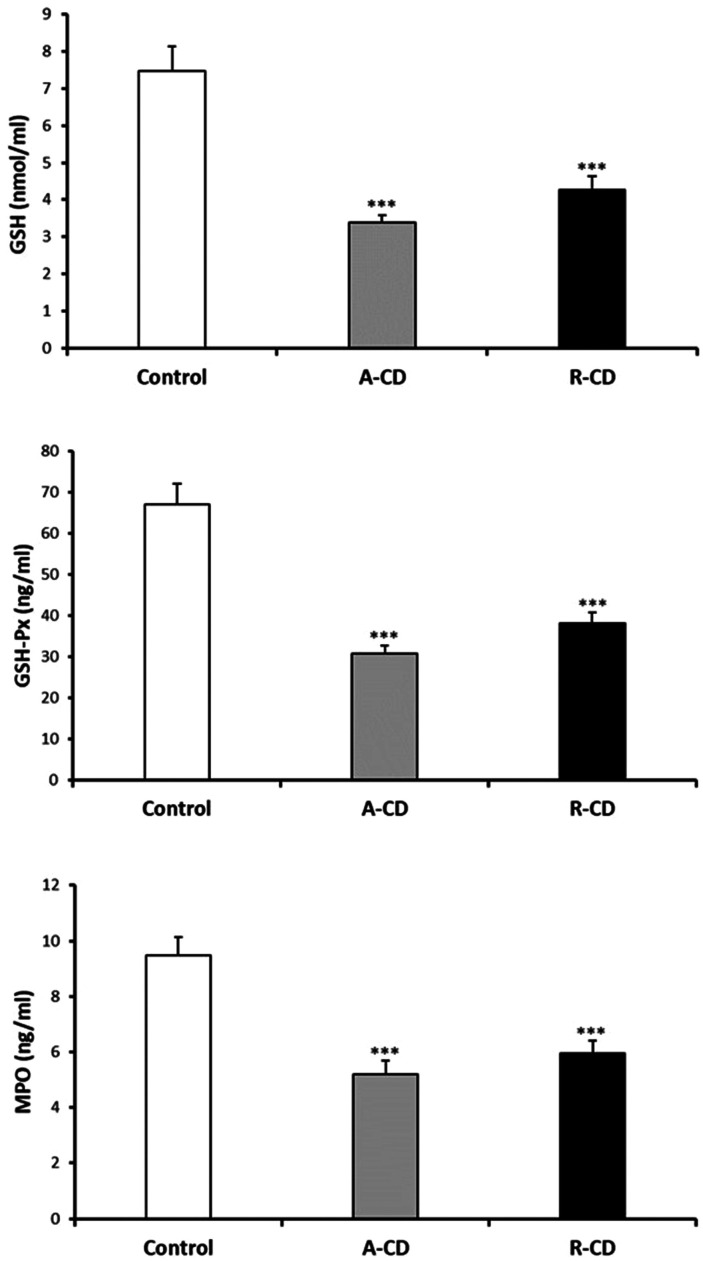 Figure 3
Figure 3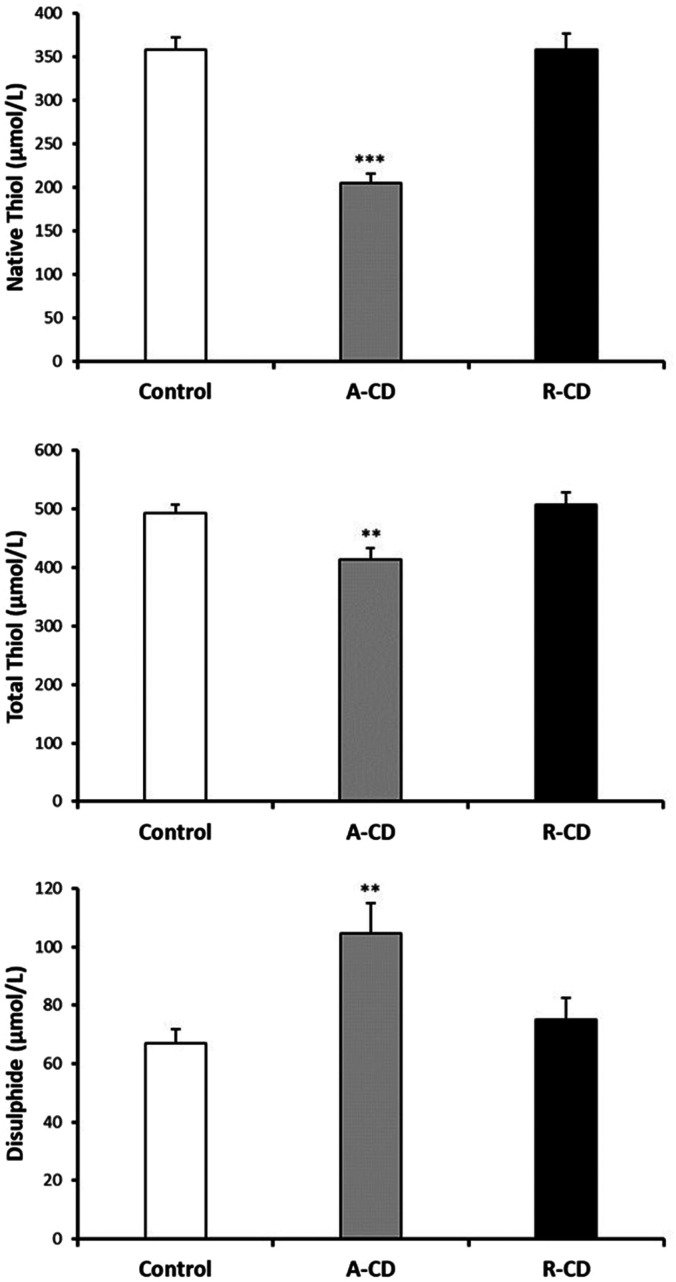 Figure 4
Figure 4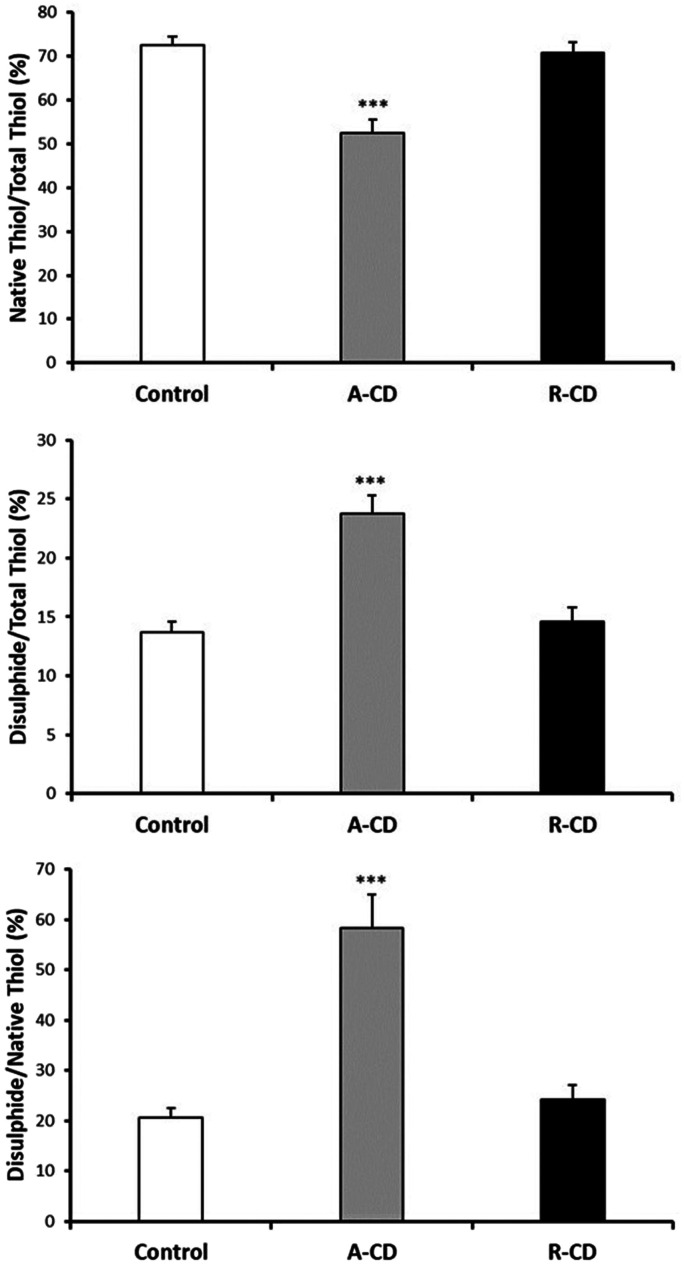 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHuman Health and Disease · Hydrogen's biological and therapeutic effects · Medical and Biological Ozone Research
Introduction
Crohn’s disease (CD) is a complex remitting–relapsing inflammatory bowel disease (IBD) with a multifactorial origin causing uncontrolled and inappropriate immune response with impaired gut mucosal barrier homeostasis.^1^ The etiopathogenesis of CD involves immunological, genetic, environmental, and microbiological factors that interact to promote immune imbalance and alter intestinal homeostasis, causing the emergence of chronic inflammation. Epigenetic factors also play crucial roles in the pathogenesis of CD.^2^ The main clinical manifestations of CD include diarrhea, abdominal pain, fatigue, fever, nausea, vomiting, and anorexia. Extraintestinal manifestations with mucocutaneous involvement are also evident in CD.^3^ With a rapidly rising trend worldwide, the annual incidence of CD has been estimated at 0.06–29.3 cases per 100,000 people.^4^
Unfortunately, no radical cure for CD is currently available. Due to the autoimmune nature of CD, most of the therapies utilized for this disorder aim to diminish the dysregulated inflammatory response. Surgical intervention for the treatment of Crohn’s-related complications is generally reserved for patients who are in an acute, life-endangering state or who have not responded to pharmacologic therapies. Moreover, surgery is not curative, and patients require ongoing therapy after surgery to prevent disease recurrence.^1,4^
Although the etiological factors for CD are not completely understood, evidence suggests that oxidative stress may be a principal effector mechanism causing tissue injury and cellular damage in the initiation and progression of CD.^5^ The combination of augmented reactive oxygen species (ROS)/reactive nitrogen species (RNS) formation and reduced antioxidant status describes several pathological aspects of CD.^5^ Furthermore, inflammation increases oxidative stress by inducing the ROS/RNS-producing systems, along with myeloperoxidase (MPO) enzyme release from inflammatory cells.^5^ Both intestinal epithelial and immune cells generate proinflammatory cytokines that stimulate the formation of ROS/RNS during mucosal inflammation. These reactive species are associated with the progression and/or initiation of CD.^1,5^
Since thiols (sulfydryl groups) are primary substrates for ROS and are rapidly oxidized by ROS metabolites, plasma-free thiols are principally viewed as a strong measure of the *in vivo *redox state. Quantifying systemic redox balance in CD could be an appropriate and minimally invasive strategy for monitoring disease activity.^6^ However, our understanding of the involvement of thiol/disulfide homeostasis in the pathophysiology of CD is limited. Therefore, the objective of this study was to identify the serum oxidative and nitrosative stress states and assess the role of dynamic thiol/disulfide homeostasis in CD.
Materials and Methods
Study population
Using consecutive sampling, a total of 76 patients with active CD at onset (A-CD) (n = 38, age median (range) = 31 (19-68) years old) or with CD in remission (R-CD) (n = 38, age median (range) = 35.5 (21-74) years old) who were admitted to the Gastroenterology Department of the Gaziantep University Hospital between November 2021 and October 2022 were prospectively recruited to participate in this research. This study was approved by Gaziantep University Clinical Research Ethics Committee (approval number: 2021/302, date: November 17, 2021). Written informed consent was obtained from the patients who participated in this study. Prior to beginning drug treatment, serum measurements were taken from patients in the A-CD group. The R-CD group comprised patients who had achieved clinical remission after the flare-up phase of the disease. The control group was composed of 38 age-matched healthy volunteers (n = 38, age median (range) = 31 (25-55) years old), selected from the hospital’s staff and their families. CD patients with any evidence of renal failure, liver disease, bowel obstruction, active gastrointestinal bleeding, abdominal abscess, diabetes, coronary or peripheral artery disease, hypertension, or pregnancy were excluded from the study. In response to ethical concerns, patients in the R-CD group were kept on their current drug therapies. Participants in the control group were excluded if there was documentation of bacterial or viral infection; a family history of CD; diagnosed genetic, neurologic, liver, or psychiatric disease; anti-inflammatory drug usage; or the presence of inflammatory disorders.
Among the patients in the R-CD group, the CD types were 58% inflammatory, 16% obstructive, and 26% fistulizing, and in the A-CD group, 71% were inflammatory, 16% obstructive, and 13% fistulizing. In terms of locations of disease involvement, 37% had ileocolonic, 51% ileal, and 12% colonic involvement in the R-CD group, and 48% had ileocolonic, 37% ileal, and 15% colonic involvement in the A-CD group.
CD diagnosis was based upon colonoscopic/endoscopic data, histopathological evaluation, laboratory findings, and clinical signs.^7^ While endoscopic activity scores were not universally obtainable due to patient preference, the Harvey-Bradshaw Index (HBI) was used to assess clinical disease activity.^8^ The HBI is subclassified as those in remission with a calculated score of <5 or active disease (mild 5-7, moderate 8-16, severe >16). This study received approval from the clinical ethics committee of Gaziantep University (reference number: 2021/302). All participants provided informed consent before enrollment, and procedures adhered to the principles of the Declaration of Helsinki.
Blood samples
Blood samples were collected via venipuncture after an overnight fast. Samples were placed in serum separator tubes, allowed to clot, and centrifuged for 10 min at 1500 g. The resulting serum was immediately stored at −80°C until analysis. All parameters were analyzed in a single-day experiment series to ensure consistent and uniform assay conditions. Samples were thawed and assayed immediately to prevent potential declines in enzyme activity. Additionally, standard laboratory analyses were performed for all patients.
Thiol/Disulfide detection
Serum native thiol (-SH) and total thiol (-SH + -S-S-) levels were measured using a commercially available kits (Rel Assay Diagnostics, Mega Tip Ltd, Gaziantep, Türkiye) according to established protocols.^9^ Briefly, specimens were incubated with 1.9 mM 5,5’-dithio-bis-(2-nitrobenzoic acid) (DTNB, Ellman’s Reagent) in phosphate buffer for 20 minutes at room temperature. Free thiol groups were then quantified by absorbance readings using a microplate reader (Epoch Microplate Spectrophotometer, BioTek Instruments, Winooski, VT, USA). Dynamic disulfide (-S-S) levels were calculated as half the difference between total and native thiol values.
Nitric Oxide (NO) Level Detection
Serum NO levels were determined using a previously described chemiluminescence method.^9^ Briefly, the serum samples were treated with absolute ethanol, and incubated for 30 minutes at 0^°^C followed by centrifugation at 20 800 g for 5 minutes. An NO analyzer (Model 280i NOA, Sievers Instruments, Boulder, CO, USA) was utilized to assess NO levels in the supernatants using vanadium trichloride as the reducing agent. NO levels were calculated from the standard curve produced by sodium nitrate. The NOAnalysis^TM^ software (version 3.21, Sievers, Boulder, CO, USA) was used for data recording and analysis.
ELISA Measurements
Serum 3-nitrotyrosine (3-NT) levels were measured using a commercially available ELISA kit (Cat. No. CK-bio-10045, Coon Koon Biotech Co. Ltd., Shanghai, China). The concentrations of glutathione (GSH) (Cat. No. 201-12-1463), glutathione peroxidase (GSH-Px) (Cat. No. 201-12-0726), and MPO (Cat. No. 201-12-0881) in the serum were detected using commercially available human ELISA kits (Sunredbio Technology Co. Ltd., Shanghai, China). Absorbance readings for all assays were obtained at 450 nm using a microplate reader.
Statistical Analysis
Data were given as mean ± standard error of mean (SEM), standard deviation (SD), or percentages. Normality was assessed using the Kolmogorov-Smirnov test. The Mann–Whitney U test was utilized for data with non-normal distribution. Otherwise, an unpaired Student’s t-test was applied to compare 2 groups of normally distributed data. The ANOVA test was utilized to compare more than 2 independent groups, followed by a post hoc Student-Newman-Keuls test for multiple comparisons. When assumptions of normality were not fulfilled, the Kruskal-Wallis test followed by Dunn’s post hoc test was applied for comparing the means of more than 2 groups. The chi-square or Fisher’s exact tests were utilized to analyze the categorical data. Depending on the distribution of data, correlation analyses were performed with Spearman’s rank or Pearson correlation tests. GraphPad Instat version 3.05 (GraphPad Software Inc., San Diego, CA, USA) or IBM SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) software was used, and P values < 0.05 were accepted as significant. Power analysis conducted using G*Power 3.1.9.4 (Heinrich Heine University, Dusseldorf, Germany) indicated a minimum sample size of 37 subjects per group.
Results
Table 1 summarizes the clinical, laboratory, and demographic data for the CD patient groups and controls. Compared to the control group, gender, average age, smoking status, white blood cell counts, mean corpuscular volume, hemoglobin, glucose, creatinine, urea, aspartate aminotransferase, gamma-glutamyl transferase, alanine aminotransferase, ferritin, folic acid, vitamin B12, and serum globulin levels were similar (P > .05 for all). Platelet count was markedly elevated in the A-CD group compared to the control and R-CD groups. C-reactive protein (CRP) values, alkaline phosphatase activity, and erythrocyte sedimentation rate were significantly higher in both A-CD and R-CD groups compared to controls. However, serum iron, total iron-binding capacity, and albumin levels were markedly lower in both A-CD and R-CD groups compared to controls (Table 1).
3-NT and NO levels were evaluated as the nitrosative stress markers. Serum NO levels were significantly elevated in both A-CD and R-CD patients compared to healthy controls (Figure 1). Serum NO levels were significantly elevated in both A-CD and R-CD patients compared to healthy controls. There were no changes between A-CD and R-CD patients in terms of NO and 3-NT levels (P > .05, Figure 1). Diminished serum MPO, GSH, and GSH-Px were recorded in CD patients (Figure 2). Although there were significant attenuations in serum native thiol (P < .001) and total thiol (P < .01) levels, a marked elevation in disulfide levels (P < .01) was found in the A-CD group compared to controls (Figure 3). These values were not changed significantly in the R-CD group and showed no differences compared to controls. Our data demonstrated that the native thiol/total thiol ratio was declined (P < .001), but disulfide/total thiol (P < .001) and disulfide/native thiol (P < .001) ratios were markedly augmented in the A-CD group (Figure 4). These ratios were not significantly different in the R-CD group compared to controls (P > .05 for all).
Significant correlations between oxidative/nitrosative stress parameters in patients with A-CD at onset are demonstrated in Table 2. Although significant positive correlations were recorded between 3-NT versus GSH-Px, GSH, and MPO, negative correlations were documented between native thiol versus disulfide, and GSH-Px versus NO levels (Table 2). In R-CD patients, 3-NT levels were also positively correlated with GSH-Px, GSH, and MPO. Interestingly, smoking was negatively correlated with 3-NT, GSH-Px, and GSH levels (Table 3). Importantly, no significant correlations were found between clinical disease activity and any of the measured oxidative/nitrosative stress parameters.
Discussion
This study highlights the critical role of oxidative/nitrosative stress and dynamic thiol/disulfide homeostasis in CD. Our data demonstrated that serum levels of the native thiol were significantly depressed during the active phases of CD in patients. Furthermore, we observed elevated serum NO levels and diminished 3-NT levels in CD patients compared to controls.
Growing evidence suggests that inflammation and exaggerated mucosal damage in the early phase of CD are linked with the infiltration of stimulated inflammatory cells.^1,5^ Stimulated neutrophils play a pivotal role in the recruitment of activated immune cells and generate excess MPO, ROS/RNS, and pro-inflammatory cytokines, leading to tissue damage.^1,5^ Elevated ROS levels associated with mucosal damage trigger oxidative stress. Notably, significant correlations exist between CD disease activity and increased mucosal ROS generation in the inflamed colon.^1^ Infiltration of activated neutrophils leads to an augmented risk of thrombosis and compromised resolution of intestinal inflammation during CD.^1,5^ These findings underscore the significant contribution of ROS to the pathophysiology of CD.
We have observed increased platelet counts in patients with active CD at onset. There is evidence showing that thrombocytosis occurs simultaneously with oxidative stress and inflammatory activity in CD.^10^ Regarding the inflammatory status, we observed meaningfully higher levels of CRP in active patients than in patients in the remission, which is consistent with the study published by Maor et al^11^
We have found elevated serum NO levels in both the active and remission phases of CD patients, and these levels were not significantly different between the A-CD and R-CD groups. Our results confirm findings from previous studies, such as the study by Oudkerk Pool et al^12^ who also observed significantly higher serum NO levels in CD patients in the active phase of the disease. Elevated NO production in the colonic mucosa of patients with active CD was reported.^13^ Overall, these results suggest that NO levels are consistently upregulated in CD.
NO regulates various physiological processes in the gastrointestinal tract. Beyond its well-established vasorelaxant effects, NO exhibits inhibition of neutrophils, suppression of adhesion and aggregation of platelets, dilation of nonvascular smooth muscle cells in response to stimulation of peptidergic nerves, augmentation epithelial permeability, and regulation of transepithelial ion secretion. Moreover, it has been suggested that NO may have protective effects during active inflammation.^14^ In colon biopsies obtained from patients with CD, augmented inducible nitric oxide synthase activity and increased NO production were identified.^14^ These findings suggest that at the site of inflammation, the colonic mucosal formation of NO is clearly elevated, and excessive amounts of NO could have cytotoxic effects on colonic cells through the formation of peroxynitrite in CD.
Earlier studies have repeatedly shown that IBD patients demonstrate a diminished total blood antioxidant status, as reflected by reduced total antioxidant capacity and low levels of antioxidant enzymes such as GSH-Px, superoxide dismutase (SOD), and catalase (CAT).^11^ However, findings regarding specific enzymatic antioxidants in plasma/erythrocytes remain somewhat contradictory. Some authors observed decreased^15^ or elevated^16^ levels of antioxidant enzymes in patients with active intestinal inflammation.
The role of SOD, which catalyzes the conversion of superoxide radicals into H_2_O_2_ and O_2_, remains unclear in CD. Decreased Cu/Zn-SOD activity and protein levels in peripheral blood cells of CD patients have been reported.^17^ In contrast, Kruidenier et al^18^ observed selective elevation of mitochondrial Mn-SOD levels in the mucosal tissue of CD patients. Additionally, Tavassolifar et al^19^ revealed significantly upregulated mRNA levels of Cu/Zn-SOD and CAT in CD patients compared to controls. However, owing to the fact that peroxynitrite is the coupling product of NO with superoxide, a decrease in superoxide due to increased SOD could lead to a decrease in peroxynitrite. This may explain decreased serum 3-NT levels in CD patients found in our study. In another report, Dijkstra et al^14^ documented that nitrotyrosine formation was observed on ROS-positive cells, but no differences in 3-NT immunoreactivity between non-inflamed or inflamed CD mucosa and normal controls were observed. These findings collectively suggest that superoxide, NO, and peroxynitrite contribute to CD pathogenesis.
H_2_O_2_ can be eliminated by 2 different enzymes: GSH-Px and CAT. GSH-Px is clearly related to the protection of cells from the damaging effects of ROS. It follows the action of SOD and catalyzes the decomposition of H_2_O_2_ into water and oxygen. Our results showed that there was a depressed GSH-Px in CD, and serum GSH-Px negatively correlated with NO levels, but our results do not support the previous studies reporting increased plasma GSH-Px activity in CD patients.^16,20^ Barros et al^21^ reported that erythrocyte GSH-Px activity was increased in the CD groups. Different studies have presented that GSH-Px is elevated in both plasma^18^ and the colon biopsies^16^ of active CD patients and is regarded as a defense mechanism against oxidative stress. Kruidenier et al^18^ observed a rise in GSH-Px activity in the intestinal CD mucosal tissue in comparison to the controls. Our results suggest that a compromised antioxidant state plays a pivotal role in both active and remission phases of CD.
We have determined diminished serum GSH levels in CD patients, which may support the findings in the affected and normal ileum of CD patients.^22^ Furthermore, our results agree with Szczeklik et al,^23^ who reported decreased serum GSH levels in both inactive and active CD groups. The inflamed ileum of patients with active CD is characterized by both a reduction of GSH and an augmentation of oxidized glutathione (GSSG, glutathione disulfide) in tissue samples obtained from the terminal ileum.^23,24^ Serum GSH levels were also found to be significantly decreased.^25^ The GSH-Px activity, as well as the concentration of its cofactor GSH, has been reported to drop in inflamed mucosa.^23,24^ Similarly, Ruan et al^26^ documented lower GSH levels in inflamed intestinal mucosa compared to healthy controls, with no significant difference between inflamed and non-inflamed mucosa in CD patients. Collectively, these findings suggest that an elevated consumption of GSH in response to nitrosative/oxidative stress may result in decreased cellular GSH levels.
GSH plays a fundamental role in cellular functions, changing the activities of various proteins through thiol-disulfide reactions. It is an important component of the overall antioxidant defense due to its radical scavenging properties. When thiol/disulfide homeostasis shifts towards disulfide production, cellular vital activities are inversely influenced, and this may lead to pathological changes. Available data regarding thiol/disulfide homeostasis in CD is scarce. We have demonstrated that serum native and total thiol levels were attenuated in active CD patients at onset but not in CD patients in the remission. In other words, there were no changes in serum free thiols in CD patients in the remission compared to controls. We also demonstrated augmented disulfide levels in CD. Similar to our results, Bourgonje et al^6^ indicated that free thiol levels in plasma were significantly declined in active CD patients compared to healthy controls. However, our data was not in agreement with Bourgonje et al^6^ who demonstrated that plasma free thiols were diminished in patients with CD in clinical remission compared to controls. Reduced plasma thiol levels were also demonstrated in other studies.^27^ Yuksel et al^28^ indicated that the diminished levels of thiol and elevated levels of disulfide were detected in the IBD group compared to the control group, which is in accordance with our study. We suggest that decreased levels of thiol in patients with active CD are due to increased oxidation.
MPO reacts with H_2_O_2_ and chloride ions to produce hypochlorous acid, a potent oxidizing substance. It has also been indicated that hypochlorous acid is much more toxic than common ROS and is able to interact easily with amino acids, sulfhydryls, pyridine nucleotides, and nitrogenous compounds.^29^ Swaminathan et al^29^ reported that fecal myeloperoxidase can be used as a biomarker of endoscopic disease activity in CD. Interestingly, our study reveals decreased serum MPO levels in CD patients.
Epidemiological evidence strongly implicates cigarette smoking as a major risk factor for CD, both increasing susceptibility and worsening disease progression.^30^ To investigate the potential impacts of smoking on oxidative/nitrosative stress, we conducted correlation analyses. Results revealed negative correlations between smoking and serum 3-NT, GSH-Px, and GSH levels, specifically in CD patients in the remission. This correlation was not observed in patients with active CD at onset.
This study has several limitations. First, we could not directly compare active and remission states within the same patient. Second, most of the patients in the remission phase were also taking medications, and this may affect the results. In the present study, several agents (5-aminosalicylic acid, azathioprine, 6-mercaptopurine, mesalazine, adalimumab, certolizumab, infliximab, and etanercept) were used to put Crohn’s patients into remission. Medications were administered according to individualized treatment needs and indications. Since all the patients received drug combinations, the potential influence of single medications on the measured parameters could not be evaluated. Thirdly, endoscopic activity assessments were not feasible for all patients. Finally, our sample size was relatively small. Future studies with larger cohorts will be necessary to provide a more comprehensive understanding of the biochemical characteristics of this disease.
In conclusion, the current study demonstrates increased oxidative stress, diminished antioxidative status, elevated NO levels, and depressed thiol levels in CD. These findings suggest that serum thiol/disulfide homeostasis could be used as a non-invasive, cost-effective biomarker of CD. The monitoring of thiol/disulfide homeostasis could help discriminate between the discrimination of active and remission phases of the disease. Our data reveal a shift in thiol-disulfide equilibrium towards the oxidative state, accompanied by a depletion of the key antioxidant GSH. This highlights the potential therapeutic value of thiol-containing drugs for CD management. Overall, incorporating antioxidant therapy into treatment regimens may provide a valuable strategy to improve disease outcomes in CD patients.
Availability of Data and Materials:
The data that support the findings of this study are available on request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alemany-Cosme E Sáez-González E Moret I , et al. Oxidative stress in the pathogenesis of Crohn’s disease and the interconnection with immunological response, microbiota, external environmental factors, and epigenetics. Antioxidants (Basel). 2021;10(1):64. (10.3390/antiox 10010064)33430227 PMC 7825667 · doi ↗ · pubmed ↗
- 2Törüner M Ünal NG . Epigenetics of inflammatory bowel diseases. Turk J Gastroenterol. 2023;34(5):437 448. (10.5152/tjg.2023.22515)37158530 PMC 10334590 · doi ↗ · pubmed ↗
- 3Kayar Y Dertli R KonürŞ , et al. Mucocutaneous manifestations and associated factors in patients with Crohn’s disease. Turk J Gastroenterol. 2022;33(11):945 954. (10.5152/tjg.2022.21750)36098365 PMC 9797716 · doi ↗ · pubmed ↗
- 4Ng SC Shi HY Hamidi N , et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769 2778. (10.1016/S 0140-6736(17)32448-0)29050646 · doi ↗ · pubmed ↗
- 5Guan G Lan S . Implications of antioxidant systems in inflammatory bowel disease. Bio Med Res Int. 2018;2018:1290179. (10.1155/2018/1290179)29854724 PMC 5966678 · doi ↗ · pubmed ↗
- 6Bourgonje AR Gabriëls RY de Borst MH , et al. Serum free thiols are superior to fecal calprotectin in reflecting endoscopic disease activity in inflammatory bowel disease. Antioxidants (Basel). 2019;8(9):351. (10.3390/antiox 8090351)31480545 PMC 6769968 · doi ↗ · pubmed ↗
- 7Lennard-Jones JE . Classification of inflammatory bowel disease. Scand J Gastroenterol Suppl. 1989;170:2 19. (10.3109/00365528909091339)2617184 · doi ↗ · pubmed ↗
- 8Harvey RF Bradshaw JM . A simple index of Crohn’s-disease activity. Lancet. 1980;1(8167):514. (10.1016/s 0140-6736(80)92767-1)6102236 · doi ↗ · pubmed ↗