Ureteroscopy and lasertripsy for lower pole stones <2 cm, in situ vs displacement? A systematic review and meta‐analysis
Arran Dingwall, James Leighton, Angus Luk, Mark Chambers, Bhaskar Somani, Robert Geraghty

TL;DR
This study compares two methods for treating kidney stones and finds that moving the stone improves success rates without increasing complications.
Contribution
The study provides a meta-analysis showing displacement improves stone-free rates for lower pole stones <2 cm.
Findings
Displacement strategies significantly increase stone-free rates compared to in situ treatment.
There is no significant difference in complication rates between the two methods.
Displacement requires slightly longer operative time, but the difference is not clinically significant.
Abstract
To investigate the outcomes of ureteroscopy and lasertripsy in lower pole renal stones <2 cm when treated in situ compared to displacement to the upper pole. Using the Medical Literature Analysis and Retrieval System Online (MEDLINE)/PubMed, the Excerpta Medica dataBASE (EMBASE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Library, and Clinicaltrials.gov we identified adult population, English language, studies published until March 2023 comparing surgical outcomes and stone‐free rates (SFRs) in relation to lower pole stones <2 cm managed in situ vs those displaced (International Prospective Register of Systematic Reviews [PROSPERO] identifier: CRD42023432750). Analysis was performed using R with the ‘meta’ package. Bias analysis was performed using the Cochrane Risk of Bias 2 tool for randomised trials and the Newcastle–Ottawa scale for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
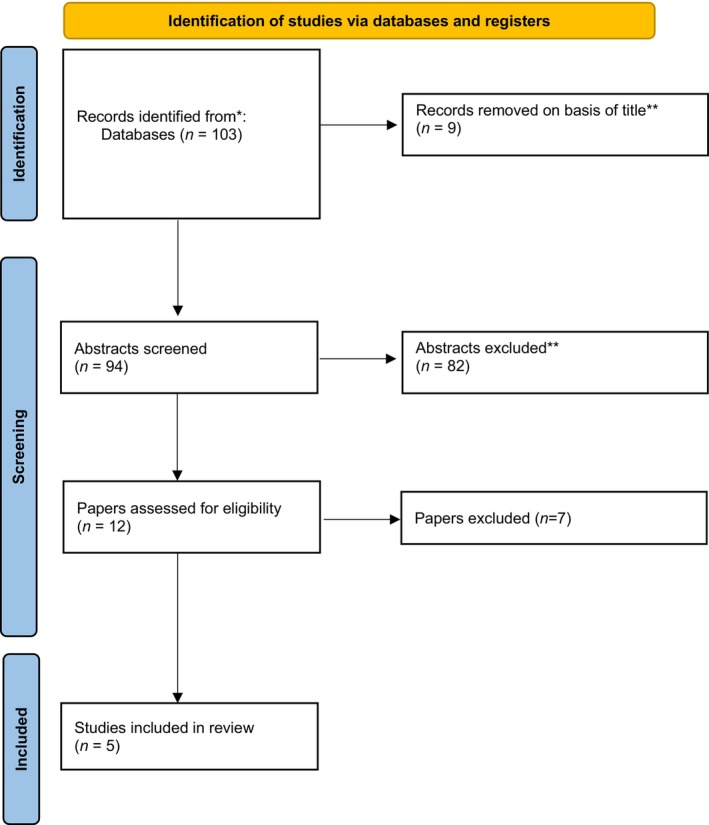 Fig. 1
Fig. 1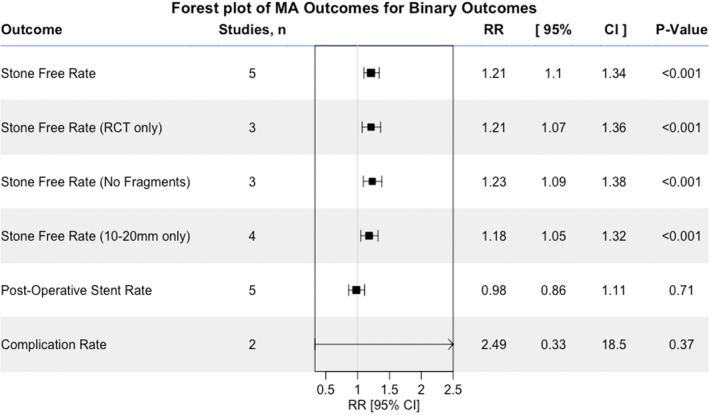 Fig. 2
Fig. 2| Reference | Country | Study type | Total patients, | Female, | Male, |
| Displacement patients, |
| Displacement group age, years, mean (SD) or median (IQR) |
| Displacement group stone size, cm, mean (SD) or median (IQR) | Laser used | Stone‐free definition |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kourambas et al. [ | USA | Retrospective cohort | 34 | 12 | 22 | 24 | 10 | 44 | 44 | 1–2 | 1–2 | Ho:YAG | Completely stone free or <02 cm fragments on either non‐contrast CT or IVU at 3 months postoperatively |
| Schuster et al. [ | USA | Retrospective cohort | 78 | 34 | 44 | 59 | 19 | 47 | 53 | 0.8 | 1 | Ho:YAG | Completely stone free on plain‐film X‐ray immediately postoperatively |
| Yaghoubian et al. [ | USA | RCT | 138 | 69 | 69 | 69 | 69 | 58 (47–68) | 57 (51–64) | 0.6 (0.5–0.7) | 0.6 (0.2–0.7) | Ho:YAG | Completely stone free on plain‐film X‐ray and US KUB at 30 days postoperatively |
| Shrestha et al. [ | Nepal | Prospective randomised study | 68 | 20 | 48 | 35 | 33 | 33 | 42 | 1.2 (0.3) | 1.2 (0.3) | Ho:YAG | Completely stone free on X‐ray and US KUB at 4 weeks postoperatively |
| Huang et al. [ | China | Prospective randomised study | 90 | 36 | 54 | 45 | 45 | 53 | 55 | 1–2 | 1–2 | Ho:YAG | Completely stone free on X‐ray KUB and <0.2 cm residual stones on US KUB at 3 months postoperatively |
| Reference | SFR, % | Operative time, min, mean (SD) | Requirement for postoperative stenting, % | Complication rate, % | ||||
|---|---|---|---|---|---|---|---|---|
|
| Displacement group |
| Displacement group |
| Displacement group |
| Displacement group | |
| Kourambas et al. [ | 83 | 90 | 49 (no split given) | 100 | 100 | 4 | 0 | |
| Schuster et al. [ | 71 | 94 | 64 | 80 | 64 | 42 | 12 | 21 |
| Yaghoubian et al. [ | 74 | 95 | 57 (14) | 66 (10) | 65 | 70 | 6 | 12 |
| Shrestha et al. [ | 86 | 91 | 43 (14) | 48 (13) | 100 | 100 | 14 | 18 |
| Huang et al. [ | 67 | 82 | 40 (17) | 39 (23) | 100 | 100 | 9 | 11 |
| Overall (pooled result from meta‐analysis) | 72 | 86 | 47 (11) | 51 (15 | 76 | 70 | 10 | 14 |
| NOS of risk of bias for observational studies | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference | Domains | ||||||||
| Selection | Comparability | Outcome | |||||||
| Representativeness of exposed cohort | Selection of non‐exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at start of study | Comparability of cohorts | Assessment of outcome | Length of follow‐up | Adequacy of follow‐up cohorts | Overall score (/9) | |
| Kourambas et al. [ | ♦ | ♦ | ♦ | ♦ | ♦ | ♦ | 6 | ||
| Schuster et al. [ | ♦ | ♦ | ♦ | ♦ | ♦ | 5 | |||
| Certainty assessment | Patients, | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations |
| Displacement group | Relative (95% CI) | Absolute (95% CI) | |
| SFR (follow‐up: median 3 months; assessed with: %) | |||||||||||
| 5 | Non‐randomised studies | Not serious | Not serious | Not serious | Serious | None | 168/232 (72.4) | 153/176 (86.9) |
|
| ⨁◯◯◯ Very low |
| SFR RCT only (follow‐up: median 3 months) | |||||||||||
| 3 | Randomised trials | Not serious | Not serious | Not serious | Serious | None | 106/149 (71.1) | 126/147 (85.7) | RR 1.21 (1.07–1.36) | 180 more per 1000 (from 60 more to 309 more) | ⨁⨁⨁◯ Moderate |
| Complications (follow‐up: median 3 months) | |||||||||||
| 5 | Non‐randomised studies | Not serious | Not serious | Not serious | Serious | None | 16/176 (9.1) | 16/232 (6.9) | RR 1.51 (0.86–2.66) | 35 more per 1000 (from 10 fewer to 114 more) | ⨁◯◯◯ Very low |
| Operative time (follow‐up: median 1 days; assessed with: MD) | |||||||||||
| 3 | Non‐randomised studies | Not serious | Not serious | Not serious | Serious | Publication bias strongly suspected | 102 | 104 | – | MD 5.62 min higher (0.4 higher to 10.83 higher) | ⨁◯◯◯ Very low |
- —Royal College of Surgeons of England 10.13039/501100000297
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Pediatric Urology and Nephrology Studies · Central Venous Catheters and Hemodialysis
Introduction
Renal stones have both individual and societal impacts with a significant morbidity [1] and high economic costs [2, 3, 4]. Recent data from the National Health and Nutrition Examination Survey (NHANES) suggests further rises in the prevalence of renal stones in the USA (now 11%), which is likely to be reflective of the developed world [5, 6]. There are three common treatment modalities available for management of renal stones <2 cm: extracorporeal shockwave lithotripsy (ESWL), flexible ureteroscopy (FURS) and percutaneous nephrolithotomy (PCNL), although the AUA [7] and European Association of Urology (EAU) guidelines suggests ESWL or FURS for stones <2 cm [8]. The use of FURS for renal stone treatment has been increasing over the past two decades and is now the predominant treatment type [9]. Lower pole stones (LPS) pose a particular challenge during FURS due to the anatomical and technical complexity of accessing the lower pole [10, 11].
Studies show that these LPS as having lower stone‐free rates (SFRs) during FURS, as low as 60.4% vs up to 94.4% in those stones found in the renal pelvis or upper pole [12, 13, 14]. There are multiple contributing factors to this unfavourable anatomy, including the infundibulopelvic angle (IPA), infundibulopelvic width (IPW), and the length of the inferior calyceal infundibulum [15]. These make FURS more difficult due to the maximum deflection offered by ureteroscopes [10, 11], paired with more difficult anatomy to navigate for the operator [12, 15].
One potential approach to the management of LPS is displacement of stones to the upper renal pole, where these aforementioned complexities are overcome due to the favourable anatomy of the upper pole [13]. We therefore aimed to perform a systematic review and meta‐analysis of displacement of LPS during FURS to the upper pole compared to treatment in situ. Our primary outcome was the SFR, with secondary outcomes of complication rate, postoperative stent rate, and operative time.
Materials and Methods
We report our findings as per the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines [16] (Appendix S1).
Literature Search and Population, Intervention, Comparison and Outcome (PICO) framework
A literature search was carried out by a professional librarian (M.C.), using the Medical Literature Analysis and Retrieval System Online (MEDLINE)/PubMed, the Excerpta Medica dataBASE (EMBASE), Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Cochrane Library. Registered randomised controlled trials (RCTs) were searched using clinicaltrials.gov. The results of this search were reviewed as full‐text manuscripts by two separate authors (A.D. and R.G.).
This literature search was carried out as pre‐defined in the initial protocol on the International Prospective Register of Systematic Reviews (PROSPERO; identifier: CRD42023432750). Study designs included in the search included comparative studies, RCTs and prospective cohorts, as well as retrospective observational studies. Full search terms are summarised in our protocol on PROSPERO. The PICO for this study is detailed below:
Population: all English language, adult patient (aged >18 years) studies.
Intervention and Comparison: studies on ureteroscopy and laser lithotripsy (URSL) for LPS with data of management using in situ lasertripsy (intervention) vs displacement and lasertripsy (comparison) for stones <2 cm.
Outcomes: the primary outcome assessed was study defined SFRs (ideally no fragments), with secondary outcomes comprising of operative time, requirement of adjuvant treatments including stenting, and complication rates (ideally graded using the Clavien–Dindo classification [17]).
Exclusion criteria included any case reports or animal studies.
Data Collection
Data were extracted using a pre‐defined Excel spreadsheet using the criteria above. Sections included: study characteristics of author, country, year of publication and study design; patient and stone demographics of age and sex, stone number, size and burden; and finally operative outcomes including stone‐free status, operative time, need for stenting and perioperative complications. Multiplane measurements of stone burden were converted into single plane by either square or cube root. For outcome measures where only median and interquartile range were supplied, the mean and SDs were calculated as per Wan et al. [18].
Risk of Bias and Publication Assessment
Risk of bias was assessed with: the Cochrane risk‐of‐bias assessment tool for RCTs [19], and the Newcastle–Ottawa Scale (NOS) of risk of bias for observational studies [20].
Publication bias was assessed via visual inspection of Funnel plots and calculation of Cochran's Q. Trim‐and‐fill adjustment was also performed to assess for publication bias, if the number of studies available for analysis was more than three.
Statistical Analysis
A meta‐analysis was performed using a random‐effect model when heterogeneity was >50%, while the fixed‐effect model was used for heterogeneity <50%. Heterogeneity was assessed using I ^2^, tau^2^, and Cochran's Q. All statistical analyses were performed using R (R Statistical software, Vienna, Austria) with the ‘meta’ package [21]. As above, we performed trim‐and‐fill analyses to statistically assess publication bias. All pooled summary statistics are resultant from meta‐analyses of proportion (for binary variables) or single continuous variable. Complete analyses along with statistical code is available in Appendix S2. We performed sensitivity analyses based on study design, stone‐free definition and stone size 1–2 cm.
Results
Study/Patient Demographics
Five studies were identified as meeting the inclusion criteria for meta‐analysis [13, 22, 23, 24, 25] (Fig. 1). These studies comprised a total of 408 patients (male, 237; female, 171) and originated from the USA, Nepal and China (Table 1). There were 232 patients in the in situ group, and 176 in the displacement group, all stones were <2 cm, with all studies bar Yaghoubian et al. [13]. examining stones 1–2 cm (Table 1) [13, 22, 23, 24, 25].
The PRISMA flow diagram for study selection.
All studies utilised a holmium: yttrium‐aluminium‐garnet laser as detailed in Table 1. Use of ureteric access sheaths (UAS) were routine in two studies [22, 25] and surgeon dependent in another [13]. In the remaining two studies [23, 24], UAS were not used; however, if the ureter was found to be unfavourable for ureteroscope passage, balloon dilatation was performed.
In all of these studies nitinol retrieval devices were used, either as a tipless basket or through a nitinol grasper (Table 1). All studies reported complete success of displacement using these devices, with two studies requiring initial in situ laser fragmentation of larger stones (sizes of these stones is not provided in the literature) prior to displacement to the upper‐pole [22, 25].
Studies defined stone free as no fragments, with two studies also including <0.2 cm fragments [22, 23]. Three studies reported that no follow‐up procedures were required in patients who were not stone free [13, 22, 23], one study had a single in situ patient requiring repeat FURS, with the remaining study having a mixture of repeated FURS, ESWL or PCNL (they did not report on the individual groups these repeated procedures belonged to) [24].
Meta‐Analysis for Primary Outcome: SFRs in In Situ vs Displacement
All five studies reported SFRs [13, 22, 23, 24, 25]. On meta‐analysis the SFRs in the displacement group (86%, 95% CI 80–90%) were significantly higher than the in situ group (71%, 95% CI 65–77%; Table 2) [13, 22, 23, 24, 25], using the fixed‐effects model (risk ratio [RR] 1.21, 95% CI 1.10–1.34; P < 0.001; Figs 2 and S1; Section 3.3: Appendix S2).
Forest plot summarising all primary and secondary outcomes.
Results showed minimal heterogeneity with I ^2^ of 3% and tau^2^ analysis of 0.002. Therefore we opted to use the common effect model for the above outcomes. There was no risk of publication bias found on trim‐and‐fill analysis with n = 0 added studies (trim‐and‐fill funnel plot in Fig. S2; Baujat plot in Fig. S5).
Sensitivity analyses of randomised studies only, stone free definition of no fragments only and stones 1–2 cm only, all demonstrated similarly significant results (Fig. 2 and Sections 3.4–3.6: Appendix S2).
Meta‐Analysis of Postoperative Need for Stenting
Stent rates were reported in all studies [13, 22, 23, 24, 25], some studies routinely stented postoperatively (Table 2), with preoperative stenting also varying between studies (Table 1). There was no significant difference found on meta‐analysis of postoperative stenting as shown in Fig. S3 (RR 0.98, 95% CI 0.86–1.11; P = 0.71; see Section 4: Appendix S2). Heterogeneity was again minimal with I ^2^ of 0% and tau^2^ of zero so the fixed‐effect model was used.
Meta‐Analysis of Postoperative Complications
All five studies reported complication rates [13, 22, 23, 24, 25]. There were no significant differences in complication rates between the in situ (10%, 95% CI 6–14%) and displacement groups (14%, 95% CI 9–20%) on meta‐analysis (RR 1.51, 95% CI 0.86–2.66; P = 0.15; Table 2, Figs 2 and S4; Section 5.1: Appendix S2). The common effect model was again used with I ^2^ of 0% and tau^2^ of zero.
Clavien–Dindo grading was available for four studies [13, 22, 23, 25]. Cumulatively by group there were the following numbers of complications: Grade I, in situ seven (4%) and displacement five (3%); Grade II, in situ six (3%) and displacement 10 (6%); Grade III, in situ one (0.6%) and displacement three (2%); Grade IV, in situ none and displacement one (0.6%). Pooling Grades I and II showed no significant differences (RR 1.24, 95% CI 0.60–0.26; P = 0.55; Section 5.2: Appendix S2). Pooling Grades III and IV also showed no significant differences (RR 2.49, 95% CI 0.33–18.49; P = 0.37; Section 5.3: Appendix S2).
Meta‐Analysis of Operative Time
Three studies reported on operative time [13, 22, 23, 25]. There were significantly longer operative times in the displacement group (pooled mean [SD] 51 [15] min) compared to the in situ group (pooled mean [SD] 47 [11] min) on meta‐analysis (mean difference 5.62 min, 95% CI 0.40–10.83 min; P = 0.03). Heterogeneity was significant with I ^2^ of 55% and tau^2^ of 11.7. Cochran's Q was 4.44 (P = 0.11). See Section 6: Appendix S2 for further detail.
Bias Assessment
As above, there was no significant evidence of publication bias found on trim‐and‐fill analysis for our primary outcome of SFRs. For all secondary outcomes there was no evidence of bias and trim and fill was not required to add any results.
For the prospective studies used [13, 22, 25] the Cochrane Risk of Bias 2 (RoB 2) tool [26] was used to assess for risk of bias. We identified low risk of bias in all domains for these first two studies, with some risk of bias identified for Huang et al. [22], as shown in Table 3 [13, 22, 23, 24, 25].
The remaining two studies [23, 24] were retrospective observational studies, assessed using the NOS [20]. We identified an outcome of 6 and 5 out of 9 (some concerns for a risk of bias) for each of these respectively.
Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Assessment
Table 4 details the GRADE assessment. Given the involvement of non‐randomised studies, this downgraded the evidence. However, for our primary outcome of SFR, we graded the certainty of evidence as moderate. With all other outcomes being very low.
Discussion
Data Summary
This systematic review and meta‐analysis of five studies [13, 22, 23, 24, 25] provides evidence for the use of displacement in the management of LPS, showing a significant increase in SFRs in displaced LPS compared to those managed in situ. This is consistent with data from all identified studies showing this same significant increase in SFRs when such stones are displaced [13, 22, 23, 24, 25]. We also demonstrate no significant difference in postoperative stent or complication rates. However, there was a significantly increased operative time in the displacement group compared to the in situ group, with a mean difference of ~6 min.
Strengths of this Systematic‐Review and Meta‐Analysis
The five studies analysed in this systematic review show some bias, with both of the observational studies showing ‘some concern’ of bias from the NOS. This risk of bias comes from neither of these studies accounting for confounding variables; however, reassuringly they both have blindly randomised groups minimising the risk this has to the assessed outcomes. Similarly, data for the prospective study by Huang et al. [22] also showed ‘some bias’ through RoB 2 analysis, due to details on the randomisation process not being present.
Data were also strong regarding heterogeneity, with minimal heterogeneity identified in SFRs, need for stenting and complication rates, with us therefore using common‐effect models throughout. Our sensitivity analyses for our primary outcome (stone‐free status) showed a conserved effect for displacement, which is reflected in the GRADE summary of evidence (moderate).
For the secondary outcomes, there were sufficient studies for meta‐analysis. Of note, four studies reported complications according to the Clavien–Dindo classification, and all studies reported an overall complication rate. Reassuringly, the proportion of complications is low, with only 10% postoperative complications in the in situ group and 14% in the displacement group. There were small, non‐significant rises in major complications (Clavien–Dindo Grade ≥III) in the displacement group; however, the sample sizes were likely too small to detect any meaningful difference. This should be a high priority analysis for a subsequent meta‐analysis once further studies have been published.
External validity of this review is also reassuring, with studies having a near‐even split of patients’ sex and with these studies originating from around the globe (China, USA, Nepal), although ideally studies would originate from more than three individual countries.
Limitations
As shown in the Baujat plot in Fig. S5, we have identified Shrestha et al. [25] as a significant outlier, with over twice the contribution to overall heterogeneity vs the other studies. However, in a leave‐one‐out analysis, the SFRs for displaced stones remained significantly higher than for those left in situ.
Another limitation is shared with many similar aspects of FURS research, and there are confounding variables arising from both study design and variations in patient anatomy. Previous studies have shown that success of FURS may also be related to renal tract anatomy including the infundibulopelvic length, the IPW and IPA [27]. As none of the studies assessed in this review included these data, we are unable to comment on if these have acted as confounding variables. However, the sensitivity analysis of randomised trials, in which anatomical complexity should be evenly distributed across the two groups, do suggest that the treatment effect is conserved.
These study design variables included different methods of identification of stone‐free status through each study. All except one study identified stone‐free status as ‘complete’, with them utilising a range of imaging from ultrasonography and CT to X‐ray. They all differed in when this imaging was used to identify stone‐free status, ranging from immediately postoperatively to 3 months (Table 1). Furthermore, not all studies identified preoperative stone size or burden, giving a significant unaccounted for in this variable.
We identified a statistically significant increase in operative time for the displacement group vs in situ group. However, an ~6 min increase is unlikely to be clinically significant, with the total mean duration in this group of 51 min, remaining under the 90 min recommended as the cut‐off by the EAU guidelines [28].
Possible Areas of Future Research
As discussed above, research suggests that the IPA has a significant bearing on stone‐free status when performing URSL on LPS [15, 27, 29]. Given the significance of the IPA on stone‐free status, future research looking into the IPA with relationship to displacement, ideally identifying cut‐offs where this is most beneficial, would be valuable to this field.
Similar to research on anatomical variations, there is ever‐growing research into variations of stone burden and how that may affect outcomes. The PuRE RCT (International Standard Randomised Controlled Trial Number 98970319; publication pending) has recently been presented at both the AUA and EAU annual meetings, with evidence suggesting that ESWL is the most cost‐effective method of treatment for LPS <1 cm with ‘no meaningful difference in patient health status despite the higher complete stone free rates with FURS’ [5]. They further suggest that PCNL is the most cost‐effective method for treatment of stones 1–2.5 cm [5]. Given these data, it suggests that FURS may become less utilised, although the authors would always advocate for a patient‐centred approach, accounting for individual preferences and contraindications. We eagerly await the published results of the PuRE trial. Further randomised trials into management of LPS with relation to stone burden and anatomical complexity are warranted, as there is currently minimal data on displacement techniques in relation to different stone burdens.
Conclusion
This study presents the most robust evidence to date of using displacement techniques during FURS in the treatment of LPS. The findings presented in this paper have evidenced how displacement of LPS to the upper renal pole has a significantly increased chance of rendering a patient stone‐free following completion of lasertripsy. There is a significant increase in operative time of ~6 min in the displacement group; however, this is likely to be clinically insignificant. There were no significant differences in complication rates. Further trials are needed to improve the certainty of evidence.
Disclosure of Interests
Robert Geraghty is funded by the Royal College of Surgeons of England and is an associate member of the EAU Guidelines panel on Urolithiasis. Bhaskar Somani is a member of the EAU Guidelines panel on Urolithiasis.
Author Contributions
Conceptualisation: Bhaskar Somani, Robert Geraghty; Methodology: Robert Geraghty; Data collection: Mark Chambers, Arran Dingwall, Robert Geraghty; Data curation: Robert Geraghty; Statistical analysis: Robert Geraghty; Writing–original draft: Arran Dingwall, James Leighton; Writing–review and editing: Robert Geraghty, Angus Luk, Bhaskar Somani; Supervision: Robert Geraghty.
Supporting information
Appendix S1. The PRISMA guidelines.
Appendix S2. In situ vs displacement.
Figure S1. Forest plot summarising the primary outcome of SFRs of in situ (control group) vs displacement (experimental group) in the management of lower pole stones. ‘Events’ represent number of stone‐free patients in each group.
Figure S2. Funnel plot demonstrating trim‐and‐fill analysis for meta‐analysis of SFRs.
Figure S3. Forest plot summarising the secondary outcome of perioperative stenting between in situ (control group) vs displacement (experimental group).
Figure S4. Forest plot summarising the secondary outcome of complication rates between in situ (control group) vs displacement (experimental group).
Figure S5. Baujat plot of primary outcome—SFRs—demonstrating each studies contribution to heterogeneity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tapiero S , Limfuco L , Bechis SK et al. The impact of the number of lifetime stone events on quality of life: results from the north American stone quality of life consortium. Urolithiasis 2021; 49: 321–326 33409555 10.1007/s 00240-020-01238-y · doi ↗ · pubmed ↗
- 2Hyams ES , Matlaga BR . Economic impact of urinary stones. Transl Androl Urol 2014; 3: 278–283 26816777 10.3978/j.issn.2223-4683.2014.07.02PMC 4708578 · doi ↗ · pubmed ↗
- 3Geraghty RM , Cook P , Walker V , Somani BK . Evaluation of the economic burden of kidney stone disease in the UK: a retrospective cohort study with a mean follow‐up of 19 years. BJU Int 2020; 125: 586–594 31916369 10.1111/bju.14991 · doi ↗ · pubmed ↗
- 4Antonelli JA , Maalouf NM , Pearle MS , Lotan Y . Use of the National Health and Nutrition Examination Survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030. Eur Urol 2014; 66: 724–729 25015037 10.1016/j.eururo.2014.06.036PMC 4227394 · doi ↗ · pubmed ↗
- 5Mc Clinton S , Starr K , Thomas R et al. The clinical and cost effectiveness of surgical interventions for stones in the lower pole of the kidney: the percutaneous nephrolithotomy, flexible ureterorenoscopy and extracorporeal shockwave lithotripsy for lower pole kidney stones randomised controlled trial (P Ur E RCT) protocol. Trials 2020; 21: 1–15 32498699 10.1186/s 13063-020-04326-x PMC 7273687 · doi ↗ · pubmed ↗
- 6Hill AJ , Basourakos SP , Lewicki P et al. Incidence of kidney stones in the United States: the continuous National Health and Nutrition Examination Survey. J Urol 2022; 207: 851–856 34854755 10.1097/JU.0000000000002331 · doi ↗ · pubmed ↗
- 7Assimos D , Krambeck A , Miller NL et al. Surgical management of stones: American urological association/endourological society guideline, Part I. J Urol 2016; 196: 1153–1160 27238616 10.1016/j.juro.2016.05.090 · doi ↗ · pubmed ↗
- 8Geraghty RM , Davis NF , Tzelves L et al. Best practice in interventional management of urolithiasis: an update from the European Association of Urology Guidelines Panel for Urolithiasis 2022. Eur Urol Focus 2023; 9: 199–208 35927160 10.1016/j.euf.2022.06.014 · doi ↗ · pubmed ↗