Adjuvant chemotherapy in T1a/bN0 breast cancer with a high 21-gene recurrence score (> 25): a 10-year follow-up in a real-world cohort
Daniela Katz, Ilan Feldhamer, Yael Wolff-Sagy, Hadar Goldvaser, Ariel Hammerman, Daniel A. Goldstein

TL;DR
This study examines whether chemotherapy improves outcomes for small, early-stage breast cancer patients with high genetic risk scores.
Contribution
The study evaluates adjuvant chemotherapy benefits in T1a/bN0 breast cancer patients with high 21-gene scores in a real-world setting.
Findings
Adjuvant chemotherapy did not improve invasive disease-free survival in T1a/bN0 breast cancer patients with high 21-gene scores.
Distant recurrence rates were similar between patients who received chemotherapy and those who did not.
The 21-gene recurrence score did not predict improved outcomes in this specific patient group.
Abstract
In ER + /HER2- early breast cancer (BC), 21-Gene Recurrence Score (RS) > 25 indicates high-risk of distant-recurrence and predicts benefit from adjuvant chemotherapy (aCT) regardless of tumor-size. However, T1a/b (≤ 1 cm) node-negative (N0) tumors, regarded as of low risk of recurrence, were under-represented in the RS trials. We therefore aimed to investigate the benefit of aCT in patients with T1a/bN0 BC, RS > 25, where clinical and genomic risk indicators are discordant. This retrospective observational cohort study utilized Israel’s national Oncotest database to identify Clalit Health Services (CHS) members, diagnosed with T1a/bN0 HR + /HER2- BC, who underwent RS testing between February 2006, and December 2019. Patients with RS > 25 who received aCT were matched 1:1 by propensity-scoring to similar patients receiving no aCT. Invasive disease-free survival (iDFS) and distant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
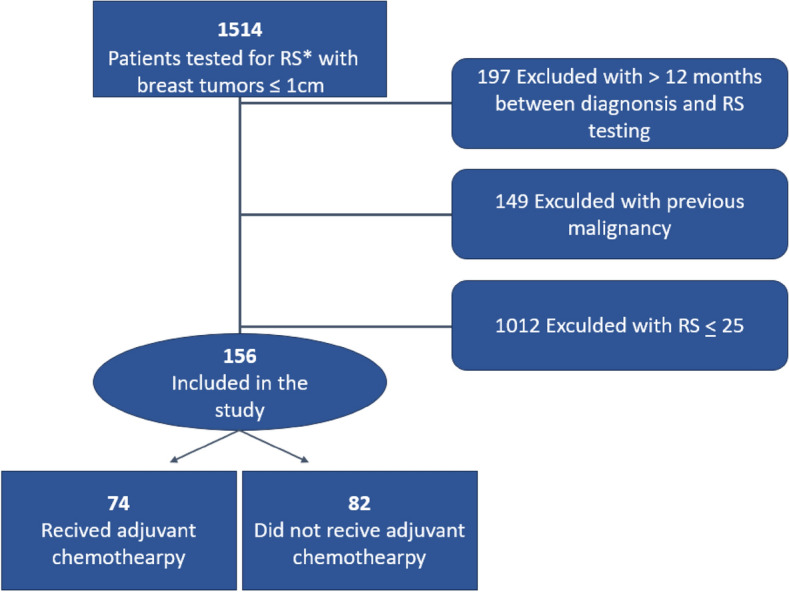 Figure 1
Figure 1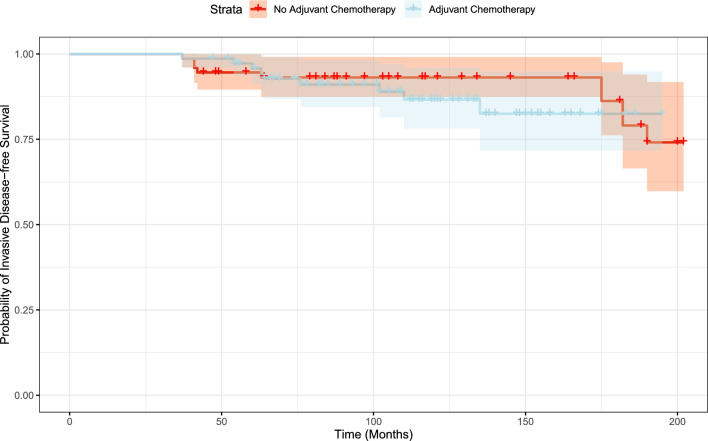 Figure 2
Figure 2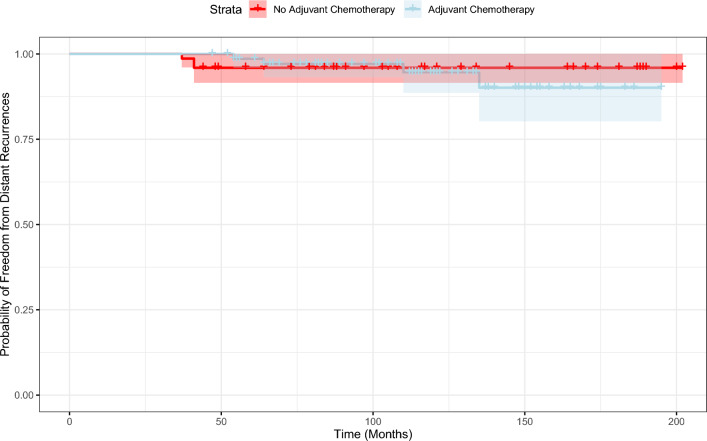 Figure 3
Figure 3- —Hebrew University of Jerusalem
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Cancer Genomics and Diagnostics · Breast Lesions and Carcinomas
Introduction
The OncotypeDX^®^ 21- gene expression assay (Genomic health, Redwood City, CA) is prognostic and predictive of benefit from adjuvant chemotherapy (aCT) for women with hormone receptor-positive (HR +) and human epidermal growth factor receptor 2 negative (HER2-) early breast cancer (BC) [1–3].
Recurrence score (RS) > 25 was established as a threshold for benefit from aCT based on the TAILORx study [3, 4], which examined the benefit of aCT in lymph node negative (N0) BC. Originally high-risk RS was defined as RS ≥ 31, however, to minimize the potential of undertreatment the high-risk threshold was adjusted to RS > 25 [3, 4].
With the increased use of screening mammography, approximately 20% of newly diagnosed breast tumors are in the T1a/b (tumor size < 0.5–1 cm) N0 stage [5]. Discrepancy between traditional clinicopathological parameters associated with clinical low risk (e.g. T1a/b, N0), and genomic high-risk as determined by RS > 25, raises a treatment dilemma. Prospective data on outcomes of the subgroup of patients with T1b (> 0.5-1cm) N0 and RS > 25 who received aCT is scarce. Even the TAILORx study, that included 188 patients with T1b tumors and RS > 25 the benefit of aCT among patients who received and did not receive aCT (180 vs 8 patients, respectively) was not reported separately [2].
In the absence of prospective data on the benefit of aCT in patients with T1a/bN0 BC and RS > 25, we aimed to examine in a retrospective real-world cohort, whether aCT added to adjuvant endocrine therapy (ET) improved outcomes in such patients. To our knowledge this is the largest study to examine this question.
Methods
This retrospective observational cohort-study utilized Israel’s national Oncotest database, which contains RS-results from the OncotypeDX^®^ 21- gene expression assay, histology subtype, grade, tumor size and HR status of the tested tumors. The Oncotest database includes data of all women in Israel diagnosed with ER/PR positive HER2 negative invasive breast cancer, for whom their oncologist opted to perform the OncotypeDX^®^ 21- gene expression assay.
Within the Oncotest database, we identified women with T1a/bN0 HR + /HER2- BC, who underwent RS testing between February 1, 2006, and December 31, 2019, and were members of Clalit Health Services (CHS), that covers about half of the total Israeli population. Data on aCT treatments provided to patients with RS > 25, the clinical outcomes, demographic characteristics, clinicopathological features and patients’ comorbidities were all extracted from CHS centralized electronic database.
Providing aCT is not standardized and is administrated according to the treating physician’s discretion. ET was recommended to all patients and provision of drug to patients was recorded. Patients with who received aCT were matched 1:1 by propensity-scoring to similar patients receiving no aCT. The primary study endpoint was the occurrence of an invasive disease-free survival (iDFS) event, as defined within the TAILORx [4]; The secondary endpoint was a distant-recurrence event. The outcome data lock was set on June 30, 2023, ensuring a minimum follow-up interval of at least 4.5 years.
Statistical analysis
Descriptive statistics was used for the sociodemographic and clinicopathologic characteristics. All patients’ characteristics were included as categorical variables except for age. To calculate propensity score (PS) for matching non-aCT to aCT patients, a logistic regression was executed with age group, socioeconomic status [6], Charlson-comorbidity index [7], tumor size (≤ 0.5 vs. > 0.5–1 cm), grade, HR status, histology and oncotype score category (26–30 vs. > 30) as independent variables. Of notice, a comparison between the oncotype score categories was conducted to identify an increased benefit of chemotherapy at a higher RS threshold, using the original threshold for chemotherapy benefit (RS ≥ 31) versus the currently accepted threshold (RS > 25) (1, 3). PS with nearest neighbor with replacements and with a caliper of 0.25 was conducted to match patients with aCT with non-aCT on a 1:1 ratio. Of the non-aCT patients, 20 (27%) were used as controls once, 11 (15%) were used as controls with two repetitions, and 7 (9%) were used as controls with three to six repetitions.
Mean-times to an iDFS and distant-recurrence events were compared by Kaplan–Meier analysis with log-rank testing. Patients were censored at data lock date. All tests were 2-sided and p ≤ 0.05 was considered statistically significant. Descriptive statistics, PS calculation and matching and Kaplan–Meier analysis were conducted by SPSS software version 29 (IBM). Kaplan–Meier survival curves were created with R statistical software version 3.5.0 (R Foundation).
The study was approved by the CHS Community Helsinki ethics committee (approval 0074–22-COM2) and was exempt from the requirement to obtain informed consent owing to the retrospective design.
Results
A total of 156 patients met the inclusion and exclusion criteria (Fig. 1), almost half (74 patients, 47.4%) received aCT (Table 1). Median duration of the study follow-up was 121.0 months (95% CI, 108.4–133.6). Patients who received aCT were younger, had less comorbidities, and had a higher RS (Table 1), type of aCT received is shown in Table 2. Duration of ET was not significantly different between both groups.Fig. 1. Consort flow diagram. The patient cohort was extracted from the Oncotest database, which includes RS results from OncotypeDX^®^ 21- gene expression assay, histology subtype, grade tumor size and hormone receptor status. RS: OncotypeDX^®^ 21- gene recurrence scoreTable 1Demographic and clinicopathological characteristics of patients by adjuvant chemotherapy treatment before propensity-core matching and afterNon-matchedPropensity score-matchedno aCTaCTp-valueno aCTaCTp-valuen = 82n = 74n = 74n = 74SociodemographicAge24–498 (9.8%)19 (25.7%)16 (21.6%)19 (25.7%)50–5924 (29.3%)22 (29.7%)20 (27%)22 (29.7%)60–6935 (42.7%)27 (36.5%)33 (44.6%)27 (36.5%)70–7415 (18.3%)6 (8.1%)0.285 (6.8%)6 (8.1%)0.79median62.5 (54–8.3)57.5 (49–4.3)0.00260 (51–65.3)57.5 (49–64.3)0.38SES (6)low11 (13.4%)19 (25.7%)19 (25.7%)19 (25.7%)medium40 (48.8%)30 (40.5%)32 (43.2%)30 (40.5%)high31 (37.8%)25 (33.8%)0.1523 (31.1%)25 (33.8%)0.93Clinical pathological propertiesTumor size (cm) </= 0.56 (7.3%)2 (2.7%)5 (6.8%)2 (2.7%)>0.5–176 (92.7%)72 (97.3%)0.1969 (93.2%)72 (97.3%)0.24Grade18 (9.8%)3 (4.1%)5 (6.8%)3 (4.1%)244 (53.7%)37 (50%)48 (64.9%)37 (50%)319 (23.2%)25 (33.8%)16 (21.6%)25 (33.8%)Unknow11 (13.4%)9 (12.2%)0.325 (6.8%)9 (12.2%)0.17HistologyIDC/Unknown73 (89%)71 (95.9%)70 (94.6%)71 (95.9%)ILC9 (11%)3 (4.1%)0.14 (5.4%)3 (4.1%)0.7ER^#^0–17 (8.5%)5 (6.8%)9 (12.2%)5 (6.8%)2–375 (91.5%)69 (93.2%)0.6765 (87.8%)69 (93.2%)0.26PR^^^0–156 (69.1%)51 (68.9%)51 (68.9%)51 (68.9%)2–325 (30.9%)23 (31.1%)0.9723 (31.1%)23 (31.1%)1.000OncotypeDX recurrence score26–3063 (76.8%)25 (33.8%)29 (39.2%)25 (33.8%)31 + 19 (23.2%)49 (66.2%) < 0.00145 (60.8%)49 (66.2%)0.5Charlson comorbidity score (7)0–140 (48.8%)52 (70.3%)49 (66.2%)52 (70.3%)2 + 42 (51.2%)22 (29.7%)0.00625 (33.8%)22 (29.7%)0.6**SES* socio-economic status, ^#^ER estrogen receptor, ^^^PR progesterone receptorTable 2Adjuvant chemotherapy treatmentsn (%)IV Doxorubicin & Cyclophosfamide16 (21%)IV Doxorubicin & Cyclophosfamide and Taxane24 (32%)IV Docetaxel & Cyclophosfamide33 (45%)IV Cyclophosfamide Methotrexate 5-FluoroUracil1 (1%)Total74
PS-matching resulted in 74 matched cases. The PS-matched groups demonstrated similar socio-demographic and clinical characteristics (Table 1). In addition, a similar distribution of the PS was observed.
Eighteen iDFS events occurred in the matched cohorts, nine in each group (p = 0.39). A total of seven (4.5%) patients were diagnosed with distant-recurrences, four (5.4%) in the aCT group and three (4%) in the non-aCT group (p = 0.64).
The mean time to an iDFS event was 171.5 months (95% CI, 160.9–182.1) and 177.6 months (95% CI, 169.2–186.0) in the aCT and non-aCT cohorts, respectively; p = 0.4. The mean time to distant recurrence was 186.2 months (95% CI, 178.1–194.5) and 188.7 months (95% CI, 181.7–195.7) in the aCT and the non-aCT cohorts, respectively (p = 0.64). Figure. 2 demonstrates iDFS over time and Fig. 3 the distant recurrence events over time, supporting the good outcome of patients with small tumors N0 BC.Fig. 2. Probability of invasive disease-free survival over time. The shaded area represents the confidence intervalsFig. 3Probability of distant recurrence over time. The shaded area represents the confidence intervals
Discussion
In our real-life retrospective cohort, with a median follow-up of 10-years, patients with T1a/bN0 BC and RS > 25, did not show improved iDFS with aCT compared to those who did not receive aCT. To our knowledge, this is the largest cohort examining this question [2, 8, 9].
We chose RS > 25 as the threshold for benefit from chemotherapy in patients without lymph node involvement based on TAILORx results [4], and the NSABP B-20 results when HER2 positive patients were excluded [3].
In our patient cohort three parameters were associated with aCT administration: age, low Charlson’s comorbidity score and RS ≥ 31. This represents the preferences of Oncologists in real-life when considering aCT in T1a/bN0 BC.
Although approximately 20% of newly diagnosed breast tumors are in the T1a/bN0 stage [5], prospective data on the benefits of aCT in this subgroup is lacking. Perhaps, due to limited adoption of aCT within this subgroup as reflected in the recent St. Gallen recommendations where approximately 90% of expert panelists [10] voted against providing aCT for tumors < 0.8 cm N0, despite a high genomic assay result. Interestingly, same experts were more inclined (up to 40%) recommending aCT for slightly larger, 0.8-1cm tumors.
In our cohort, there were 12.2% iDFS events and 4.5% distant recurrences events. Our findings are consistent with the MINDACT study that showed excellent disease-free survival and distant metastasis-free survival in patients with breast cancer of low-clinical (tumors ≤ 1cm N0) and high-genomic risk who did not receive aCT [11, 12].
Interestingly, we noticed that the mean time to an iDFS or to a distant recurrence event exceeded 171.5 and 186.2 months (Figs. 2, 3), respectively, emphasizing the inherent risk for late-recurrence of ER + /HER2- small tumors which is not predicted by the current RS assay [13].
The strength of our study lies in the highly selective study population, consisting of small N0 tumors with high genomic risk and the lengthy follow-up duration (median of ten years). To our knowledge, this is the largest breast cancer real-life cohort that examined benefit from aCT in T1a/bN0 BC. Very small tumors are usually under-represented in clinical trials, e.g. in the TAILORx study only 13% of patients had tumors 1cm or smaller (tumor 0.5 > were excluded) [4] and in the NSABP B-20 trial (excluding HER2 positive by RT-PCR) only 14.9% had such tumors [3].
In addition, we used the CHS registry, a well-established registry reflecting real- world experience that was used as a validation cohort to develop the RSclin tool, which aimed to individualize prognosis and prediction of chemotherapy benefit [13]. The registry served as a basis for many published BC manuscripts [14, 15].
Our study also has several limitations, primarily its retrospective and uncontrolled nature, leading to an imbalance between characteristics of patients who received aCT and those who did not. We addressed the imbalance using PS matching; however, a few control subjects were matched three to six times, even after applying a relatively high caliper of 0.25 for the PS matching. Another significant limitation is the low number of events observed, consistent with the prognosis of patients with low-clinical risk and high-genomic risk in the MINDACT trial [11].
Another study constraint arises from the selection bias inherent in the study cohort, comprised of patients selected by their treating physician to undergo 21- gene expression assay testing. Ordering genomic testing in Israel is at the discretion of the breast surgeon or treating oncologist and not limited by tumor size. Therefore, the study cohort may not represent the entire T1a/bN0 population and represents patients to whom aCT was considered, younger patients or those with a more luminal B-like phenotype BC (defined by grade 2–3, lower progesterone receptor expression and a higher cell proliferation) associated with an inferior outcome. Evidence for poorer outcomes in patients with histological grade 3 tumors and RS > 25 is provided by the study conducted by Stemmer et al., (13) which examined 10-year outcome of patients with N0 BC based on their RS-result in a comparable cohort.
We believe this limitation did not adversely affect the study results, because the absence of benefit from aCT in these higher-risk tumors would probably extend to a lack of benefit in lower clinical-risk tumors with a more luminal A-like phenotype.
Another limitation is the small subgroup of T1a tumors (8/156 patients), especially those treated with aCT (2/8 patients) prevent drawing conclusions regarding any benefit from aCT in this subgroup.
In summary, within our retrospective cohort, providing aCT did not improve outcomes of patients with T1a/bN0 HR + /HER2- BC with RS > 25, suggesting that RS > 25 was not predictive of benefit from aCT in our study. The low number of events observed in our study supports the good prognosis of these patients.
Prospective trials are still needed to identify at diagnosis those few patients who later experience distant recurrence, possibly by evaluating RS ≥ 31 threshold. Another possibility is integrating clinicopathologic biomarkers with the RS, that could potentially lead to more accurate identification of patients with small tumors at high- risk for recurrence, allowing others to avoid unnecessary aCT. This becomes increasingly important as more patients are diagnosed with T1a/bN0 tumors through routine BC screening.