Effects of neutrophil granule proteins on sepsis-associated lymphopenia and their relationship with CD4+ T-cell pyroptosis
Jia-yu Mao, Ya-wen Xie, Xian-li Lei, Jia-hui Zhang, Wei Cheng, Na Cui

TL;DR
High levels of proteins from neutrophil granules are linked to lymphopenia in sepsis patients and may contribute to CD4+ T cell death.
Contribution
This study identifies a novel association between elevated neutrophil granule proteins and sepsis-associated lymphopenia, along with CD4+ T-cell pyroptosis.
Findings
Neutrophil granule proteins MPO and NE are significantly higher in sepsis patients with lymphopenia.
MPO and NE levels independently predict the risk of sepsis-associated lymphopenia.
Neutrophil granule proteins are strongly correlated with CD4+ T cell pyroptosis markers.
Abstract
Neutrophil acts as a double-edged sword in the immune system. We hypothesized that an elevated neutrophil granule protein level is associated with sepsis-associated lymphopenia (SAL). We enrolled 61 patients with sepsis admitted to the Department of Critical Care Medicine of Peking Union Medical College Hospital between May 2022 and October 2023 in this study. Clinical and immunological parameters were recorded. Levels of neutrophil granule proteins, including myeloperoxidase (MPO) and neutrophil elastase (NE), and pyroptosis factors were examined. Levels of neutrophil granule proteins (MPO, 82.9 vs. 175.3, p < 0 <.0001; NE, 56.3 vs. 144.2, p < 0.0001) were significantly higher in patients with sepsis with lymphopenia. Neutrophil granule protein levels were independently associated with SAL risk (MPO: OR = 1.0841, 95% CI, 1.0020–1.1730; NE: OR = 1.0540, 95% CI, 1.0040–1.1065). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
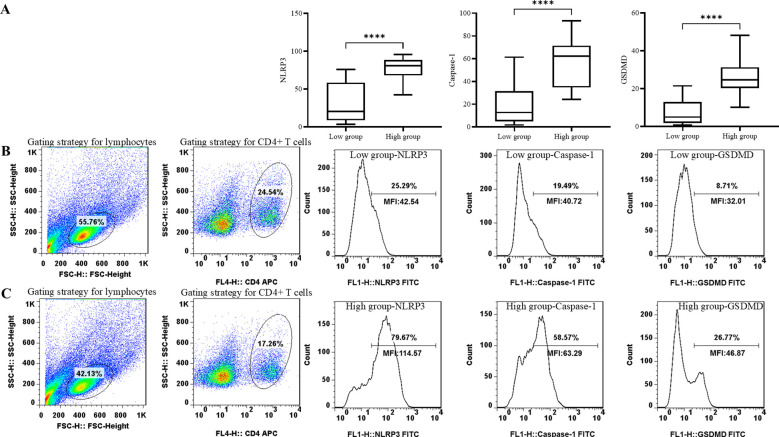 Figure 1
Figure 1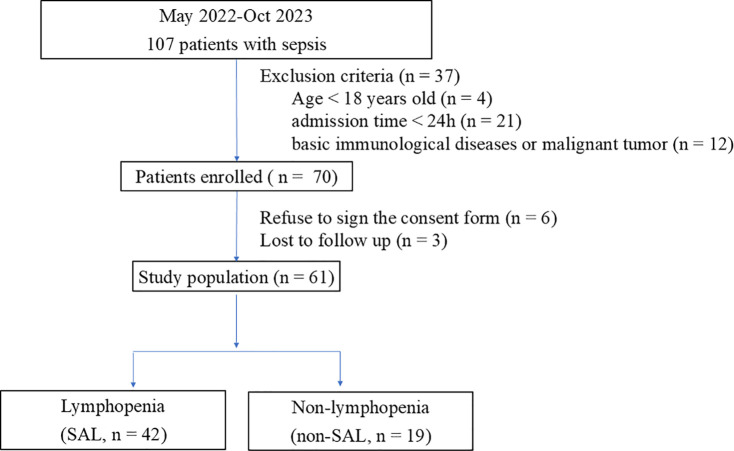 Figure 2
Figure 2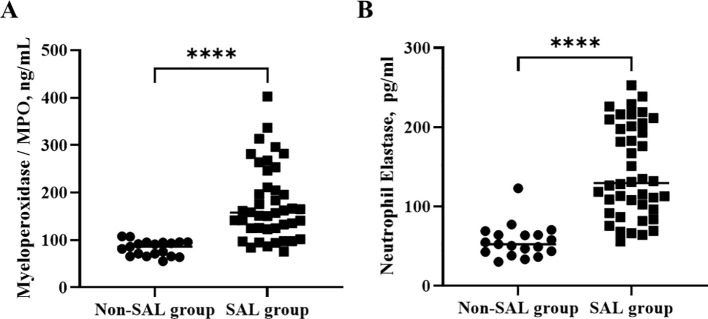 Figure 3
Figure 3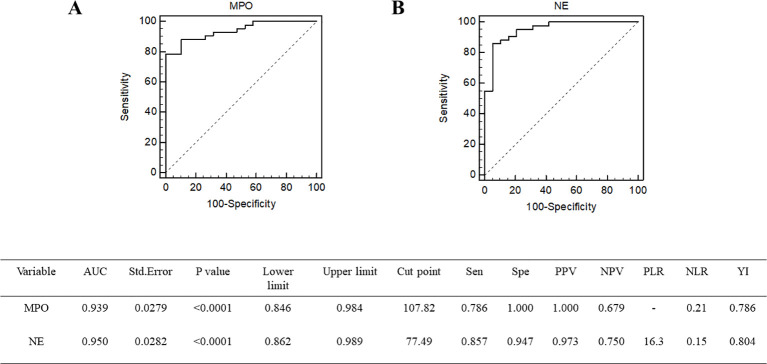 Figure 4
Figure 4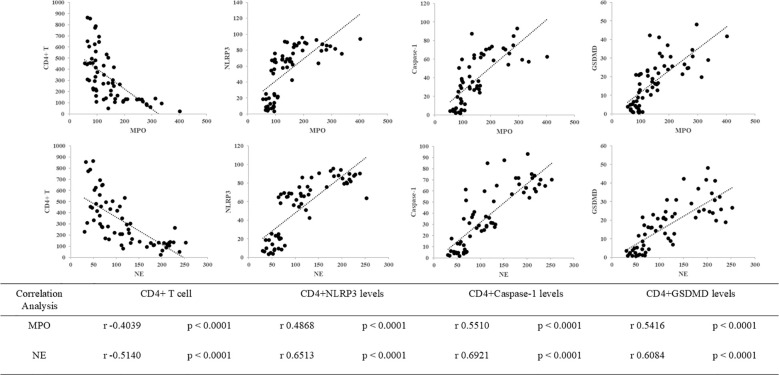 Figure 5
Figure 5| Characteristics | Non-SAL, n = 19 | SAL, n = 42 | p |
|---|---|---|---|
| Age, years | 61.6 (48.2 – 74.9) | 60.8 (43.4 – 78.2) | 0.8708 |
| Sex, n (%) |
|
|
|
| Infection site, n (%) | |||
| Bloodstream | 3 (15.8) | 6 (14.3) | 0.9999 |
| Lung | 10 (52.6) | 16 (38) | 0.5792 |
| Abdominal cavity | 7 (36.8) | 20 (45.2) | 0.2763 |
| Soft tissue | 3 (15.8) | 2 (4.8) | 0.1696 |
| Pathogen, n (%) | |||
| Gram-negative bacilus | 9 (47.4) | 27 (64.3) | 0.2659 |
| Gram-positive coccus | 6 (31.6) | 19 (50) | 0.5792 |
| Gram-positive bacilus | 2 (10.5) | 2 (4.8) | 0.5820 |
| Fungus | 3 (15.8) | 12 (28.6) | 0.3507 |
| PCT, ng/mL | 0.5 (0.2 – 2.0) | 5.4 (0.8 – 11.0) | 0.0964 |
| CRP, mg/L | 111.1 (32.4 – 189.9) | 172.3 (61.3 -283.4) | 0.0371* |
| 28-day mortality, n (%) | 0 (0) | 8 (19) | 0.0488* |
| ICU stay time, days | 2.0 (2.0 – 4.0) | 7.0 (3.0 – 9.8) | 0.0176* |
| APACHE II | 11.9 (5.3 – 18.5) | 17.5 (11.1 – 23.9) | 0.0176* |
| SOFA | 6.3 (2.4 – 10.2) | 9.0 (5.0 – 12.9) | 0.0201* |
| MV, n (%) | 13 (68.4) | 39 (92.3) | 0.0207* |
| CRRT, n (%) | 1 (5.3) | 12 (28.6) | 0.0474* |
| Creatinine, umol/L | 72 (51 – 106.5) | 76.5 (56.5 – 109.8) | 0.5998 |
| TBil, umol/L | 13.1 (9.7 – 18.7) | 16.0 (10.4 – 34.8) | 0.2334 |
| WBC, *10^9/L | 14.8 (7.0 – 22.7) | 13.0 (6.5 – 19.5) | 0.3526 |
| Neutrophil#, *10^6/L | 12.9 (5.7 – 20.1) | 11.9 (6.0 – 17.9) | 0.5846 |
| LY#, *10^6/L | 1568 (930 – 2208) | 572 (331 – 812) | <0.0001**** |
| CD4+ T#, *10^6/L | 544 (349 – 739) | 218 (81 – 355) | <0.0001**** |
| CD8+ T#, *10^6/L | 411 (92 – 731) | 139 (54 – 224) | <0.0001**** |
| IL-6, pg/mL | 78.2 (22.9 – 113.0) | 128.7 (36.9 – 559.1) | 0.1129 |
| IL-8, pg/mL | 45.5 (31.0 – 69.9) | 48.9 (28.9 – 135.3) | 0.2271 |
| IL-10, pg/mL | 6.5 (5.0 – 19.3) | 10.8 (5.2 – 19.7) | 0.5418 |
| TNFα, pg/mL | 11.1 (2.5 – 19.8) | 11.2 (2.5 – 18.6) | 0.5057 |
| MPO, ng/mL | 82.9 (67.6 – 98.1) | 176.2 (99.6 – 252.9) | <0.0001**** |
| NE, ng/mL | 56.3 (35.9 – 76.6) | 144.2 (86.9 – 201.6) | <0.0001**** |
| 95% CI for OR | ||||||
|---|---|---|---|---|---|---|
| Variable | B | SE | p | OR | Lower | Upper |
| Age | 0.0029 | 0.0164 | 0.8617 | 1.0029 | 0.9712 | 1.0356 |
| APACHE II | 0.1384 | 0.0520 | 0.0077 | 1.1485 | 1.0373 | 1.2716 |
| SOFA | 0.1532 | 0.0732 | 0.0363 | 1.1656 | 1.0099 | 1.3453 |
| MPO | 0.0862 | 0.0279 | 0.0020 | 1.0900 | 1.0320 | 1.1513 |
| NE | 0.0792 | 0.0238 | 0.0009 | 1.0824 | 1.0331 | 1.1341 |
| 95% CI for OR | ||||||
|---|---|---|---|---|---|---|
| Variable | B | SE | p | OR | Lower | Upper |
| APACHE II | 0.0568 | 0.1035 | 0.5832 | 1.0584 | 0.8641 | 1.2964 |
| SOFA | 0.1304 | 0.1616 | 0.4198 | 1.1393 | 0.8299 | 1.5639 |
| MPO | 0.0808 | 0.0402 | 0.0446 | 1.0841 | 1.0020 | 1.1730 |
| NE | 0.0526 | 0.0248 | 0.0339 | 1.0540 | 1.0040 | 1.1065 |
| Characteristics | Low neutrophil granule proteins, n = 31 | High neutrophil granule proteins, n = 30 | p |
|---|---|---|---|
| Age, years | 58.2 (41.5 – 74.9) | 64.0 (48.9 – 79.2) | 0.1656 |
| Sex, n (%) |
|
|
|
| Infection site, n (%) | |||
| Bloodstream | 5 (16.1) | 4 (13.3) | 0.9999 |
| Lung | 11 (35.5) | 15 (50.0) | 0.3056 |
| Abdominal cavity | 11 (35.5) | 16 (53.3) | 0.2016 |
| Soft tissue | 3 (9.7) | 2 (6.7) | 0.9999 |
| Pathogen, n (%) | |||
| Gram-negative bacilus | 14 (45.2) | 22 (73.3) | 0.0374* |
| Gram-positive coccus | 9 (29.0) | 16 (53.3) | 0.0707 |
| Gram-positive bacilus | 2 (6.5) | 2 (6.7) | 0.9999 |
| Fungus | 4 (12.9) | 11 (55.0) | 0.0402* |
| 28-day mortality, n (%) | 1 (3.2) | 7 (23.3) | 0.0261* |
| ICU stay time, days | 3.0 (2.0 – 8.5) | 6.0 (3.0 – 10.3) | 0.0451* |
| APACHE II | 13.2 (6.8 – 19.6) | 18.4 (11.9 – 24.9) | 0.0030** |
| SOFA | 6.5 (3.1 – 10.0) | 9.8 (5.7 – 13.9) | 0.0018** |
| MV, n (%) | 23 (74.2) | 29 (96.7) | 0.0261* |
| CRRT, n (%) | 3 (9.7) | 10 (33.3) | 0.0311* |
| PCT, ng/mL | 0.6 (0.3 – 2.7) | 6.8 (1.3 – 11.0) | 0.1588 |
| CRP, mg/L | 121.2 (35.9 – 206.5) | 186.4 (71.7 -301.0) | 0.0160* |
| WBC, *10^9/L | 11.9 (8.4 – 19.3) | 12.8 (8.5 – 14.9) | 0.5554 |
| LY#, *10^6/L | 1249 (598 – 1900) | 503 (276 – 484) | <0.0001**** |
| CD4+ T#, *10^6/L | 443 (230 – 655) | 192 (58 – 171) | <0.0001**** |
| CD8+ T#, *10^6/L | 320 (40 – 599) | 125 (41 – 126) | 0.0006*** |
| IL-6, pg/mL | 46.9 (17.5 – 113.0) | 276.0 (65.1 – 1000.0) | 0.0094** |
| IL-8, pg/mL | 35.7 (29.0 – 60.1) | 64.0 (38.0 – 145.0) | 0.0410* |
| IL-10, pg/mL | 7.4 (5.0 – 12.8) | 11.3 (5.2 – 29.6) | 0.2921 |
| TNFα, pg/mL | 9.5 (2.5 – 18.2) | 12.1 (2.5 – 18.9) | 0.7503 |
| Characteristics | Low neutrophil granule proteins, n = 31 | High neutrophil granule proteins, n = 30 | p |
|---|---|---|---|
| CD4+ T#, *10^6/L | 443 (230 – 655) | 192 (58 – 171) | <0.0001**** |
| CD4+NLRP3+, % | 31.3 (6.2 – 56.3) | 78.4 (65.9 – 90.9) | <0.0001**** |
| CD4+Caspase-1+, % | 19.4 (1.4 – 37.5) | 56.5 (36.6 – 76.5) | <0.0001**** |
| CD4+GSDMD+, % | 7.9 (0.9 – 14.9) | 26.5 (17.4 – 35.6) | <0.0001**** |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammasome and immune disorders · Streptococcal Infections and Treatments · Immune Response and Inflammation
Introduction
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection (1). In this dysregulated response, many immune mechanisms that are initially activated to protect host are harmful, on account of both excessive inflammation and immune suppression (2). The mechanistic underpinnings of concurrent immune suppression and relevant immune system changes in patients with sepsis still need further exploration.
Polymorphonuclear neutrophils are traditionally regarded as professional phagocytic and acute inflammatory cells that engulf the microbial pathogens (3). As an innate immune system response, antigen presentation triggers the adaptive immune system to activate cytotoxic T lymphocytes and induce B lymphocytes to secrete specific antibodies. Upon activation, neutrophils extruded their nuclear DNA and histones in association with the attached granule proteins to form neutrophil extracellular traps (NETs) to trap the environmental foreign invaders (4). However, granule proteins not only contribute to killing bacteria within the phagosome, but also are capable of inflicting tissue damage (5), which prompted us to explore the interaction of neutrophil granule proteins with adaptive immune cells and their contribution to sepsis-associated immunosuppression.
Pyroptosis is a type of programmed cell death mediated by caspase-dependent activation of members of the gasdermin family and inflammasome formation (6). In patients with sepsis, pyroptosis is observed in multiple immune cells (7). Our previous study revealed that a reduction in CD4^+^ T cells is central to the immunosuppression phase of sepsis and that the canonical pyroptosis pathway obliterates CD4^+^ T cells (8). NETs have already been verified to interact with the NLRP3 inflammasome in septic lung injury (9, 10). In this research, we aimed to explore the relationship between neutrophil granule proteins and sepsis-associated lymphopenia (SAL) and its interaction with CD4^+^ T-cell pyroptosis. We hypothesized that the level of neutrophil granule proteins may reflect the occurrence of SAL through the pyroptosis pathway of CD4^+^ T cells.
Materials and methods
Patients and study design
A prospective study was performed from May 2022 to October 2023 in the Department of Critical Care Medicine of Peking Union Medical College Hospital (PUMCH). The PUMCH institutional Ethic Committee approved this study (approval number JS-1170), and all patients enrolled in this study signed informed consent. The study was registered at the Chinese Clinical Trial Registry (ChiCTR-ROC-17010750).
The inclusion criteria were as follows: (1) ≥ 18 years old, (2) ICU (intensive care unit) stay time over 1 day, and (3) diagnosis of sepsis (see below). Patients had basic immunological diseases or malignant tumors were excluded. Sepsis was diagnosed according to the definition of the Third International Consensus (1); lymphopenia was diagnosed if the total lymphocyte count was < 1.1 × 10^9^/L according to the 2022 SAI expert consensus (11).
Outcome
Basic clinical evaluation and laboratory characteristics were collected on the first day of ICU admission. Basic clinical data, including age, sex, and basic information on immunological diseases and malignant tumors, were collected. Laboratory characteristics such as routine blood biochemistry, immunological parameters such as the peripheral blood lymphocyte count and lymphocyte subset counts, the SOFA (Sequential Organ Failure Assessment) score, and the APACHE (Acute Physiology and Chronic Health Evaluation) II score were recorded. Information on life-sustaining treatment, including the need for mechanical ventilation and renal replacement, was recorded. The follow-up data were 28-day mortality rate and ICU stay time.
Neutrophil granules can be divided into four groups according to the different maturation stages (12), and the levels of myeloperoxidase (MPO) and neutrophil elastase (NE) were measured as primary or azurophil granules. The NOD-like receptor family pyrin domain containing 3 (NLRP3) is a type of cytoplasmic pattern recognition receptor that may trigger inflammasome formation. NLRP3 was measured to evaluate the inflammasome and quantify pyroptosis in cells (13, 14). As the upstream canonical activation pathway of pyroptosis, the levels of NLRP3, Caspase-1 and gasdermin D (GSDMD) were measured gasdermin D (GSDMD) were measured (15).
Within 24 h of ICU admission, peripheral blood samples were collected. Blood sample was centrifuged immediately, and plasma was collected and stored at −80°C. Peripheral blood mononuclear cells (PBMCs) were purified by Ficoll density-gradient separation. Plasma and PBMCs were stored in the Clinical Biobank (ISO 20387: 2018) of Peking Union Medical College Hospital. The levels of MPO and NE were quantified by enzyme-linked immunosorbent assay (ELISA) (MPO: JL11580-96T Beijing China; NE: JL12352-96T Beijing China). For phenotypic staining, antibodies specific to CD4 (BioLegend, 980802, San Diego, CA), NLRP3 (Invitrogen, PA5-79740, Thermo Fisher Scientific, Inc.), Caspase-1 (Invitrogen, PA5-140994, Thermo Fisher Scientific, Inc.), and GSDMD (Invitrogen, PA5-119680, Thermo Fisher Scientific, Inc.) were used for surface staining of cells. Thawed PBMCs were resuspended and incubated with antibody under absolute dark conditions in room temperature. Having been washed by staining buffer, cells were fixed and permeabilized according to the instructions. The gating strategy of flow cytometry experiments is shown in Figure 1. Lymphocytes were gated on side scatter (SSC) and forward scatter (FSC). T cells (CD3^+^), CD4^+^, and CD8^+^ T-cell subsets were quantitated. Then, CD4^+^ lymphocytes were gated and immunoassayed with combinations of fluorochrome-conjugated antibodies, including NLRP3, Caspase-1, and GSDMD. The percentages of CD4^+^ lymphocytes expressing NLRP3, Caspase-1, and GSDMD and the MFI of these markers on CD4^+^ lymphocytes were further quantitated. A total of 10,000 cells were analyzed from each sample. The samples were analyzed through a BDCalibur flow cytometer (BD Biosciences) with FlowJo software (BD Biosciences).
*Comparison of pyroptosis biomarker levels, including NLRP3, Caspase-1, and GSDMD in groups with different neutrophil granule protein levels. ***p < 0.0001 (A) Comparison of percentage of NLRP3+ CD4+ T cells, percentage of Caspase-1+ CD4+ T cells, and percentage of GSDMD+ CD4+ T cells between patients with low neutrophil granule protein level and high neutrophil granule protein level. (B) Representative flow dot plots of the lymphocyte gating strategy of the lymphocyte, CD4+ T cell, NLRP3 MFI on CD4+ T cells, Caspase-1 MFI on CD4+ T cells, and GSDMD MFI on CD4+ T cells in patients with low neutrophil granule protein level. (C) Representative flow dot plots of the lymphocyte gating strategy of the lymphocyte, CD4+ T cell, NLRP3 MFI on CD4+ T cells, Caspase-1 MFI on CD4+ T cells, and GSDMD MFI on CD4+ T cells in patients with high neutrophil granule protein level.
Statistical analysis
Normally distributed data are shown as the mean with standard deviation and were analyzed with Student’s t-test. Nonnormally distributed data are expressed as the median and interquartile range and were compared through the Mann–Whitney U test. Categorical variables are recorded as proportions and were analyzed by the chi-square test. Logistic regression was performed to identify parameters with predictive value for SAL risk. Statistically significant variables were subsequently analyzed using a multi-logistic regression, and the results were expressed as P and odds ratio (OR) with 95% confidence interval (CI). The value of neutrophil granule proteins for SAL risk prediction was calculated via ROC (receiver operating characteristic) curve analysis with the Hanley–McNeil test. The area under the curves (AUCs) were examined to determine a cutoff level to predict SAL occurrence. Based on the cutoff level, all the patients were divided into a low neutrophil granule protein group and a high neutrophil granule protein group. Pearson’s correlation analysis was performed for the detection of correlation between neutrophil granule proteins and expression levels of pyroptosis markers on CD4^+^ T cells. Statistical analyses were performed with the SPSS 13.0 software package (SPSS, Chicago, USA).
Results
Basic characteristics of study population in SAL and non-SAL groups
From May 2022 to October 2023, 107 patients admitted to the Critical Care Medicine Department of PUMCH were diagnosed with sepsis. Among these patients, 25 who did not meet the inclusion criteria (4 were < 18 years old and 21 were discharged within 24 h) were excluded, 12 patients had basic immunological diseases or malignant tumors, 6 refused to sign the informed consent, and 3 had withdrawn. A total of 61 patients were enrolled in this research, 42 of whom met the criteria for lymphopenia (Figure 2).
Flowchart of patients included in the study.
Basic clinical characteristics after ICU admission were compared between patients with or without SAL (non-SAL group vs. SAL group), as shown in Table 1. Age of patients between the different groups was accordant, and the majority of patients were male. Infection sources were similar in patients with SAL and those without SAL. The level of C-reactive protein in the SAL group (111.1 vs. 172.3 mg/L, p = 0.0371), but not the level of procalcitonin, was significantly greater. The mortality (0 vs. 19%, p = 0.0488), ICU stay time (2 vs. 7 days, p = 0.0176), SOFA score (6.3 vs. 9.0, p = 0.0201), APACHE II score (11.9 vs. 17.5, p = 0.0176), and need for mechanical ventilation (68.4 vs. 92.3%, p = 0.0207) and renal replacement (5.3 vs. 28.6%, p = 0.0474) were significantly greater in the SAL group than in the control group. No significant difference in white blood cell count was shown between the groups.
In terms of the lymphocyte counts and their subsets, the lymphocyte count (1,568 vs. 572 × 10^6^/L, p < 0.0001) and CD4^+^ T-cell (544 vs. 218 × 10^6^/L, p < 0.0001) and CD8^+^ T-cell counts (411 vs. 139 × 10^6^/L, p < 0.0001) were significantly lower in the SAL group. The levels of neutrophil granule proteins, including MPO (82.9 vs. 175.3, p < 0 <.0001) and NE (56.3 vs. 144.2, p < 0 <.0001), were significantly higher in the SAL group, as shown in Figure 3. In summary, patients with SAL showed significantly higher levels of neutrophil granule proteins.
*Comparison of neutrophil granule protein levels, including MPO (A) and NE (B) in groups of patients with sepsis with or without lymphopenia. ***p < 0.0001. SAL, sepsis-associated lymphopenia.
Neutrophil granule protein levels are a risk factor for lymphopenia in patients with sepsis
Lymphopenia risk in patients with sepsis was examined by univariate logistic regression analysis (Table 2). Among them, the variables SOFA score, APACHE II score, MPO, and NE were associated with lymphopenia risk in patients with sepsis. After further adjustment by multivariate logistic regression analysis, the OR of MPO after adjustment was 1.0841 (95% CI, 1.0020–1.1730, p = 0.0446), and the OR of NE after adjustment was 1.0540 (95% CI, 1.0040–1.1065, p = 0.0339) (Table 3). To further determine the value of neutrophil granule proteins for SAL risk prediction in patients with sepsis, ROC curve analysis was generated. The area under the ROC curve for the prediction of SAL occurrence of MPO was 0.939 (95% CI, 0.846–0.984; p < 0.0001), and that of NE was 0.950 (95% CI, 0.862–0.989; p < 0.0001) (Figure 4).
Receiver operating characteristic curve of MPO (A) and NE (B) for the prediction of SAL occurrence. MPO, myeloperoxidase; NE, neutrophil elastase.
Clinical features of patients with sepsis with different neutrophil granule protein levels
Based on the cutoff level of neutrophil granule proteins in ROC curve analysis, all the patients were divided into a low neutrophil granule protein group and a high neutrophil granule protein group, with high levels of both MPO and NE. Table 4 shows the clinical characteristics of patients in the different neutrophil granule protein groups. Age, sex, and infection site were in agreement between the groups. Gram-negative bacilli (73.3% vs. 45.2%, p = 0.0374) and fungi (55.0% vs. 12.9%, p = 0.0402) were more prevalent in the high neutrophil granule protein level group. The mortality (23.3% vs. 3.2%, p = 0.0261), ICU stay time (6.0 vs. 3.0, p = 0.0451), APACHE II score (18.4 vs. 13.2, p = 0.0030), and SOFA score (9.8 vs. 6.5, p = 0.0018) were significantly greater in the high neutrophil granule protein level group than in the low neutrophil granule protein level group. Both the need for mechanical ventilation (96.7% vs. 74.2%, p = 0.0261) and the need for renal replacement (33.3% vs. 9.7%, p = 0.0311) were significantly greater in the high neutrophil granule protein level group. The levels of inflammatory biomarkers, such as CRP (186.4 vs. 121.2, p = 0.0160), IL-6 (276.0 vs. 46.9, p = 0.0094), and IL-8 (64.0 vs. 35.7, p = 0.0410) were significantly different in the groups with different neutrophil granule protein levels. Lower lymphocyte counts and subset cell counts were seen in patients with high neutrophil granule protein levels. Overall, patients with sepsis with high neutrophil granule protein levels had worse outcomes and experienced longer ICU stay times and more severe organ dysfunction.
Levels of biomarkers of pyroptosis in CD4+ T cells were associated with neutrophil granule protein levels in patients with sepsis
Biomarkers of pyroptosis in CD4^+^ T cells were evaluated in groups with different neutrophil granule protein levels. The level of NLRP3 [78.4 (65.9–90.9) vs. 31.3 (6.2–56.3), p < 0.0001^^] was significantly higher in the high neutrophil granule protein level group, and the levels of the components of its subsequent pathway, Caspase-1 [56.2 (36.0–76.4) vs. 19.4 (1.4–37.5), p < 0.0001^^] and GSDMD [26.5 (17.4–35.6) vs. 7.9 (0.9–14.9), p < 0 <.0001^****^], were higher in the high neutrophil granule protein level group (shown in Figure 1, Table 5).
Relationships among neutrophil granule proteins, CD4+ T cells, and pyroptosis
We hypothesized that neutrophil granule proteins, CD4^+^ T cells, and pyroptosis interact closely in the mechanism underlying SAL. Consistent with this hypothesis, Pearson’s correlation analysis revealed significant correlations between MPO levels and CD4^+^ T cells (r = −0.4039, p < 0.0001), CD4^+^NLRP3 levels (r = 0.4868, p < 0.0001), CD4^+^Caspase-1 levels (r = 0.5510, p < 0.0001), and CD4^+^GSDMD levels (r = 0.5416, p < 0.0001), as well as between NE levels and CD4^+^ T cells (r = −0.5140, p < 0.0001), CD4^+^NLRP3 levels (r = 0.6513, p < 0.0001), CD4^+^Caspase-1 levels (r = 0.6921, p = 0.0002), and CD4^+^GSDMD levels (r = 0.6084, p < 0.0001) (Figure 5). A significant relationship between neutrophil granule proteins and the pyroptosis pathway of CD4^+^ T cells was revealed.
Correlations between neutrophil granule protein level (including MPO and NE), CD4+ T cells, and pyroptosis biomarkers (including NLRP3, Caspase-1, and GSDMD) in patients with sepsis. The correlation between MPO levels and CD4+ T cells (r = −0.4039, p < 0.0001), MPO levels and CD4+NLRP3 levels (r = 0.4868, p < 0.0001), MPO levels and CD4+Caspase-1 levels (r = 0.5510, p < 0.0001), and MPO levels and CD4+GSDMD levels (r = 0.5416, p < 0.0001). The correlation between NE levels and CD4+ T cells (r = −0.5140, p < 0.0001), NE levels and CD4+NLRP3 levels (r = 0.6513, p < 0.0001), NE levels and CD4+Caspase-1 levels (r = 0.6921, p = 0.0002), and NE levels and CD4+GSDMD levels (r = 0.6084, p < 0.0001).
Discussion
Our study first evaluated the role of plasma neutrophil granule protein level in patients with SAL. To explore the relationship between neutrophil granule proteins and SAL, we evaluated the levels of plasma neutrophil granule proteins within 24 h after admission. We found that higher plasma neutrophil granule protein levels showed close relationship with the incidence of lymphopenia in patients with sepsis. Moreover, patients with sepsis with high neutrophil granule protein levels had lower CD4^+^ T lymphocyte counts and higher levels of biomarkers of pyroptosis. The significant correlation between neutrophil granule proteins and CD4^+^ T-cell counts and levels of biomarkers of pyroptosis revealed that plasma neutrophil granule proteins may play a role in SAL through the pyroptosis pathway of CD4^+^ T cells.
Immunosuppressive changes, often implicated in increased susceptibility to secondary infections (16, 17), are a main cause of overall mortality of patients with sepsis (18). The immune system is composed of the innate and the adaptive immune system. Research over the last decade has documented neutrophil heterogeneity and functional versatility far beyond their antimicrobial function (19). Emerging evidence indicates that neutrophils utilize granule proteins to interact with innate and adaptive immune cells and regulate the inflammatory response. Our study explored that patients with SAL had higher plasma neutrophil granule protein levels than controls did. Neutrophil granule proteins were independently associated with lymphopenia risk (MPO: OR = 1.0841, 95% CI, 1.0020–1.1730, p = 0.0446; NE: OR = 1.0540, 95% CI, 1.0040–1.1065, p = 0.0339). The area under the ROC curve in predicting SAL occurrence for MPO was 0.939 (95% CI, 0.846–0.984; p < 0.0001), whereas that for NE was 0.950 (95% CI, 0.862–0.989; p < 0.0001). Overall, patients with sepsis with high neutrophil granule protein levels had longer ICU stays and higher mortality, more severe organ dysfunction, and frequent need for organ support. Our study firstly explored the effects of neutrophil granule proteins in patients with sepsis with lymphopenia.
Different cell types and characteristics were involved in immunosuppression in patients with sepsis. A major reason for immunosuppression in sepsis is the depletion of immune cells (20, 21). Notably, the abnormal quantity and function of CD4^+^ T cells cannot be ignored in the development and progression of immunosuppression (22). Previous research has shown that NETs may interact with adaptive immune cells through different pathways (23, 24). In our study, patients with high neutrophil granule proteins had significantly fewer CD4^+^ T cells [192 (58–171) vs. 443 (230–655), p < 0 <.0001]. Neutrophil granule proteins were closely related to the CD4^+^ T-cell count (MPO vs. CD4^+^ T-cell count, r = −0.4039, p < 0.0001; NE vs. CD4^+^ T-cell count, r = −0.5140, p < 0.0001). In addition to traditional signal transduction between the innate and adaptive immune system (21, 25), the connections between neutrophil granule proteins and T lymphocytes deserve further exploration.
As a type of programmed cell death discovered in recent years, pyroptosis of immune cell in sepsis is complicated (26). A protective role in sepsis was initially thought with the downregulation of inflammation, but an increasing number of studies have demonstrated the disadvantages of excessive pyroptosis (27, 28). Observational study findings have suggested that the NLRP3 inflammasome may drive post-septic immunosuppression (29, 30). Our previous study verified that canonical pyroptosis is an important mechanism underlying CD4^+^ T-cell lymphocytopenia during sepsis (8, 31). In this study, biomarkers of CD4^+^ T-cell pyroptosis were evaluated in groups with different neutrophil granule protein levels. Levels of NLRP3 [78.4 (65.9–90.9) vs. 31.3 (6.2–56.3), p < 0.0001], Caspase-1 [56.2 (36.0–76.4) vs. 19.4 (1.4–37.5), p < 0.0001], and GSDMD [26.5 (17.4–35.6) vs. 7.9 (0.9–14.9), p < 0 <.0001] were significantly higher in the high neutrophil granule protein level group. Neutrophil granule proteins are closely related to CD4^+^ T-cell pyroptosis. We hypothesize that neutrophil granule proteins may participate in SAL through CD4^+^ T-cell pyroptosis.
The impact of neutrophil granule proteins on immune responses is largely implicated in APC T-cell immunity. MPO can modulate immune responses by either CD4^+^ T -cell activation or dendritic cell suppression, and elastase can potentially promote Th17 response but simultaneously induces DC production of TGF-β for suppressing T-cell proliferation (32, 33). Our study first explored crosstalk between neutrophil granule proteins and the pyroptosis pathway of CD4^+^ T cells. Neutrophil granule proteins have been identified as important modulators of neutrophil trafficking, reverse transendothelial migration, phagocytosis, neutrophil life span, NET formation, efferocytosis, cytokine activity, and autoimmunity (5). Based on recent studies, NETs may interact with pyroptosis signal pathway through different approaches. Increased NETs may induce expression of pyroptosis-related proteins and promote NLRP3 inflammasome activation (9, 10). The STING/IRE1α signaling pathway or the NF-κB/caspase 3/GSDME axis may contribute to the process (34, 35). However, the complex regulatory mechanisms in sepsis are still worth exploring.
There are still several limitations in our study. As a single-center study, it may limit the generalizability of the results. Relatively small sample and complex confounders may lower the credibility of the results. A larger sample size or larger multicenter studies should be considered. Second, although the correlation between neutrophil granule proteins and CD4^+^ T-cell pyroptosis was identified in this research, the causal relationship still requires further basic studies. More than that, immunosuppression is a complex status that may change during different courses of disease. In our study, we only collected blood samples within 24 h after being admitted, and a dynamic analysis of neutrophil granule proteins may be worthy of further study. Finally, neutrophil granule protein detections still have several limitations because plasma neutrophil granule proteins can be induced by different mechanisms like neutrophil degranulation, necroptosis, pyroptosis, or NETosis. Further animal experiments are still needed to explore detailed mechanisms.
Conclusion
Increased levels of neutrophil granule proteins were significantly associated with SAL incidence, and a significant relationship between neutrophil granule proteins and the pyroptosis pathway of CD4^+^ T cells was revealed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singer M Deutschman CS Seymour CW Shankar-Hari M Annane D Bauer M. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. (2016) 315:801–10. doi: 10.1001/jama.2016.0287 PMC 496857426903338 · doi ↗ · pubmed ↗
- 2van der Poll T Shankar-Hari M Wiersinga WJ. The immunology of sepsis. Immunity. (2021) 54:2450–64. doi: 10.1016/j.immuni.2021.10.012 34758337 · doi ↗ · pubmed ↗
- 3Tsai CY Hsieh SC Liu CW Lu CS Wu CH Liao HT. Cross-Talk among Polymorphonuclear Neutrophils, Immune, and Non-Immune Cells via Released Cytokines, Granule Proteins, Microvesicles, and Neutrophil Extracellular Trap Formation: A Novel Concept of Biology and Pathobiology for Neutrophils. Int J Mol Sci. (2021) 22(6):3119. doi: 10.3390/ijms 22063119 33803773 PMC 8003289 · doi ↗ · pubmed ↗
- 4Brinkmann V Reichard U Goosmann C Fauler B Uhlemann Y Weiss DS. Neutrophil extracellular traps kill bacteria. Science. (2004) 303:1532–5. doi: 10.1126/science.1092385 15001782 · doi ↗ · pubmed ↗
- 5Othman A Sekheri M Filep JG. Roles of neutrophil granule proteins in orchestrating inflammation and immunity. FEBS J. (2022) 289:3932–53. doi: 10.1111/febs.v 289.14 PMC 954610633683814 · doi ↗ · pubmed ↗
- 6Vigneron C Py BF Monneret G Venet F. The double sides of NLRP 3 inflammasome activation in sepsis. Clin Sci (Lond). (2023) 137:333–51. doi: 10.1042/CS 20220556 36856019 · doi ↗ · pubmed ↗
- 7Liu D Huang SY Sun JH Zhang HC Cai QL Gao C. Sepsis-induced immunosuppression: mechanisms, diagnosis and current treatment options. Mil Med Res. (2022) 9:56. doi: 10.1186/s 40779-022-00422-y 36209190 PMC 9547753 · doi ↗ · pubmed ↗
- 8Guo R Zhao G Bai G Chen J Han W Cui N. Depletion of m TOR ameliorates CD(4)(+) T cell pyroptosis by promoting autophagy activity in septic mice. Int Immunopharmacol. (2023) 124:110964. doi: 10.1016/j.intimp.2023.110964 37738689 · doi ↗ · pubmed ↗