Key capabilities required for podiatry graduates: A Delphi consensus study
Shannon E. Munteanu, Matthew Cotchett, Matthew J. Oates, Nicoletta Frescos, Vivienne Chuter, Mike Frecklington, Marie T. Butler, Nick W. Haley, Hylton B. Menz

TL;DR
This study identifies key skills needed for podiatry graduates by reaching consensus among employers using a Delphi method.
Contribution
The study establishes a set of employer-validated capabilities for podiatry graduates through a modified Delphi survey.
Findings
Sixty-one items across seven domains achieved consensus among employers.
Thirty-nine of these items were rated as 'essential' for podiatry graduates.
The findings can inform the development of a work-readiness tool for podiatry education.
Abstract
Work‐readiness is linked to health professional graduates' job performance, satisfaction, engagement and retention. However, there is currently no podiatry‐specific graduate employer work‐readiness survey tool that has been developed with employers of graduate podiatrists. The aim of this study was to conduct a modified Delphi survey to achieve consensus among employers of podiatry graduates on the key capabilities required for podiatry graduates. A Delphi method of consensus development was used, comprising three online survey rounds. Purposive sampling was used to recruit individuals with extensive experience and knowledge in mentoring and managing graduate podiatrists in Australia or New Zealand. In Round 1, participants were asked to rate agreement/disagreement with 71 items across seven domains relating to capabilities required of podiatry graduates that were extracted from a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
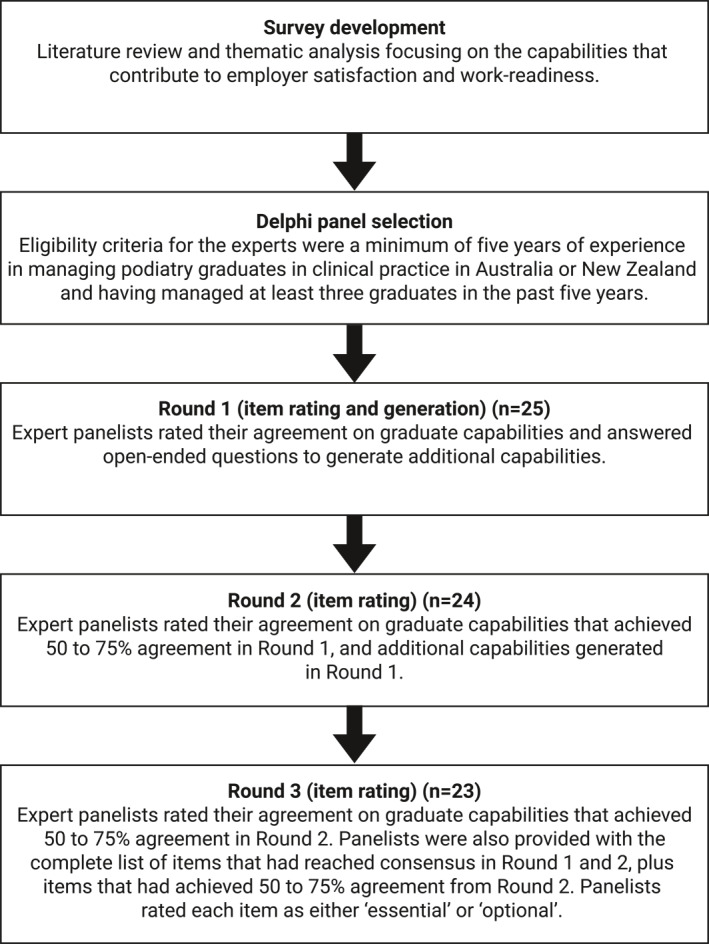 FIGURE 1
FIGURE 1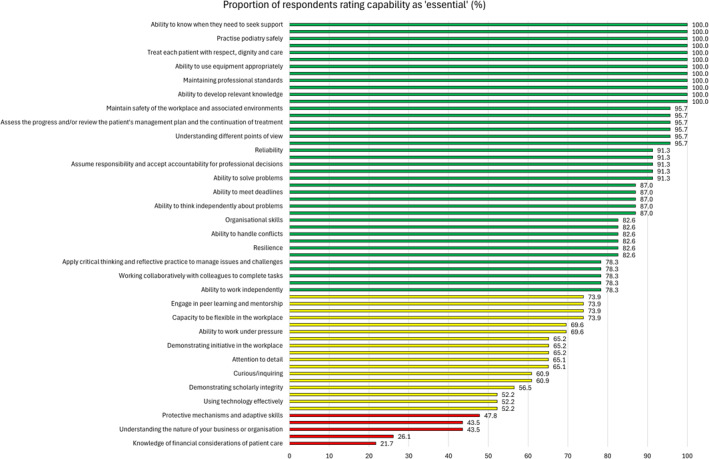 FIGURE 2
FIGURE 2| Participant characteristics | Values |
|---|---|
| Age, mean ± SD (years) | 46.1 ± 7.6 |
| Female gender, | 13 (52) |
| Female sex, | 13 (52) |
| Country of birth, | |
| Australia | 19 (76) |
| New Zealand | 4 (16) |
| Sri Lanka | 1 (4) |
| South Korea | 1 (4) |
| Ethnicity, | |
| Central Asian | 1 (4) |
| North‐West European | 9 (36) |
| North‐East Asian | 2 (8) |
| Oceanian | |
| Australian peoples | |
| Australian | 9 (36) |
| Australian Aboriginal | 0 (0) |
| Australian South Sea Islander | 0 (0) |
| Torres Strait Islander | 0 (0) |
| Norfolk Islander | 0 (0) |
| New Zealand Peoples | |
| Māori | 0 (0) |
| New Zealander | 2 (8) |
| Southern and Eastern European | 2 (8) |
| Principal location of clinical practice, | |
| Australia | 21 (84) |
| New South Wales | 2 (8) |
| Northern Territory | 2 (8) |
| Queensland | 3 (12) |
| South Australia | 4 (16) |
| Tasmania | 1 (4) |
| Victoria | 7 (28) |
| Western Australia | 2 (8) |
| New Zealand | 4 (16) |
| Auckland | 2 (8) |
| Canterbury | 1 (4) |
| Wellington | 1 (4) |
| Primary work sector as manager of graduates, | |
| Private | 19 (76%) |
| Public | 6 (24%) |
| Number of years managing podiatry graduates in clinical practice, mean ± SD | 14.9 ± 5.7 |
| Total number of podiatry graduates that have been managed, mean ± SD | 12.1 ± 5.8 |
| Total number of podiatry graduates managed over the past 5 years (2019 onwards), mean ± SD | 5.0 ± 2.3 |
| Capability | Consensus achieved | Round 1 ( | Round 2 ( | Round 3 ( |
|---|---|---|---|---|
| Generic capabilities: Foundation capabilities (general literacy, numeracy, and communication skills and the ability to investigate and integrate knowledge) | ||||
| Oral communication skills | Yes | 24 (96.0) | ||
| Written communication skills | Yes | 21 (84.0) | ||
| Numeracy skills | Yes | 17 (68.0) | 22 (91.7) | |
| Ability to develop relevant knowledge | Yes | 22 (88.0) | ||
| Ability to develop relevant skills | Yes | 24 (96.0) | ||
| Ability to solve problems | Yes | 22 (88.0) | ||
| Ability to integrate knowledge | Yes | 22 (88.0) | ||
| Ability to think independently about problems | Yes | 19 (76.0) | ||
| Generic capabilities: Adaptive capabilities (the ability to adapt and apply skills/knowledge and work independently) | ||||
| Broad background knowledge | Yes | 19 (79.2) | ||
| Ability to develop innovative ideas | No | 8 (33.3) | ||
| Ability to identify new opportunities | No | 8 (33.3) | ||
| Ability to adapt knowledge to different contexts | Yes | 17 (70.8) | 23 (95.8) | |
| Ability to apply skills in different contexts | Yes | 20 (83.3) | ||
| Ability to work independently | Yes | 20 (83.3) | ||
| Protective mechanisms and adaptive skills | Yes | 15 (62.5) | 20 (83.3) | |
| Resilience | Yes | 15 (62.5) | 17 (70.8) | 20 (87.0) |
| Generic capabilities: Collaborative capabilities (teamwork and interpersonal skills) | ||||
| Working well in a team | Yes | 21 (87.5) | ||
| Getting on well with others in the workplace | Yes | 21 (87.5) | ||
| Working collaboratively with colleagues to complete tasks | Yes | 22 (91.7) | ||
| Understanding different points of view | Yes | 20 (83.3) | ||
| Ability to interact with coworkers from different or multicultural backgrounds | Yes | 21 (87.5) | ||
| Ability to handle conflicts | Yes | 16 (66.7) | 22 (91.7) | |
| Generic capabilities: Technical capabilities (application of professional and technical knowledge and standards) | ||||
| Applying professional knowledge to job tasks | Yes | 23 (95.8) | ||
| Using technology effectively | Yes | 23 (95.8) | ||
| Applying technical skills in the workplace | Yes | 22 (91.7) | ||
| Maintaining professional standards | Yes | 21 (87.5) | ||
| Observing ethical standards | Yes | 23 (95.8) | ||
| Using research skills to gather evidence | Yes | 17 (70.8) | 20 (83.3) | |
| Demonstrating scholarly integrity | Yes | 16 (66.7) | 21 (87.5) | |
| Ability to use equipment appropriately | Yes | 20 (83.3) | ||
| Generic capabilities: Employability capabilities (the ability to perform and innovate in the workplace) | ||||
| Ability to work under pressure | Yes | 13 (54.2) | 19 (82.6) | |
| Capacity to be flexible in the workplace | Yes | 18 (75.0) | 22 (95.7) | |
| Ability to meet deadlines | Yes | 17 (70.8) | 19 (82.6) | |
| Understanding the nature of your business or organisation | Yes | 17 (70.8) | 21 (91.3) | |
| Demonstrating leadership skills | No | 4 (16.7) | ||
| Demonstrating management skills | No | 3 (12.5) | ||
| Taking responsibility for personal professional development | Yes | 13 (54.2) | 21 (91.3) | |
| Demonstrating initiative in the workplace | Yes | 14 (58.3) | 20 (87.0) | |
| Confident | Yes | 14 (58.3) | 18 (78.3) | |
| Marketing knowledge and skills | No | 4 (16.7) | ||
| Motivated | Yes | 19 (79.2) | ||
| Administration knowledge and skills | No | 7 (29.2) | ||
| Client service knowledge and skills | Yes | 12 (50.0) | 18 (78.3) | |
| Organisational skills | Yes | 17 (70.8) | 17 (73.9) | 21 (91.3) |
| Maturity | No | 13 (54.2) | 13 (56.5) | 15 (65.2) |
| Systems thinking (ability to have a broader perspective and see the larger picture) | No | 9 (37.5) | ||
| Self‐management (career and life) | No | 12 (50.0) | 15 (65.2) | 13 (56.5) |
| Hard working | Yes | 17 (70.8) | 19 (82.6) | |
| Podiatry‐specific capabilities (the knowledge, skills, and professional attributes needed to safely and competently practice as a podiatrist or podiatric surgeon in Australia | ||||
| Use pharmaceutical products safely and effectively within own scope of practice | Yes | 21 (87.5) | ||
| Assess the progress and/or review the patient's management plan and the continuation of treatment | Yes | 21 (87.5) | ||
| Practice in an ethical and professional manner, consistent with relevant legislative and regulatory requirements | Yes | 24 (100.0) | ||
| Treat each patient with respect, dignity and care | Yes | 24 (100.0) | ||
| Assume responsibility and accept accountability for professional decisions | 20 (83.3) | |||
| Advocate on behalf of the patient when appropriate | Yes | 21 (87.5) | ||
| Seek opportunities to progress the profession for the benefit of the community | No | 11 (45.8) | ||
| Communicate clearly, effectively, empathetically and appropriately with the patient and their family or carers | Yes | 20 (83.3) | ||
| Communicate and collaborate with the patient, members of the patient's healthcare team and relevant others | Yes | 20 (83.3) | ||
| Examine and reflect on how one's own culture influences perceptions and interactions with others from different cultures | No | 14 (58.3) | 13 (56.5) | 15 (65.2) |
| Apply critical thinking and reflective practice to manage issues and challenges | Yes | 16 (66.7) | 21 (91.3) | |
| Identify ongoing professional learning needs and opportunities | Yes | 18 (75.0) | 20 (87.0) | |
| Engage in peer learning and mentorship | Yes | 19 (79.2) | ||
| Practice podiatry safely | Yes | 24 (100.0) | ||
| Protect and enhance patient safety | Yes | 22 (91.7) | ||
| Regularly implement quality assurance processes to improve patient care | No | 12 (50.0) | 14 (60.9) | 13 (56.5) |
| Maintain safety of the workplace and associated environments | Yes | 19 (79.2) | ||
| Other capabilities | ||||
| Knowledge of environmental issues | No | 8 (33.3) | ||
| Knowledge of financial considerations of patient care | Yes | 12 (50.0) | Missing data | 19 (82.6) |
| Knowledge of political issues | No | 1 (4.2) | ||
| Knowledge of economic issues | No | 2 (8.3) | ||
| Personal presentation and grooming | Yes | 20 (83.3) | ||
| Display a positive self‐concept | Yes | 20 (83.3) | ||
| Additional capabilities identified in Round 1 | ||||
| Attention to detail | Yes | NA | 20 (87.9) | |
| Ability to provide and receive feedback | Yes | NA | 20 (87.9) | |
| Ability to know when they need to seek support | Yes | NA | 21 (91.3) | |
| Curious/inquiring | Yes | NA | 18 (78.3) | |
| Loyalty | No | NA | 10 (43.5) | |
| Reliability | Yes | NA | 20 (87.5) | |
| Transparency | No | NA | 14 (60.9) | 15 (65.2) |
| Capability | Essential, | Optional, |
|---|---|---|
| Generic capabilities: Foundation capabilities (general literacy, numeracy, and communication skills and the ability to investigate and integrate knowledge) | ||
| Oral communication skills | 23 (100.0) | 0 (0.0) |
| Written communication skills | 22 (95.7) | 1 (4.3) |
| Numeracy skills | 12 (52.2) | 11 (47.8) |
| Ability to develop relevant knowledge | 23 (100.0) | 9 (0.0) |
| Ability to develop relevant skills | 23 (100.0) | 0 (0.0) |
| Ability to solve problems | 21 (91.3) | 2 (8.7) |
| Ability to integrate knowledge | 20 (87.0) | 3 (13.0) |
| Ability to think independently about problems | 20 (87.0) | 3 (13.0) |
| Generic capabilities: Adaptive capabilities (the ability to adapt and apply skills/knowledge and work independently) | ||
| Broad background knowledge | 6 (26.1) | 17 (73.9) |
| Ability to adapt knowledge to different contexts | 19 (82.6) | 4 (17.4) |
| Ability to apply skills in different contexts | 20 (87.0) | 3 (13.0) |
| Ability to work independently | 18 (78.3) | 5 (21.7) |
| Protective mechanisms and adaptive skills | 11 (47.8) | 12 (52.2) |
| Resilience | 19 (82.6) | 4 (17.4) |
| Generic capabilities: Collaborative capabilities (teamwork and interpersonal skills) | ||
| Working well in a team | 15 (65.2) | 8 (34.8) |
| Getting on well with others in the workplace | 18 (78.3) | 5 (21.7) |
| Working collaboratively with colleagues to complete tasks | 18 (78.3) | 5 (21.7) |
| Understanding different points of view | 22 (95.7) | 1 (4.3) |
| Ability to interact with co‐workers from different or multi‐cultural backgrounds | 19 (82.6) | 4 (17.4) |
| Ability to handle conflicts | 19 (82.6) | 4 (17.4) |
| Generic capabilities: Technical capabilities (application of professional and technical knowledge and standards) | ||
| Applying professional knowledge to job tasks | 22 (95.7) | 1 (4.3) |
| Using technology effectively | 12 (52.2) | 11 (47.8) |
| Applying technical skills in the workplace | 19 (82.6) | 4 (17.4) |
| Maintaining professional standards | 23 (100.0) | 0 (0.0) |
| Observing ethical standards | 23 (100.0) | 0 (0.0) |
| Using research skills to gather evidence | 12 (52.2) | 11 (47.8) |
| Demonstrating scholarly integrity | 13 (56.5) | 10 (43.5) |
| Ability to use equipment appropriately | 23 (100.0) | 0 (0.0) |
| Generic capabilities: Employability capabilities (the ability to perform and innovate in the workplace) | ||
| Ability to work under pressure | 16 (69.6) | 7 (30.4) |
| Capacity to be flexible in the workplace | 17 (73.9) | 6 (26.1) |
| Ability to meet deadlines | 20 (87.0) | 3 (13.0) |
| Understanding the nature of your business or organisation | 10 (43.5) | 13 (56.5) |
| Taking responsibility for personal professional development | 20 (87.0) | 3 (13.0) |
| Demonstrating initiative in the workplace | 15 (65.2) | 8 (34.8) |
| Confident | 10 (43.5) | 13 (56.5) |
| Motivated | 18 (78.3) | 5 (21.7) |
| Client service knowledge and skills | 15 (65.2) | 8 (34.8) |
| Organisational skills | 19 (82.6) | 4 (17.4) |
| Hard working | 15 (65.2) | 8 (34.8) |
| Podiatry‐specific capabilities (the knowledge, skills, and professional attributes needed to safely and competently practice as a podiatrist or podiatric surgeon in Australia | ||
| Use pharmaceutical products safely and effectively within own scope of practice | 21 (91.3) | 2 (8.7) |
| Assess the progress and/or review the patient's management plan and the continuation of treatment | 22 (95.7) | 1 (4.3) |
| Practice in an ethical and professional manner, consistent with relevant legislative and regulatory requirements | 23 (100.0) | 0 (0.0) |
| Treat each patient with respect, dignity and care | 23 (100.0) | 0 (0.0) |
| Assume responsibility and accept accountability for professional decisions | 21 (91.3) | 2 (8.7) |
| Advocate on behalf of the patient when appropriate | 16 (69.6) | 7 (30.4) |
| Communicate clearly, effectively, empathetically, and appropriately with the patient and their family or carers | 23 (100.0) | 0 (0.0) |
| Communicate and collaborate with the patient, members of the patient's healthcare team and relevant others | 22 (95.7) | 1 (4.3) |
| Apply critical thinking and reflective practice to manage issues and challenges | 18 (78.3) | 5 (21.7) |
| Identify ongoing professional learning needs and opportunities | 17 (73.9) | 6 (26.1) |
| Engage in peer learning and mentorship | 17 (73.9) | 6 (26.1) |
| Practice podiatry safely | 23 (100.0) | 0 (0.0) |
| Protect and enhance patient safety | 23 (100.0) | 0 (0.0) |
| Maintain safety of the workplace and associated environments | 22 (95.7) | 1 (4.3) |
| Other capabilities | ||
| Knowledge of financial considerations of patient care | 5 (21.7) | 18 (78.3) |
| Personal presentation and grooming | 17 (73.9) | 6 (26.1) |
| Display a positive self‐concept | 14 (60.9) | 9 (39.1) |
| Additional capabilities identified in round 1 | ||
| Attention to detail | 15 (65.2) | 8 (34.8) |
| Ability to provide and receive feedback | 21 (91.3) | 2 (8.7) |
| Ability to know when they need to seek support | 23 (100.0) | 0 (0.0) |
| Curious/inquiring | 14 (60.9) | 9 (39.1) |
| Reliability | 21 (91.3) | 2 (8.7) |
- —Australian Podiatry Education and Research Foundation 10.13039/501100022909
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDelphi Technique in Research · Global Health Workforce Issues
INTRODUCTION
1
Work‐readiness is defined as the extent to which graduates are perceived to possess the attitudes and attributes essential for success in the workplace [1]. In healthcare professions, work‐readiness is linked to health professional graduates' job performance, satisfaction, engagement, and retention [2]. Consequently, education providers in healthcare, including those offering podiatry programs, must ensure their curricula align with employer expectations for work‐ready graduates while also meeting professional registration standards [3].
The measurement of work‐readiness is crucial as it provides an indication of the effectiveness of higher education in preparing graduates for the workforce and can inform curriculum development. Work‐readiness of graduates can be evaluated by employers using application forms, interviews, and cognitive tests, as well as academic achievement, but the validity of these approaches has been questioned [4]. Over the last decade, questionnaires specifically designed to determine work‐readiness of graduates, such as the work‐readiness scale (WRS), have been developed as a valid approach for determining self‐perceived work‐readiness [1].
Within the field of podiatry, the area of work‐readiness measurement is in its infancy, with few questionnaires specifically developed to measure the self‐perceived work‐readiness of podiatrists. Reynolds et al. [5] developed a work‐readiness tool by combining items from an exploratory qualitative study of 11 podiatrists that were clinical educators and historical competency standards. This tool, administered to 74 registered podiatrists in Australia and New Zealand, showed that 76% felt ‘prepared to practice as a podiatrist at graduation’. In addition, the WRS for allied health professionals (WRS‐AH) has been developed to assess the self‐perceived work‐readiness of allied health graduates [6]. This tool was validated with 245 allied health graduates, including 3 podiatrists, and perceived work‐readiness was reported as high, with a mean of 80%. Moreover, the employer satisfaction survey (ESS) measures employer satisfaction with graduates from Australian higher education institutions [7]. The ESS, a national annual generic survey, allows comparison across fields of education. An important consideration is that although the current tools may provide useful information regarding key capabilities for work‐readiness of podiatry graduates, neither tool has specifically included employers of graduate podiatrists in their development, which raises questions about their validity in reflecting the views of employers in podiatry. Although the tool developed by Reynolds et al. [5] used 11 clinical supervisors, their views may not be reflective of graduate employers.
There is a need to develop a podiatry‐specific graduate employer work‐readiness survey tool that aligns with current professional standards and incorporates employer perspectives. The engagement of consumers (i.e., employers of graduate podiatrists) in the tool's development is crucial to ensuring its validity, acceptance and dissemination [8]. Therefore, as an initial step toward developing a podiatry‐specific graduate employer work‐readiness tool, this study aimed to conduct a modified Delphi survey to achieve consensus among employers of podiatry graduates on the key capabilities required of podiatry graduates.
METHODS
2
Study design
2.1
This study used a Delphi technique which is an approach that seeks to obtain consensus on the opinions of ‘experts’ through a series of structured questionnaires (referred to as ‘rounds’) that are completed anonymously [9, 10, 11]. The La Trobe University Human Research Ethics Committee provided ethical approval (number HEC23363), and all participants provided written informed consent prior to enrolment. The study is reported according to the Conducting and REporting DElphi Studies (CREDES) checklist (Supporting Information S1: Supplementary file 1) [12].
Steering Committee
2.2
A Steering Committee consisting of the study authors (SEM, MC, MJO, NF, VC, MF, MTB, NWH, and HBM) guided the research. The committee members were registered podiatrists, and we aimed for representation across genders, geographical regions across Australia and New Zealand, across different health workplace (public and private clinical practice) and academic sectors.
Survey development
2.3
The initial survey was developed based on a comprehensive literature review, focusing on the knowledge, skills, and professional attributes (collectively referred to as ‘capabilities’ [13]) that were associated with employer satisfaction and work‐readiness among graduates in allied health, dentistry, and medicine in Australia and New Zealand. The literature review search strategy was developed by two authors (SEM, HBM). Terms related to employer satisfaction were based on a previous review of graduate work‐readiness [4], whereas terms related to health professions were derived from an Australian national government resource [14]. The literature search was conducted by one of the authors (SEM) to identify relevant records that capabilities could be extracted from. The search was conducted without date restriction up to October 28, 2022 in Medline, CINAHL, and Embase. The search strategy was designed to capture a broad range of terms related to employer satisfaction and work‐readiness of health practitioners in Australia and New Zealand (Supporting Information S2: Supplementary file 2). In addition, a search was conducted in Google and Google Scholar to identify grey literature. To ensure a comprehensive list of capabilities, the reference lists of the identified records were manually reviewed, and members of the Steering Committee were invited to suggest additional sources. The search identified 24 unique records, with 1 additional record [13] recommended by the Steering Committee on December 6, 2022. From these sources, a total of 403 potential capabilities were extracted by one member of the Steering Committee (SEM) and compiled in an Microsoft Excel spreadsheet. After removing duplicates using Excel's ‘remove duplicates' function, 388 unique capabilities remained. These were then thematically analysed by two independent Steering Committee members (SEM, MC) to eliminate any remaining duplicates and categorise them into domains that aligned with the ESS. Any disagreements were resolved through discussions. This process resulted in a refined list of 71 items, distributed across 7 domains, which were included in the Round 1 survey.
Delphi panel selection
2.4
Although there is no agreement on the sample size for Delphi studies, a minimum of 12 participants is considered sufficient to enable consensus to be achieved [10]. Therefore, we sought to form a panel of a minimum of 16 experts, assuming a dropout rate of 20% over the survey rounds [15]. The aim was to gather a diverse range of perspectives. We utilised a purposive sampling technique to recruit individuals with extensive experience and knowledge in mentoring and managing graduate podiatrists. The eligibility criteria for the experts were a minimum of 5 years of experience in managing podiatry graduates in clinical practice in Australia or New Zealand and having managed at least three graduates in the past 5 years. Invitations were developed with the goal of achieving a representative distribution across various geographic regions (including Australian states and territories and New Zealand provinces) and across different health workplace sectors (public and private). The study authors compiled a list of such experts, who were then sent an email invitation to participate in the study in February 2024.
Procedure
2.5
The study was carried out from March to August 2024. Eligible participants who agreed to participate received individual email invitations containing links to each survey round. The Delphi process was implemented by one of the authors (SEM). Study data were collected and managed using the REDCap (research electronic data capture) electronic data capture tool hosted at La Trobe University (Australia) [16, 17]. REDCap is a secure, web‐based software platform designed to support data capture for research studies, providing an intuitive interface for validated data capture, audit trails for tracking data manipulation and export procedures, automated export procedures for seamless data downloads to common statistical packages, and procedures for data integration and interoperability with external sources.
At the start of the online survey for Round 1, respondents were asked to confirm their consent, with a skip logic feature in place to exclude those who did not consent [18]. Each survey round was open for a period of 4 weeks. Participants who did not complete a survey round within the first week were sent up to three weekly reminder emails. Thereafter, if participants still did not complete a survey round after the closing date, they were contacted via a final email and offered an extension if needed. Participants who did not respond to the survey or follow‐up emails within 2 weeks after the closing date were classified as non‐responders [18]. After each round, participants were provided with a copy of their individual responses and the collective responses of the panel (presented as frequencies and proportions).
Survey rounds
2.6
The survey was conducted over three rounds. Piloting was performed by the authors prior to each round, and they were not involved as participants in the study. In Round 1 (item generation and rating), experts were presented with a series of statements derived from a literature review of capabilities that are indicative of work‐readiness and employer satisfaction in allied health, dentistry, and medicine graduates. These statements were rated by the participants using a five‐point Likert scale (ranging from ‘strongly disagree’, ‘disagree’, ‘neither agree nor disagree’, ‘agree’, to ‘strongly agree’) [15, 19]. Experts were also given the opportunity to suggest any additional items they believed should be included using free text. These suggestions were then thematically analysed within a deductive framework to generate a series of additional items for Round 2 [20]. This analysis was independently conducted by two Steering Committee members (SEM, MC), and any disagreements were resolved through discussion until a consensus was reached. In Round 1, data on participant characteristics were also collected including age, gender, sex, country of birth, ethnicity, principal location of practice, primary work sector, and experience (number of years as the manager of graduates and total number of graduates managed).
In Round 2 (item rating), experts were presented with the statements from Round 1 that received agreement levels between 50% and 75% agreement. These statements had not reached a consensus but were deemed to require further consideration by the panel. Alongside these statements, experts were also shown their own responses from Round 1, as well as the collective response of the group, represented by the median, mode, and proportion of responses in each category [19, 21, 22]. Experts were given the opportunity to re‐rate these items. Additionally, they were presented with new items that had been generated from the thematic analysis of the additional suggestions made in Round 1 and were asked to rate their agreement with these added items.
In Round 3 (item rating), the final round, the process from Round 2, was repeated. Additionally, experts were given the complete list of items that had reached consensus in the previous rounds, as well as items that had achieved 50%–75% agreement from Round 2. To prioritise capabilities, experts were then asked to rate the importance of each item as either ‘essential’ or ‘optional’ [23]. The Delphi process was concluded upon the completion of this round, regardless of whether full agreement was reached on all items.
Data handling and analysis
2.7
Data were analysed using SPSS Version 29 (IBM Corporation, Armonk, NY, USA). Participant characteristics were reported according to the distribution of the measurement scale. A range of 50%–95% has been used to define consensus in past Delphi studies, with 75% being the median [24]. Therefore, items were accepted if they reached ≥75% consensus. This required 75% or more of the experts to indicate that they agreed or strongly agreed with an item in Round 2 or 3. Round 2 and 3 included items where 50%–75% of experts had agreed or where there were additional comments from Round 2 to ensure adequate consideration. If less than 50% of participants agreed to an item, it was excluded from future rounds. Further, any item that did not reach consensus in Round 3 was excluded.
RESULTS
3
Participant characteristics
3.1
The flow of the study process is presented in Figure 1. A total of 31 potential participants were invited, and responses were received from 25 in Round 1, 24 in Round 2, and 23 in Round 3, representing an 8% (n = 2 drop‐outs) participant attrition rate during the study. Participant characteristics (Round 1) are shown in Table 1. All members of the expert panel were registered podiatrists. The expert panel comprised of 13 (52%) women, and the mean (SD) age was 46.1 (7.6) years. Most participants described being born in Australia (76%) or New Zealand (16%) and the majority identified as being of Oceanian (44%) or North‐West European (36%) ethnicity. The principal location of practice was Australia in 21 (84%) of participants, where Victoria (n = 7, (28%), South Australia (n = 4, 16%), and Queensland (n = 3, 12%) were most represented. Participants from New Zealand (n = 4, 16%) were from Auckland (n = 2, 8%), Canterbury, and Wellington (each n = 1, 4%). The majority (n = 19, 76%) of participants managed graduates in the private sector, had been managing graduates for a mean of 14.9 years, and had managed a mean total of 12 graduates which included a mean of 5 graduates in the previous five years (since 2019).
Flow of the study process.
Consensus and agreement on the key capabilities required for podiatry graduates to meet workforce needs across survey rounds
3.2
Table 2 presents the agreement among the expert panel. In Round 1, 71 items were presented. Of these, 36 (50.7%) achieved consensus and were accepted, 11 (15.5%) were excluded, and 24 (33.8%) were classified as uncertain (50%–75% of respondents had rated that item as ‘agree’ or ‘strongly agree’) and carried forward to be presented in Round 2. Furthermore, 7 additional capabilities were received from respondents to be presented in Round 2. In Round 2, 31 items were presented and 22 (71.0%) achieved consensus and were accepted, 1 (3.2%) was excluded, and 8 (25.8%) were classified as uncertain (this included 1 item where a data error prevented analysis). In Round 3, 8 items were presented, with 3 (37.5%) achieving consensus and being accepted, and 5 (62.5%) items being classified as uncertain being excluded. Overall, of the 78 items (71 in Round 1 plus 7 additional items generated) presented to respondents, 61 (78.2%) achieved consensus and were accepted, and 17 (21.8%) were excluded.
Table 3 presents the expert panel's ratings of the 61 key capabilities that achieved consensus as being essential versus optional. Thirty‐nine items (63.9%) were rated as ‘essential’ by 75% of more respondents, 17 (27.9%) were rated as ‘essential’ by 50%–75% of respondents, and 5 (8.2%) were rated as ‘essential’ by less than 50% of respondents. Figure 2 presents these ratings in a descending order.
TABLE 3: Essential versus optional ratings of the expert panel for key capabilities required of podiatry graduates that achieved consensus. a
Ratings of the 61 key capabilities that achieved consensus as being essential versus optional. Proportion of expert panel rating capability as ‘essential’: green bars (≥75%), yellow bars (50%–75%), red bars (<50%).
DISCUSSION
4
We conducted a Delphi survey to achieve consensus among employers of podiatry graduates on the key capabilities required for podiatry graduates. Our expert panel consisted of 25 participants with a mean of 15 years of experience in managing podiatry graduates in clinical practice in Australia or New Zealand who reported managing a mean 12 graduates, including 5 since 2019. Of the 78 items presented to our expert panel, 61 (78.2%) achieved consensus and were accepted, and 17 (21.8%) were excluded. Of the 61 items that achieved consensus, thirty‐nine (63.9%) were rated as ‘essential’ by 75% of more respondents. To the best of our knowledge, this study is the first to seek to comprehensively identify key capabilities required for podiatry graduates from an employer's perspective.
A considerable proportion (n = 61, 78%) of items that were presented to the expert panel achieved consensus and were accepted. This was not surprising, given that the generation of items was based on a comprehensive literature search, generation from members of the Steering Committee and expert panel input in Round 1. Specifically, there was 100% consensus for items within the generic foundation capability, generic collaborative capability, and generic technical capability domains. In contrast, the generic employability capability domain had the largest proportion of items (n = 4, 22% within this domain) that did not achieve consensus. The capabilities ‘demonstrating leadership skills’, ‘demonstrating management skills’, ‘marketing knowledge and skills’, ‘administration knowledge and skills’, and ‘systems thinking (ability to have a broader perspective)’ did not achieve consensus. These findings are not unexpected as the items could be considered more reflective of acquired capabilities used by experienced podiatrist employees in leadership roles. However, further research is required to confirm this.
There were some unexpected findings. The items ‘ability to develop innovative ideas’ and ‘ability to identify new opportunities’ from the generic adaptive capabilities domain did not achieve consensus. These capabilities are specific items of the national Australian graduate employer survey, the ESS [7]; so, while these capabilities are generally important for graduates, they might not be as critical for podiatrists specifically. Further, there were three items (n = 3, 18% within this domain) from the podiatry‐specific capabilities domain that did not achieve consensus. These were capabilities relating to ‘seek opportunities to progress the profession for the benefit of the community’, ‘examine and reflect on how one's own culture influences perceptions and interactions with others from different cultures’, and ‘regularly implement quality assurance processes to improve patient care’. This was unexpected as these items were derived from the Podiatry Board of Australia Professional Capabilities for Podiatrists [13], which describes the threshold capabilities needed to practice as a registered podiatrist in Australia. The findings related to the items ‘ability to develop innovative ideas’, ‘ability to identify new opportunities’, ‘regularly implement quality assurance processes to improve patient care’, and ‘seek opportunities to progress the profession for the benefit of the community’ could be considered more relevant for experienced podiatrists rather than new graduates. However, additional studies are required to verify this.
The finding that the item ‘examine and reflect on how one's own culture influences perceptions and interactions with others from different cultures’ did not achieve consensus as being considered important for new graduates does not reflect the fundamental role of self‐reflexivity in the development of culturally capable healthcare practitioners. This finding also likely reflects historical education and healthcare training within Western monocultural training modules and highlights the need for upskilling within the profession to facilitate the availability of culturally safe podiatry care. In Australia and New Zealand, access to culturally safe practice is mandated in the National Law. Culturally safe practice is integrated throughout the professional capabilities of the podiatry profession in Australia and New Zealand. It is well recognised that the cultural safety deficit in our healthcare systems negatively impacts the health of Indigenous people [25, 26]. To redress these health inequities, it is crucial for podiatrists to develop and value skills for providing culturally safe healthcare from graduation throughout their professional lives [26]. Additionally, the podiatry profession must enhance its awareness of self‐reflexivity as a key professional capability for delivering culturally safe practices. To this end, this authorship group views the capability ‘examine and reflect on how one's own culture influences perceptions and interactions with others from different cultures’ as an essential capability of new graduate practitioners and experienced practitioners alike.
The findings of this study have the potential to inform the creation of a podiatry‐specific graduate employer work‐readiness tool. This tool could enable graduate employers to provide feedback to podiatry education program providers on the effectiveness of their curricula in preparing graduates for the workforce. Additionally, the study's findings could serve as a framework for employers to identify, communicate with, and support the capability development of new podiatry graduates. Regulatory bodies could also utilise these findings in their review and revision of podiatry standards. A potential barrier to developing a comprehensive work‐readiness tool is the length, given that all 61 items achieving consensus could be included. Statistical approaches such as factor analysis could be used to reduce the number of items [27]. Alternatively, a short form of the tool could be developed using the 39 items deemed ‘essential’ by 75% or more of the respondents in our study. Overall, these outcomes have the potential to enhance the work‐readiness of podiatry graduates, optimise work performance, satisfaction, and engagement, and reduce workforce attrition.
A strength of the study is the use of an iterative Delphi method, which used a diverse group of participants with extensive experience in managing podiatry graduates in clinical practice in Australia or New Zealand. Overall, the study participants were proportionately representative in terms of gender, workplace settings (private and public), and geographic distribution across Australia and New Zealand [28, 29, 30, 31]. However, the findings of this study should be interpreted considering its limitations. Firstly, we did not provide qualifiers and examples for each item to optimise understanding. Consequently, some items may not have achieved consensus due to ambiguity. Secondly, although we endeavoured to recruit a representative sample for our Steering Committee and Delphi expert panel, each may not fully reflect the diversity of the populations they are intended to represent. For instance, both the Steering Committee and expert panel lacked representation from Indigenous people, and we did not determine if panelists identified as having a disability, were lesbian, gay, bisexual, transgender, queer or intersex, or were from socioeconomically disadvantaged backgrounds. This could explain our finding that the capability ‘examine and reflect on how one's own culture influences perceptions and interactions with others from different cultures’ did not achieve consensus as being considered important for new graduates. Any future work should explore this further with groups that are more representative of priority populations. Further, the findings may not reflect the perspective of graduate employers outside of Australia and New Zealand. Thirdly, the findings of this study are likely to be time‐dependent and may not represent the perspectives of future graduate employers. Future employers in podiatry may prioritise environmental sustainability and ability to provide cultural safe practice as essential capabilities for new graduates [26, 32]. Fourthly, there is potential that additional capabilities for work‐readiness in allied health graduates were reported in publications following the literature search in October 2022 that were not presented in Round 1 to Delphi expert panelists in March 2024. In this regard, both the podiatry‐specific work‐readiness tool reported by Reynolds et al. [5] and WRS‐AH tool [6] were published in 2023. However, we believe that this study generated a complete list of capabilities because (i) a comprehensive search was used to create the initial list presented in Round 1 and (ii) expert panelists added additional items during Round 1 of the survey.
CONCLUSION
5
A consensus among employers of podiatry graduates was established on the key capabilities required for podiatry graduates. Sixty‐one items were identified across seven domains, and of these, 39 items were rated as essential. The findings of this study can inform the creation of a podiatry‐specific graduate employer work‐readiness tool that could be used by employers to provide feedback to podiatry education program providers as well as new graduates in the workplace.
AUTHOR CONTRIBUTIONS
Shannon E. Munteanu: Conceptualisation; methodology; writing—original draft; writing—review & editing. Matthew Cotchett: Conceptualisation; methodology; writing—review & editing. Matthew J. Oates: Conceptualisation; methodology; writing—review & editing. Nicoletta Frescos: Conceptualisation; methodology; writing–review & editing. Vivienne Chuter: Conceptualisation; methodology; writing–review & editing. Mike Frecklington: Conceptualisation; methodology; writing—review & editing. Marie T. Butler: Methodology; writing—review & editing. Nick W. Haley: Methodology; writing–review & editing. Hylton B. Menz: Conceptualisation; methodology; writing—review & editing.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
The La Trobe University Human Research Ethics Committee provided ethical approval (number HEC23363), and all participants provided written informed consent prior to enrolment.
Supporting information
Supporting Information S1
Supporting Information S2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Caballero, C. L. , A. Walker , and M. Fuller‐Tyszkiewicz . 2011. “The Work Readiness Scale (WRS): Developing a Measure to Assess Work Readiness in College Graduates.” Journal of Teaching and Learning for Graduate Employability 2(1): 41–54. 10.21153/jtlge 2011 vol 2no 1art 552. · doi ↗
- 2Walker, A. , and K. Campbell . 2013. “Work Readiness of Graduate Nurses and the Impact on Job Satisfaction, Work Engagement and Intention to Remain.” Nurse Education Today 33(12): 1490–1495. 10.1016/j.nedt.2013.05.008.23742716 · doi ↗ · pubmed ↗
- 3Australian Government: Australian Universities Accord Final Report . 2023.
- 4Caballero, C. L. , and A. Walker . 2010. “Work Readiness in Graduate Recruitment and Selection: a Review of Current Assessment Methods.” Journal of Teaching and Learning for Graduate Employability 1(1): 13–25. 10.21153/jtlge 2010 vol 1no 1art 546. · doi ↗
- 5Reynolds, K. , E. Rathbone , and M. Mc Lean . 2023. “Competencies Associated with Australian and New Zealand Podiatrists' Perceptions of Their Preparedness for Graduate Clinical Practice.” Australian Journal of Clinical Education 12(1): 71–91. 10.53300/001c.84453. · doi ↗
- 6Lawton, V. , E. Ilhan , V. Pacey , T. M. Jones , A. Walker , and C. M. Dean . 2023. “A Work Readiness Scale for Allied Health Graduates.” The Internet Journal of Allied Health Sciences and Practice 22(1): Article 16.
- 7Quality Indicators for Learning and Teaching (QILT) . Employer Satisfaction Survey. https://www.qilt.edu.au/surveys/employer‐satisfaction‐survey‐(ess)
- 8Saunders, C. , and A. Girgis . 2010. “Status, Challenges and Facilitators of Consumer Involvement in Australian Health and Medical Research.” Health Research Policy and Systems 8(1): 34. 10.1186/1478-4505-8-34.21087513 PMC 2998503 · doi ↗ · pubmed ↗