Mean Fetal Kidney Length at the Third Trimester: An Emerging Ultrasound Parameter for Gestational Age Assessment
Sasikala Kathiresan, Susithira Aarthy, Emil Phinehas, Kalaiselvi Selvaraj

TL;DR
This study shows that fetal kidney length is a more accurate way to estimate gestational age in the third trimester compared to traditional ultrasound measurements.
Contribution
The study introduces fetal kidney length as a novel and reliable ultrasound parameter for gestational age assessment in late pregnancy.
Findings
Fetal kidney length had a 97.4% accuracy in predicting gestational age, compared to 57.3% for conventional markers.
Fetal kidney length showed narrower agreement limits with last menstrual period-based gestational age than traditional biometric parameters.
Fetal kidney length is unaffected by growth restrictions, making it more reliable in high-risk pregnancies.
Abstract
Introduction Accurate gestational age (GA) determination is essential for effective obstetric care, guiding the timing of delivery, fetal evaluations, and interventions. Conventional ultrasound (USG) markers such as biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL) often lose precision in the third trimester, with discrepancies of up to three weeks. These limitations highlight the need for alternative, reliable metrics. Fetal kidney length (FKL), which increases consistently by about 1 mm per week after 24 weeks of gestation and remains unaffected by growth restrictions, presents a promising alternative. This study aimed to evaluate the diagnostic utility of mean FKL for third-trimester GA assessment. Methods A cross-sectional study was conducted from March to June 2021 at a tertiary care hospital in Tamil Nadu, India. Fifty…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
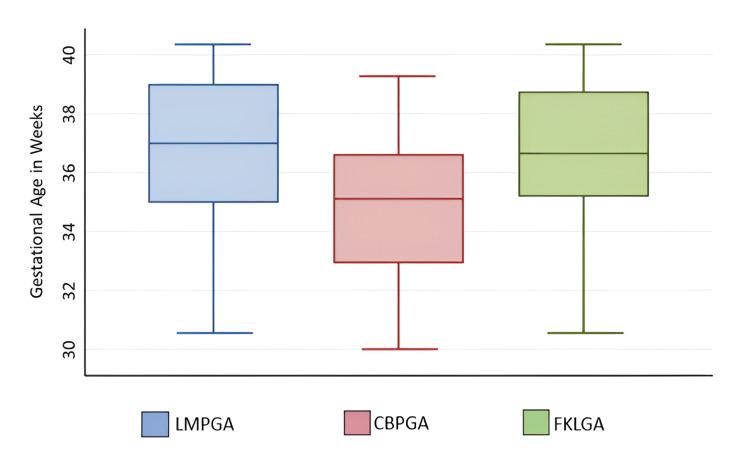 Figure 1
Figure 1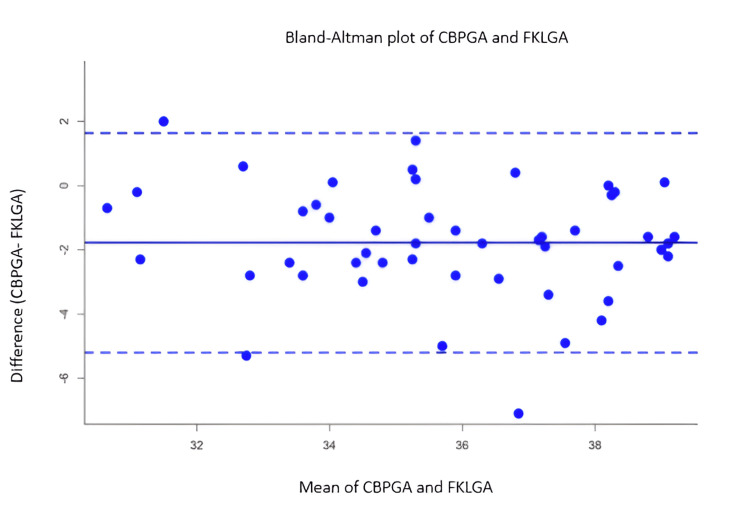 Figure 2
Figure 2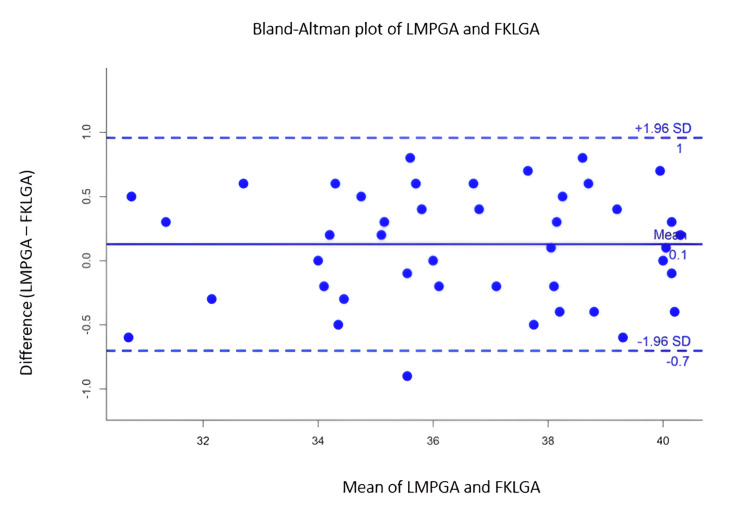 Figure 3
Figure 3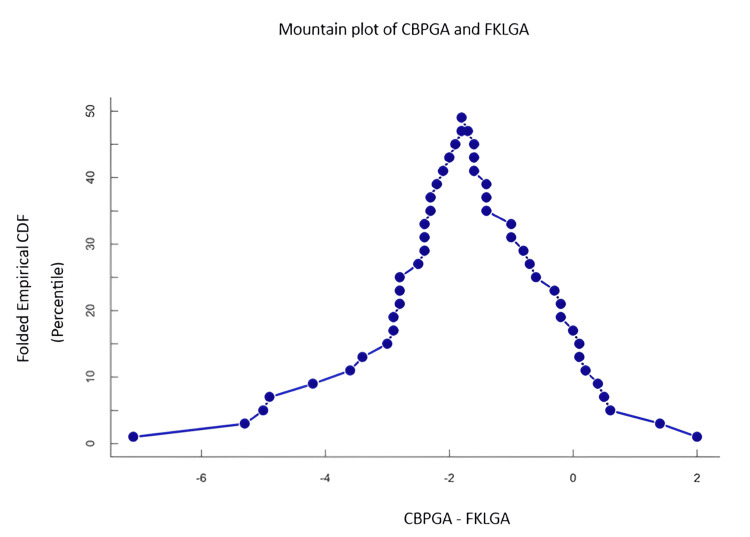 Figure 4
Figure 4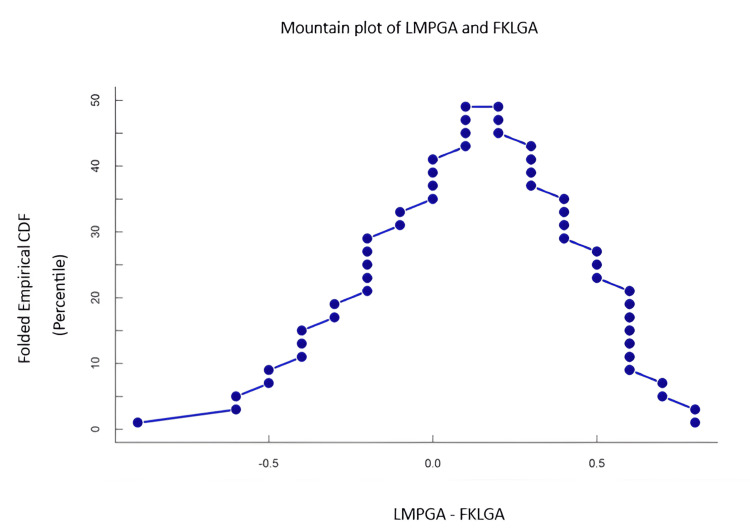 Figure 5
Figure 5| Factor | Frequency (number) | Percentage (%) |
| Gravida | ||
| Primigravida | 27 | 54 |
| 2 | 10 | 20 |
| 3 or more | 13 | 26 |
| Para | ||
| Nullipara | 27 | 54 |
| 1 | 13 | 26 |
| 2 or more | 10 | 20 |
| Previous history of abortion status | ||
| No | 46 | 92 |
| Yes | 4 | 8 |
| Age mean (SD) | 23.6 (1.6) | |
| Parameter | Mean | SD | P25 | P75 |
| BPD (cm) | 8.57 | 0.52 | 8.25 | 8.9 |
| AC (cm) | 31.3 | 2.3 | 30.2 | 32.4 |
| HC (cm) | 31.4 | 1.6 | 30 | 32.5 |
| FL (cm) | 6.6 | 0.6 | 6.2 | 7.1 |
| Mean FKL (mm) | 36.3 | 3.2 | 33.7 | 38.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Birth, Development, and Health · Pediatric Urology and Nephrology Studies
Introduction
Accuracy in the calculation of gestational age (GA) is the cornerstone in obstetric care that drives the treatment plan in terms of time and mode of delivery. It also provides the critical window for various screening tests and assessment of the fetus in the continuum of care during pregnancy. Inappropriate GA assessment results in either underestimation of potential risks in fetuses such as intrauterine growth restriction (IUGR) or poorly timed interventions such as induction of labor or cesarean section. Women who present late in pregnancy with uncertain or unknown menstrual dates rely on ultrasound (USG) for GA, which is the least reliable after the first trimester. Hence, careful consideration of the entire clinical picture is required in management decisions when based on third-trimester ultrasound alone.
In practice, gestational assessment with the last menstrual period (LMP) along with a first-trimester dating scan by measuring crown-rump length ascertain GA accurately [1]. However, GA in the second and third trimesters assessed by conventional biometric parameters (CBP) in ultrasound, such as head circumference (HC), biparietal diameter (BPD), abdominal circumference (AC), and femur length (FL), is with disparities. This can be as high as three weeks in the third trimester [2]. As a result, increasing GA is an independent risk factor for inappropriate GA assessment by CBP in ultrasonography (USG) [3]. Thus, there is a need for more accurate estimates of gestational age through better diagnostic parameters.
Fetal kidney development has demonstrated a consistent increase of 1.7 mm every two weeks during pregnancy, remaining unaffected by any growth abnormalities [4]. As reported by Konje et al., fetal kidney length (FKL) correlates positively with gestational age after 24 weeks [5]. Further, FKL is an easily reproducible parameter in third-trimester ultrasound [6]. Unlike other conventional biometric parameters, FKL does not vary with fetal growth restriction compared to appropriately grown fetuses [7]. In this context, this study aimed to ascertain the diagnostic utility of mean FKL measurement in the determination of GA in the third trimester.
Hence, the aims and objectives of this study are as follows: to estimate the intraclass correlation between mean fetal kidney length (FKL) measurement in the determination of gestational age (GA) using ultrasonography (USG), to assess the reliability of mean FKL measurement in the determination of gestational age against other conventional biometric parameters (BPD, HC, AC, and FL) by ultrasonography, and to build the model to predict gestational age using mean FKL measurement.
Materials and methods
Study design and setting
This was a facility-based cross-sectional study conducted in a tertiary care hospital in Madurai, Tamil Nadu. This facility caters to two lakh reproductive population approximately. The annual footfall of antenatal women registered and receiving antenatal care from this facility is around five hundred. Trained obstetricians and radiologists perform the ultrasound in this facility.
Study population and sampling method
After obtaining Institutional Ethics Committee (IEC) approval (approval number: VMCIEC/01/2021, date: 24/02/2021), this study included antenatal pregnant women who had 28 completed weeks but within 42 weeks of the gestation period, were not classified under any high-risk pregnancy categories, had singleton pregnancy, and were able to accurately recall the last menstrual period (LMP) with corresponding gestation confirmed in the first-trimester dating scan done between eight and 12 weeks of gestation. Pregnant women with an anomalous fetus, suspected IUGR, unknown dates, multiple gestations, gestational diabetes mellitus, oligo-/polyhydramnios, fetal hydroureteronephrosis and other renal abnormalities, and failure to visualize biometric parameters were excluded from the study. All pregnant women referred for antenatal USG in the facility, during the reference period from March to June 2021, were consequently enrolled without further sampling. A total of 50 third-trimester antenatal women were included in the study after applying the inclusion and exclusion criteria.
Data collection
One trained operator (radiologist with five years experience) performed all examinations using a 2-5 MHz curvilinear probe in a Philips HD5 ultrasound machine (Bothell, WA). The conventional biometric parameters (BPD, HC, AC, and FL) were measured in the USG, based on the standard methods described in Callen's Ultrasonography in Obstetrics and Gynecology [8]. Mean FKL refers to the whole length of both kidneys separately in the paravertebral plane; the values were averaged. All parameters were taken during restricted/minimal fetal movements. Data were collected in a structured data extraction sheet. The variables included were the age of the pregnant woman, LMP, GA based on LMP, conventional biometric parameters as per USG (BPD, HC, AC, and FL), GA as per conventional parameters, mean FKL, and GA as per FKL.
Data management
Data were entered in an Excel spreadsheet (Microsoft Corp., Redmond, WA). Clinical and demographic features were summarized as frequencies and percentages. Biometric parameters were described as mean and standard deviation (SD). Using the linear regression model, the equation for estimating gestational age from mean FKL was obtained. In the linear regression, the actual gestational age was the dependent variable and FKL was the independent variable. The Bland-Altman plot was drawn between predicted gestational age using mean FKL and actual gestational age based on LMP with limits of agreement (LoA) including difference ±2 standard error limits. Similarly, gestational age based on other fetal parameters and LMP-based gestational age were also plotted. Intraclass correlation measures were estimated. All analyses were done using Stata software (StataCorp LLC, College Station, TX), and plots were created in R software.
Results
A total of 50 antenatal women were enrolled in the study for the assessment of GA using various ultrasonogram-based parameters. About 54% of them were primigravidae, and 8% of the study population had a previous history of abortion. The mean (SD) age of the participants was 23.6 (1.6) years. Other obstetric parameters of the participants are described in Table 1, and the distribution of biometric parameters in ultrasonogram is listed in Table 2.
The median gestational age based on LMP (LMPGA) was 37 weeks with an interquartile range (IQR) from 35 to 39 weeks. The IQR of mean fetal kidney length-based gestational age (FKLGA) varied from 35 to 38 weeks. The average gestational age based on conventional biometric parameters (CBPGA) (BPD, HC, AC, and FL) was lower compared to LMPGA or FKLGA (Figure 1).
Distribution of gestational age based on different parametersEach box represents the IQR, which contains the middle 50% of the data (from the 25th to the 75th percentile), whereas the line inside the box indicates the median gestational age for each method. LMPGA has the highest median gestational age, and CBPGA has the lowest median, indicating that it may systematically underestimate gestational age compared to FKLGA.LMPGA: last menstrual period-based gestational age, CBPGA: conventional biometric parameter-based gestational age, FKLGA: fetal kidney length-based gestational age, IQR: interquartile range
In Figure 2 and Figure 3, the Bland-Altman plot was drawn between the average of reference gestational age (LMPGA) and index markers such as FKL and conventional biometric parameters in the X-axis and the difference between reference (LMPGA) and conventional biometric parameters in the Y-axis. The limits of agreement (LoA) fall between -0.5 and 1 week in the mean FKL-based index markers, whereas the LoA varied from -2 to 6 weeks in the other markers based on gestational age.
Bland-Altman plot showing the mean and the difference between CBPGA and FKLGAThe mean of CBPGA and FKLGA in the X-axis represents the average gestational age estimated by the two methods, whereas the difference between CBPGA and FKLGA in the Y-axis shows the difference in gestational age estimates between CBPGA and FKLGA for each data point. The mean difference is slightly negative, suggesting that, on average, FKLGA estimates are slightly higher than CBPGA. Most of the data points lie within the limits of agreement (±1.96 SD), which suggests that the two methods generally agree.CBPGA: conventional biometric parameter-based gestational age, FKLGA: fetal kidney length-based gestational age, SD: standard deviation
Bland-Altman plot showing the mean and the difference between LMPGA and FKLGAThe mean difference is close to zero (+0.1), indicating almost no systematic bias between LMPGA and FKLGA, suggesting that FKLGA provides gestational age estimates that align closely with LMPGA on average. The small mean difference and narrow limits of agreement indicate that LMPGA and FKLGA are comparable methods for estimating gestational age.LMPGA: last menstrual period-based gestational age, FKLGA: fetal kidney length-based gestational age
In Figure 4 and Figure 5, the mountain plot based on difference and cumulative distribution function also showed the peak around 0 in mean FKLGA, whereas the peak was observed at 2 weeks in other markers. The consistent difference (centered near -2 weeks) indicates that CBPGA systematically underestimates gestational age compared to FKLGA.
Mountain plot showing the difference between CBPGA and FKLGAThe X-axis represents the difference in gestational age estimates between CBPGA and FKLGA, whereas the Y-axis represents the CDF in a folded or symmetric manner around the peak. The central tendency is near -2, indicating that the most frequent difference between CBPGA and FKLGA is approximately -2 weeks, suggesting that, on average, CBPGA underestimates gestational age compared to FKLGA. A narrow and steep curve suggests better agreement, as the differences are clustered around the peak value.CBPGA: conventional biometric parameter-based gestational age, FKLGA: fetal kidney length-based gestational age, CDF: cumulative distribution function
Mountain plot showing the difference between LMPGA and FKLGAThe central tendency is around 0, indicating that the most frequent difference between LMPGA and FKLGA is approximately 0 weeks, suggesting a good overall agreement between the two methods. The narrow and steep curve indicates strong agreement between the methods, with minimal variability.LMPGA: last menstrual period-based gestational age, FKLGA: fetal kidney length-based gestational age, CDF: cumulative distribution function
The intraclass correlation between LMPGA and mean FKLGA was 0.986 (95% CI: 0.976-0.992). The intraclass correlation between LMPGA and GA based on other markers was 0.539 (95% CI: 0.31-0.739). The linear regression model was built considering LMPGA as a dependent variable and maternal age and index markers (mean FKLGA and GA based on other markers) as independent variables. Maternal age was found to be insignificant. The fetal kidney-based model explained around 97.4% variability in the gestational age (adjusted squared R - 0.9738). Each one-unit increase in fetal kidney length correspondingly increased one week of gestational age (beta coefficient: 0.99; 95% CI: 0.94-1.04; p = 0.001). In the linear regression, gestational age based on other markers explained 57.3% of the variability in the gestational age (beta coefficient: 0.85; 95% CI: 0.64-1.06; p = 0.001; adjusted squared R - 0.5729).
Discussion
The current study carried out among third-trimester pregnant women showed the following key features: (1) the high intraclass correlation observed between mean FKLGA and LMPGA compared to other traditional USG-based fetal biomarkers; (2) about 97% of the variability in gestational age was explained by fetal kidney length alone, whereas other markers, such as BPD, HC, AC, and FL, were able to explain around 57%; and (3) a one-unit (1 mm) increase in FKL corresponds to one week of maturity in GA [9].
Gestational age is the single most predominant factor that determines the course of action in managing high-risk pregnancies and determines the prognosis. The favorable maternal and fetal outcomes are dependent on these key decisions. However, in the context where not all registration of pregnancies are within the first trimester and often proportion of antenatal women recalling their LMP is less than 80% [3], the reliance on USG-based fetal markers cannot be overlooked.
Although USG plays a vital role in GA assessment, its accuracy is limited to the first trimester. For pregnant women presenting late or uncertain LMP dates, third-trimester conventional biometric parameters are less reliable in GA assessment. Rumack and Levine noted in their textbook that the kidneys continue to develop during pregnancy [10]. They provide a nomogram illustrating renal lengths from 14 to 42 weeks of gestation, indicating that the renal-to-abdominal circumference ratio remains stable at 0.27-0.30 throughout pregnancy. The mean FKL in assessing GA is in close correlation with GA by LMP in comparison with GA assessment with other conventional biometric parameters in USG [11]. Kidneys are identified easily and measured in late pregnancy.
The gestational age in the third trimester was estimated using LMP, CBP, and mean FKL in this study. It is observed that LMPGA might tend to overestimate gestational age, while CBPGA might underestimate it. FKLGA lies in between, potentially making it a balanced option. This study shows that the length of the mean fetal kidney length and gestational age linearly increases from 29.5 ± 3 mm at 31 weeks to 40 ± 3 mm at 40 weeks, which is similar to the study conducted by Peter et al. in the Indian population [12]. The current study reports a high ICC between LMPGA and FKLGA, which was 0.986, whereas CBPGA has an ICC of 0.539. These measurements are close to the findings of Yusuf et al. [13] and Bardhan et al. [14]. Evidence from various other parts of the world has reported between 20 and 40 weeks of FKL, which acts as a reliable marker [15]. The high level of agreement implies that both LMPGA and FKLGA can be used in most clinical scenarios for GA assessment; however, given the small differences, FKLGA can be considered a practical alternative to LMPGA, especially in scenarios where LMP data are unavailable or uncertain. The rate of increase in FKL reported in the current study (1 mm increase per GA week maturity) corresponds to the coefficient level reported by Kansaria and Parulekar (0.9 mm/GA week) [4]. This is consistent with the study by Cohen et al. that kidney length correlates with gestation [16,17]. Konje et al. predicted the gestational age close to ±8 days in the third trimester by combining FKL and conventional biometric parameters [5].
The study included only 50 participants from a single center, which may limit the generalizability of the findings. Larger, more diverse populations are necessary to validate the results. High-risk pregnancies were excluded, which may limit the applicability of the findings to more complex clinical cases where accurate GA estimation is often more critical.
Conclusions
This research highlights the effectiveness of mean FKL as an ultrasonographic measure for accurately determining GA during the third trimester. With an impressive intraclass correlation of 0.986 between FKLGA and LMPGA, FKL surpasses traditional biometric indicators such as biparietal diameter, head circumference, abdominal circumference, and femur length, which tend to exhibit higher variability and lower reliability. The consistent linear growth pattern of FKL aligns closely with GA, making it an essential tool for pregnancies that present late or have uncertain LMP dates. The findings indicate that FKL accounts for 97% of the variability in GA, providing a crucial advantage in clinical scenarios where precise GA estimation is vital for timely and appropriate obstetric interventions. Further studies with diverse populations are needed to replicate the analysis across different subgroups to confirm the generalizability of this agreement. Integrating FKL into standard third-trimester ultrasonographic evaluations could enhance maternal and fetal outcomes by delivering more accurate GA measurements, particularly when other methods are inadequate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dating and growth in the first trimester Best Pract Res Clin Obstet Gynaecol Bottomley C Bourne T 4394522320091928224710.1016/j.bpobgyn.2009.01.011 · doi ↗ · pubmed ↗
- 2Sonographic prediction of gestational age: accuracy of second- and third-trimester fetal measurements AJR Am J Roentgenol Benson CB Doubilet PM 127512771571991195088110.2214/ajr.157.6.1950881 · doi ↗ · pubmed ↗
- 3Dating ultrasounds are fundamental to modern obstetric care Ir Med J Mohamed M Mc Cormick CA Foo A Meaney S O' Donoghue K 5821152022 https://pubmed.ncbi.nlm.nih.gov/35695731/35695731 · pubmed ↗
- 4Nomogram for foetal kidney length Bombay Hosp J Kansaria J Parulekar S 155162512009 https://www.semanticscholar.org/paper/Nomogram-for-Foetal-Kidney-Length-Kansaria-Parulekar/bf 9a 37cade 3fd 5039 f 2688323 cacea 5e 3c 75c 4b 9
- 5Determination of gestational age after the 24th week of gestation from fetal kidney length measurements Ultrasound Obstet Gynecol Konje JC Abrams KR Bell SC Taylor DJ 5925971920021204754010.1046/j.1469-0705.2002.00704.x · doi ↗ · pubmed ↗
- 6Fetal kidney length as a useful adjunct parameter for better determination of gestational age Saudi Med J Ugur MG Mustafa A Ozcan HC Tepe NB Kurt H Akcil E Gunduz R 5335373720162714661610.15537/smj.2016.5.14225 PMC 4880653 · doi ↗ · pubmed ↗
- 7A cross-sectional study of changes in fetal renal size with gestation in appropriate- and small-for-gestational-age fetuses Ultrasound Obstet Gynecol Konje JC Okaro CI Bell SC de Chazal R Taylor DJ 2226101997926341910.1046/j.1469-0705.1997.10010022.x · doi ↗ · pubmed ↗
- 8Callen's ultrasonography in obstetrics and gynecology, 6th edition Norton ME Scoutt LM Feldstein VA 82025 Elsevier 97803233283402017 https://www.us.elsevierhealth.com/callens-ultrasonography-in-obstetrics-and-gynecology-9780323328340.html