Endoscopic ultrasound-guided hepaticogastrostomy without tract dilation using a novel 0.035-inch guidewire
Ritsuko Oishi, Haruo Miwa, Kazuki Endo, Hiromi Tsuchiya, Yuichi Suzuki, Kazushi Numata, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
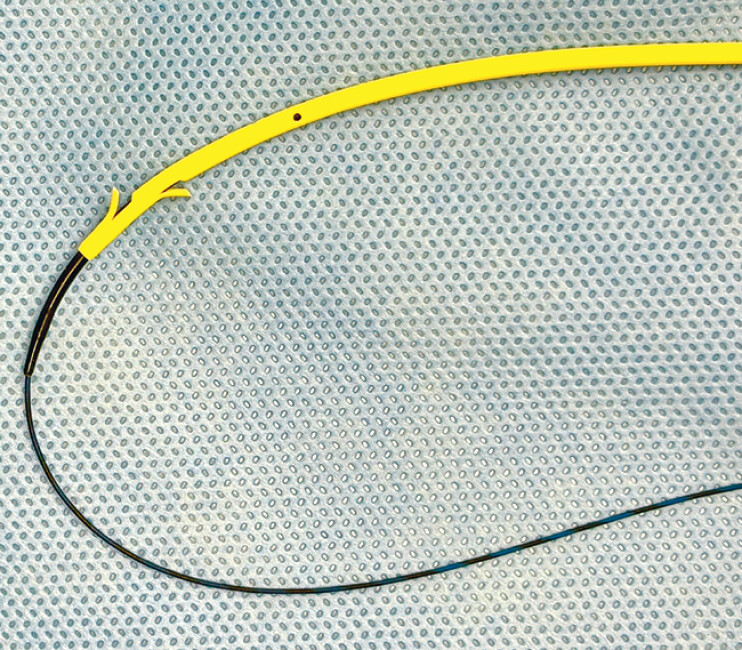 Fig. 1
Fig. 1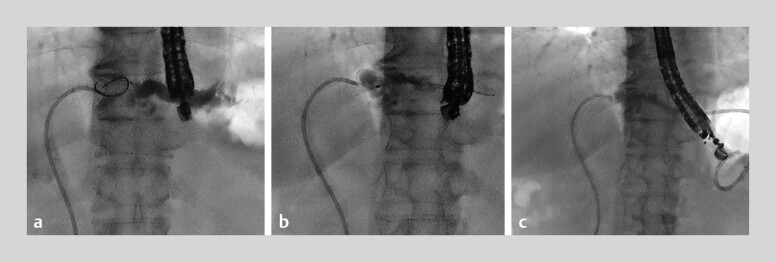 Fig. 2
Fig. 2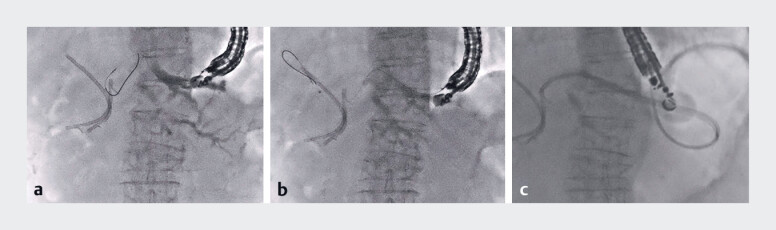 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Pediatric Hepatobiliary Diseases and Treatments
Biliary peritonitis is one of the complications of endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS), and it is mostly caused by tract dilation 1 2 3 . In patients with acute cholangitis, bile leakage may cause refractory infection in the abdominal cavity. Therefore, omitting tract dilation is expected to reduce the risk of bile peritonitis; however, plastic stent placement without tract dilation has been reported as challenging 4 . A novel 0.035-inch guidewire (CAPELLA 0.035; Japan Lifeline Co., Ltd., Tokyo, Japan) has a stiff shaft that facilitates stent deployment in EUS-HGS ( Fig. 1 ), which is also compatible with most devices designed for 0.025-inch guidewires. Herein, we present two cases in which a plastic stent was successfully placed without tract dilation using a CAPELLA 0.035 during EUS-HGS ( Video 1 ).
A novel 0.035-inch guidewire (CAPELLA 0.035) has a stiff shaft that facilitates stent deployment in endoscopic ultrasound-guided hepaticogastrostomy, and it is also available with most devices dedicated to 0.025-inch guidewires.
A novel guidewire, CAPELLA 0.035-inch, has a soft and tapered tip that facilitates plastic stent placement without tract dilation during endoscopic ultrasound-guided hepaticogastrostomy.Video 1
Case 1: A 78-year-old man with acute cholangitis caused by biliary stricture of the lateral branch was admitted. EUS-HGS was performed because transpapillary drainage failed. Firstly, B2 was punctured with a 19-gauge needle, and a 0.025-inch guidewire (VisiGlide 2; Olympus Medical Systems, Tokyo, Japan) was inserted after contrast injection. Subsequently, an ultra-tapered catheter (MTW Endoskopie Manufaktur, Wesel, Germany) was advanced, and the guidewire was exchanged for a CAPELLA 0.035. Finally, a 7-Fr plastic stent (Through and Pass Type IT; Gadelius Medical, Tokyo, Japan) was successfully placed ( Fig. 2 ).
Case 1. a B2 was punctured with a 19-gauge needle, followed by contrast injection and insertion of a 0.025-inch guidewire. b An ultra-tapered catheter was inserted into the bile duct, and the guidewire was exchanged for a CAPELLA 0.035. c A 7-Fr plastic stent was successfully placed without tract dilation.
Case 2: An 82-year-old woman with a hepaticojejunostomy anastomotic stricture due to recurrence of ampullary carcinoma was admitted with acute cholangitis. EUS-HGS was performed for acute cholangitis caused by the recurrence of a biliary obstruction after plastic stent placement. B2 was punctured with a 19-gauge needle and a 0.025-inch guidewire was placed in the right hepatic duct. After the guidewire exchange for a CAPELLA 0.035, the plastic stent was successfully placed ( Fig. 3 ).
Case 2. a B2 was punctured with a 19-gauge needle, followed by contrast injection and insertion of a 0.025-inch guidewire. b After exchanging the guidewire for a CAPELLA 0.035, a catheter was inserted into the right hepatic duct. c A 7-Fr plastic stent is successfully placed without tract dilation.
To the best of our knowledge, this is the first report of EUS-HGS omitting tract dilation enabled by a novel 0.035-inch guidewire that is essential for this procedure.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogura T Higuchi K Endoscopic ultrasound-guided hepaticogastrostomy: Technical review and tips to prevent adverse events Gut Liver 20211519620510.5009/gnl 2009632694240 PMC 7960972 · doi ↗ · pubmed ↗
- 2Mukai S Itoi T Tsuchiya T One-step tract dilation using a novel long balloon catheter during endoscopic ultrasound-guided hepaticogastrostomy J Hepatobiliary Pancreat Sci 202431 e 38e 4038822454 10.1002/jhbp.12014 PMC 11503455 · doi ↗ · pubmed ↗
- 3Yamamoto Y Ogura T Nishioka N Risk factors for adverse events associated with bile leak during EUS-guided hepaticogastrostomy Endosc Ultrasound 2020911011532295968 10.4103/eus.eus_68_19PMC 7279085 · doi ↗ · pubmed ↗
- 4Ohno A Fujimori N Kaku T Feasibility and efficacy of endoscopic ultrasound-guided hepaticogastrostomy without dilation: A propensity score matching analysis Dig Dis Sci 2022675676568435689110 10.1007/s 10620-022-07555-z · doi ↗ · pubmed ↗