Cold snaring vs. standard forceps biopsy in sampling colorectal cancer: a comparative case report
Simona Agazzi, Eukene Rojo, Elena De Cristofaro, Jérôme Rivory, Thomas Walter, Tanguy Fenouil, Mathieu Pioche

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
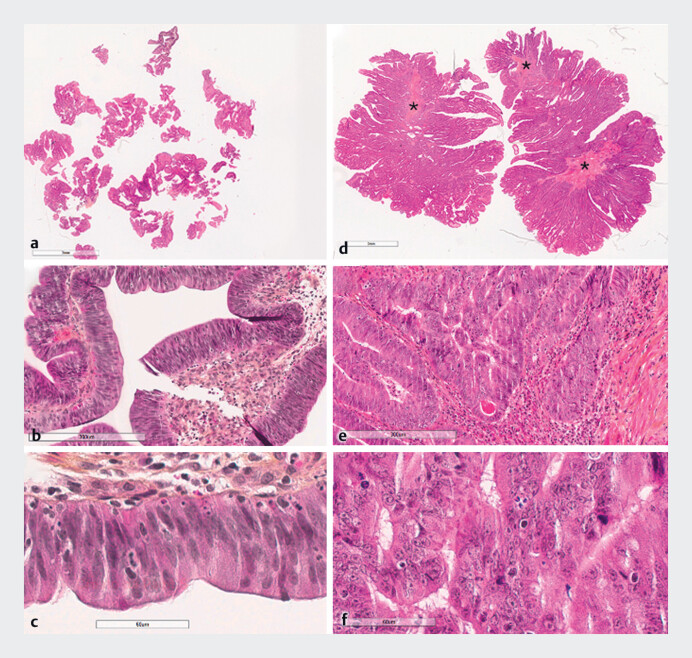 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Screening and Detection · Colorectal Cancer Surgical Treatments · Inflammatory Bowel Disease
An accurate histological diagnosis of colorectal cancer is essential for promptly establishing appropriate therapeutic management. Furthermore, nowadays larger samples are needed to evaluate immunological and genetic panels. For malignant lesions that cannot be removed endoscopically, the European Guidelines recommend taking six carefully targeted biopsies from the suspected cancer focus 1 . Despite advancements in endoscopic imaging, a retrospective study of 962 patients undergoing colorectal adenocarcinoma resection found that 29% (62/217) required repeat endoscopy due to sampling errors 2 , leading to a 1.36-fold increase in time to surgery (95% CI 1.20–1.54, p<0.001) and higher healthcare costs. Choi et al. found that positive diagnosis rates for the first, second, and third biopsy specimens of advanced colorectal cancer were 78.1%, 87.5%, and 93.8%, respectively, with no significant increase from additional biopsies 3 . Reducing biopsy numbers by increasing targeted tissue sample size through cold snaring could enhance diagnostic sensitivity, minimize repeat procedures, and reduce pathologist workload.
We report a case of a 58-year-old patient who underwent a colonoscopy that revealed a 5-cm macronodular lesion proximal to the hepatic flexure ( Video 1 ). The lesion was thoroughly evaluated using white light imaging, narrow band imaging, and underwater magnification. The major 15-mm nodule was characterized by a pit pattern VN (Kudo classification), suggesting invasive cancer.
Procedure comparing cold snare biopsy with standard forceps biopsy in sampling colorectal cancer.Video 1
The lesion was considered non-removable endoscopically. Biopsies were performed, six with forceps and one with cold snaring. The six biopsies with forcepss were stored in formalin in one container, while the snare biopsy was placed in a separate container. Pathologists conducted a blind analysis.
Histological examination of the cold snare biopsy revealed focal areas with glandular fusion, papillary structures, and necrotic foci, affirming adenocarcinoma developed within a tubulovillous adenoma with high grade intra-epithelial neoplasia ( Fig. 1 ). In contrast, forceps biopsies showed only high grade intraepithelial neoplasia due to fragmentation and superficiality, without evidence of adenocarcinoma.
Comparison of histopathological features. a–c Forceps biopsy. d–f Cold snare biopsy.
Endoscopy_UCTN_Code_TTT_1AQ_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pouw RE Bisschops R Endoscopic tissue sampling - Part 2: Lower gastrointestinal tract. European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 2021531261127310.1055/a-1671-633634715702 · doi ↗ · pubmed ↗
- 2Johnson GGRJ Hershorn O Sampling error in the diagnosis of colorectal cancer is associated with delay to surgery: a retrospective cohort study Surg Endosc 2022364893490234724583 10.1007/s 00464-021-08841-z PMC 8559691 · doi ↗ · pubmed ↗
- 3Choi Y Choi HS Optimal number of endoscopic biopsies in diagnosis of advanced gastric and colorectal cancer J Korean Med Sci 201227363910.3346/jkms.2012.27.1.3622219611 PMC 3247772 · doi ↗ · pubmed ↗