Infrarenal endovascular repair of abdominal aortic aneurysm with hostile aortic neck configuration by primary placement of an infrarenal Palmaz stent followed by an endoprosthesis with suprarenal fixation (the “Neoneck” technique)
André Pinheiro Ribeiro Alves, Queise da Costa Cettolin, Yasmin Falcon Lacerda, Mauricio de Amorim Aquino, Gustavo dos Santos Domingues

TL;DR
A new endovascular technique called 'Neoneck' is described to treat abdominal aortic aneurysms with challenging aortic neck angles, showing promising early results.
Contribution
The novel 'Neoneck' technique uses a Palmaz stent to rectify aortic neck angles before endoprosthesis placement in complex AAA cases.
Findings
All patients had immediate technical success with no migration, fracture, or type Ia endoleaks.
Aneurysmal sac reduction was observed after six months in treated patients.
The technique was feasible and effective in cases where open repair or ideal devices were not available.
Abstract
The Endovascular Repair (EVAR) is the first-choice technique for Abdominal Aortic Aneurysm (AAA). Treatment success is dependent on favorable anatomy and an adequate sealing zone formed by a straight aortic neck (slightly angled). Endoprostheses implanted at critical aortic angles (above 75º) may result in unfavorable results such as fracture, migration, and type Ia endoleak. The technique for creating a proximal “Neoneck” consists of implanting the Palmaz stent in the proximal neck of the AAA, before placement of the endoprosthesis, allowing remodeling and rectification of the aortic neck. To describe the “Neoneck” technique and report the early results of three cases with rectification of the proximal neck angle using a Palmaz stent, enabling treatment in these cases with angulated necks. We analyzed data collected from patients in whom Palmaz stents were placed, constructing a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1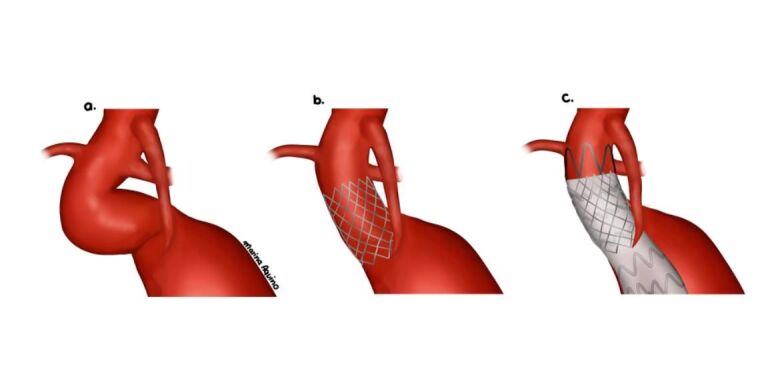 Figure 2
Figure 2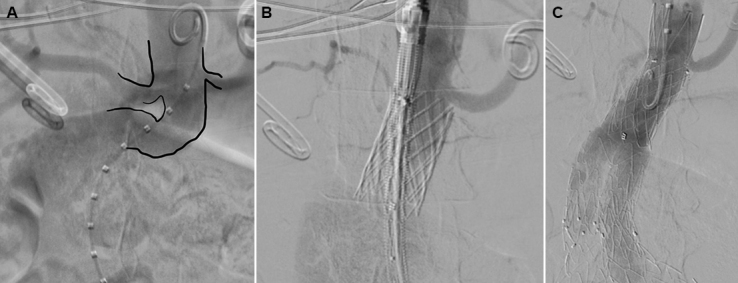 Figure 3
Figure 3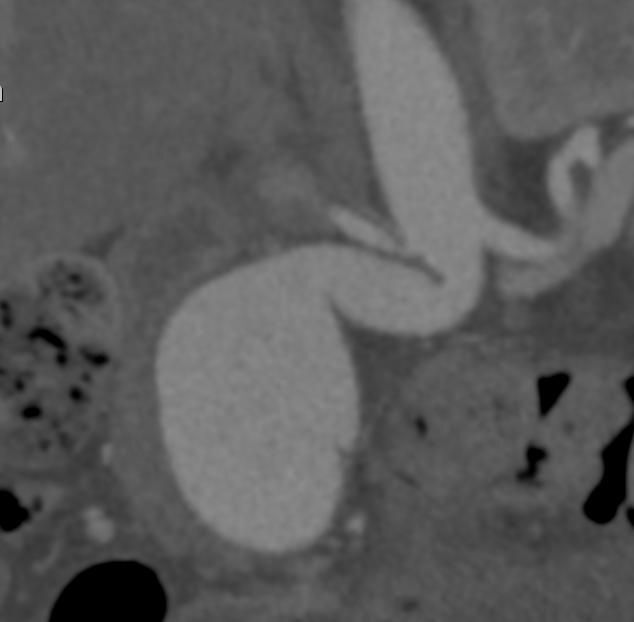 Figure 4
Figure 4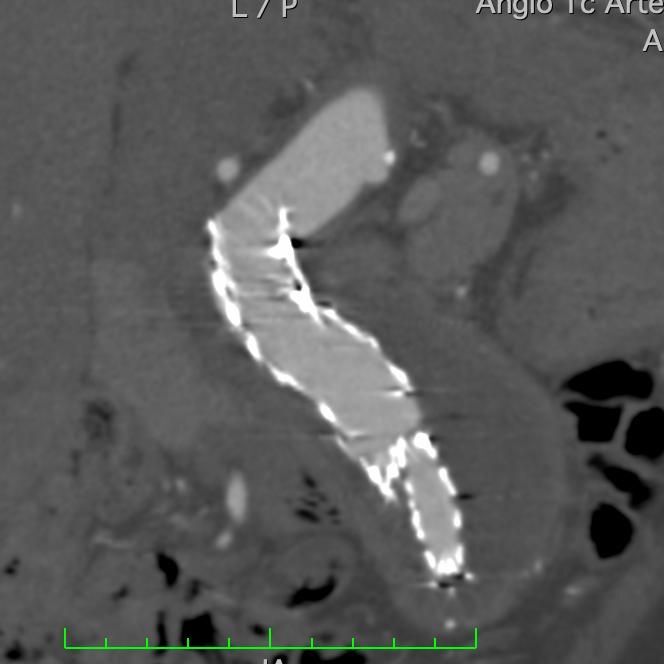 Figure 5
Figure 5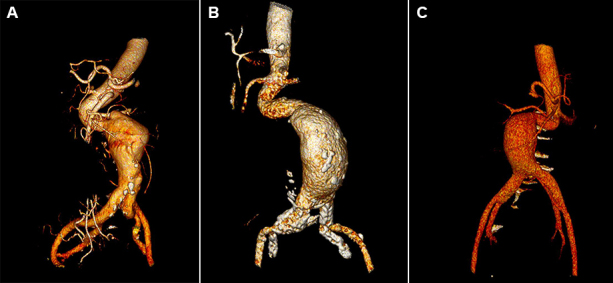 Figure 6
Figure 6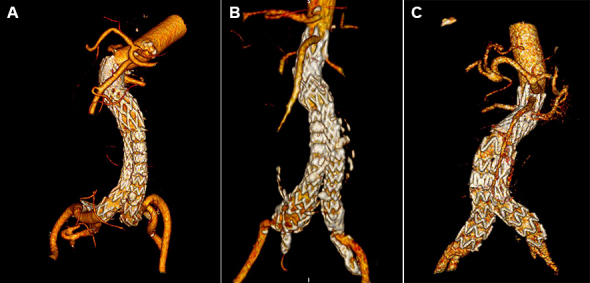 Figure 7
Figure 7|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|
| 1 | F/67y | SAH, CHF | Abdominal aortic aneurysm | 105 | 20 | 5.6 | Incraft/Cordis® | Palmaz (P4014/Cordis) | Maxi LD/Cordis® |
| 2 | F/62y | SAH, ovarian cancer | Dilated abdominal aortic dissection | 91 | 17 | 3.4 | E- tegra/Artvion® | Palmaz (P4014/Cordis) | Atlas/Bard® |
| 3 | F/94y | SAH | Abdominal aortic aneurysm | 93 | 18 | 3.8 | Incraft/Cordis® | Palmaz (P4014/Cordis) | Maxi LD/Cordis® |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic aneurysm repair treatments · Cardiac, Anesthesia and Surgical Outcomes · Aortic Disease and Treatment Approaches
INTRODUCTION
Infrarenal Abdominal Aortic Aneurysm (AAA) occurs in approximately 4% to 8% of the population.^1-3^ Endovascular aneurysm repair (EVAR) is the gold standard treatment^4-6^ and its success is fundamentally dependent on favorable anatomy, with an adequate sealing zone, preferably formed by a straight aortic neck (slightly angled), of adequate length, without calcifications or thrombi.^4,7,8^ In many cases, however, severe angles are seen in the proximal neck, representing an important obstacle to a satisfactory outcome of the infrarenal EVAR for AAA.^8^
Endoprostheses placed at critical angles (greater than 75º) may result in unfavorable results such as fracture, migration, type Ia endoleak, and even aneurysm rupture. When available, fenestrated/customized endoprostheses can be deployed for visceral arteries, allowing sealing at a proximal region of the aorta in a better aligned area, with a higher success rate. Unfortunately, the high cost of these devices and the time required to manufacture them (minimum of 15 days) often make their use impractical, especially in urgent situations.^8^
One technique recently developed for very tortuous necks involves making a proximal “Neoneck”. This resource consists of using a balloon-expandable Palmaz stent (P4014 Cordis®) implanted at the proximal neck of the AAA during the same surgical intervention, before placement of the endoprosthesis, allowing remodeling and rectification of the aortic neck for the subsequent infrarenal EVAR, thus avoiding type Ia endoleak.^9^ The Palmaz stent is traditionally used to correct type Ia endoleaks in settings in which sealing is difficult, aiming to increase the radial force exerted by the prosthesis on the proximal neck and maximize its contact with the aortic wall.^10,11^ In the method described, however, the stent is deployed prior to endoprosthesis placement, straightening the aortic neck for a better fit and EVAR success.^9^
This study aims to describe the “Neoneck” technique and report the early results of three cases of infrarenal aortic aneurysms treated at a specialized center for treatment of aortic diseases in Salvador, Bahia, Brazil, with endovascular repair in conjunction with preparatory rectification of the tortuosity of the proximal aortic neck using a Palmaz stent, creating a straight Neoneck and enabling EVAR.
METHODS
Study design
A retrospective analysis was performed based on data collected from three patients in whom Palmaz stents were placed, constructing a proximal “Neoneck”, during EVAR for infrarenal AAA with very tortuous proximal aortic necks, from December 2021 to July 2023.
Patients
Patients were included with aneurysmal dilatation of the infrarenal abdominal aorta (whether aneurysm or dilated dissection) who had a proximal neck with severe angulation (greater than 75º), in whom it was necessary to construct a new neck with a steel stent to allow adequate EVAR.
Data were collected and analyzed on demographics, anatomy (including extension, diameter, and angulation of aortic neck), devices deployed for treatment, besides perioperative results and treatment follow-up in acute and subacute settings, including immediate and late postoperative success rates, complications – in particular, endoleaks –, morbidity, mortality, and patency in the short and medium term.
All patients were treated at a single center, and the signed consent was obtained from all. This study was approved by the Research Ethics Committee at the HGRS (Ethics Appraisal Submission Certificate: 69734323.1.0000.5028, Consolidated Opinion: 6.574.411).
The Neoneck technique
For treatment, we used the balloon-expandable Palmaz stent (P4014/Cordis®) mounted on Maxi LD/Cordis® or Atlas/Bard® balloon catheters, employing an average graft oversizing of 10 to 20% of the proximal neck diameter, followed by placement of suprarenal fixation endoprostheses, employing an oversizing of approximately 20% of the diameter of the proximal aortic neck.
All patients underwent femoral access by surgical dissection. Initially, a 14F x 40cm sheath was placed in the common femoral artery. Subsequently, a 0.035 ” x 260cm extra-stiff guidewire was passed through the femoral access, followed by previous assembly of the Palmaz stent on a Maxi LD/Cordis® or Atlas/Bard® balloon catheter. To avoid migration of the stent over the balloon during passage through the femoral introducer valve, the balloon was slowly inflated outside the patient, creating resistance to distal migration of the stent (Figure 1). Then, positioning angiography was performed, and the Palmaz stent mounted on the balloon catheter was implanted in an infrarenal position (Figure 2). Finally, the standard technique for endovascular treatment of the AAA was performed, with placement of the bifurcated endoprosthesis.
Image depicting the balloon partially inflated before passing through the femoral introducer sheath, creating resistance to distal migration of the Palmaz stent.
Schematic drawing demonstrating the technique for creating a Neoneck with a Palmaz stent prior to EVAR.
Pre-treatment and control CT angiography (AngioCT) were performed in the bioimaging department of the HGRS, at intervals of 1, 3, and 6 months postoperative. The images were analyzed using Osirix software®.
Definitions
Technical success is defined as evidence of total aneurysm exclusion on the control intraoperative angiography, without type Ia (proximal neck) or type III (material and device connections) endoleaks, and maintenance of patency of visceral arteries. Late postoperative success is defined as maintenance of these results on control CT scans after 1 and 6 months.
Statistics
Continuous data were expressed as mean ± standard deviation or median and interquartile range, if the distribution was not normal. Categorical data were expressed as counts and percentages.
Considering the references in the literature, with a prevalence of 4-8% of Infrarenal Abdominal Aortic Aneurysms, of which approximately 48-53% have hostile necks, with a sampling error of 5% and a 95% confidence interval, an ideal sample size of 399 patients was found. This study describes the technique and the initial experience of the first three cases treated at the service, without a sufficient number for an ideal sample. The STROBE protocol was followed.
RESULTS
Between December 2021 and July 2023, three patients with AAA with a very tortuous proximal aortic neck underwent EVAR using the Neoneck technique (Table 1).
Analyzing demographic data, in regards to sex, all patients were female. All patients had significant comorbidities and/or advanced age that restricted the choice of open repair due to unfavorable prognosis. Systemic arterial hypertension was the most prevalent pathology, present in all patients. Mean age was 74.3 years (62-94 years) and median age was 67 years.
Regarding aortic pathology and anatomy, two patients had AAA and one patient had an isolated dilated dissection of the abdominal aorta. The mean diameter of the aortic dilation was 6.3cm (4.8-8.0cm) and the median diameter was 6.1cm. The mean length of the proximal neck was 4.3cm (3.4-5.6cm) and the median length was 3.8cm. The mean angle was 96 degrees (91º-105º) and the median angle was 93º.
Regarding femoral access, all patients had femoral arteries with acceptable caliber (mean 8mm) and no significant calcifications.
All procedures in this series were performed with technical success (Figure 3). Mean fluoroscopy time was 81 minutes (60-97 min). There were no cases of migration, fracture, or type IA endoleak. The average volume of iodinated contrast used was 120mL and none of the patients had renal dysfunction after surgery.
Intraoperative angiography images. A) First, showing a tortuous aortic neck. B) Second, primary Palmaz stent already released, before the endoprosthesis is deployed, showing rectification of the proximal neck. C) Third, Palmaz stent and endoprosthesis already placed, with no evidence of type Ia endoleak.
During follow-up with CT angiography (Figures 4-7), an 8% median reduction of the aneurysmal sac was observed on the imaging exams performed after six months of follow-up.
Preoperative CT angiography image showing tortuous aortic neck.
CT angiography image 30 days after EVAR with the Neoneck technique, showing rectification of the aortic neck, with no endoleaks.
Preoperative 3D CT angiography reconstructions showing tortuous aortic neck. (A) 3D CT reconstruction of the first patient; (B) 3D CT reconstruction of the second patient; (C) 3D CT reconstruction of the third patient.
Postoperative 3D CT angiography reconstructions, 30 days after EVAR with the Neoneck technique. (A) 3D CT reconstruction of the first patient treated; (B) 3D CT reconstruction of the second patient treated; (C) 3D CT reconstruction of the third patient treated.
There were no complications related to surgical access and/or deaths registered during this case series.
DISCUSSION
There is no denying the advances achieved in EVAR over recent years. The improvements in techniques and devices have enabled inclusion of an increasing number of cases that are now treatable with this technique. However, the success of EVAR is dependent on favorable anatomy with an adequate sealing zone. Hostile aortic necks tend to make it difficult to anchor the devices, making type IA endoleaks more likely and increasing the risk of aneurysmal sac rupture and death.^4,8^
In cases of anatomies prohibitive for EVAR, open surgical repair should still be recommended, with excellent results in eligible patients.^4^ However, AAA is very prevalent in elderly patients with comorbidities that may be limiting, such as heart and lung diseases. A significant part of this population may have important risk factors that restrict the choice of open repair due to a high risk of perioperative complications and death.^1,2,4^
The only devices for highly angulated aortic necks (up to 90º) approved for use in Brazil were the Anaconda/Terumo® and the Aorfix/Endovastec®. The first has not been available in Brazil since 2021 and the second is unfortunately not available for use at our service. Recently, Gore® launched endoprostheses capable of accommodating large aortic angles, although the abdominal device is not yet available in Brazil. For this reason, over the years, several techniques have been developed and refined to allow endovascular treatment, even in cases of severe angulation, achieving adequate proximal sealing in EVAR.
In 2013, Chisci et al.^9^ published a case report using the E-XL/Artivion® transrenal stent as a way to treat and prevent type Ia endoleaks in patients with tortuous aortic necks undergoing EVAR. After 15 months’ follow-up there was no evidence of proximal endoleaks. However, it is important to emphasize that the presence of a stent in the transrenal topography can make future approaches more difficult if there is a need to cover visceral arteries and the risks and benefits of its use must therefore be weighed up. In 2017, Takayama et al.^12^ published a proposed technique for angulated necks, using the directional control mechanism of the tip of a C3 Excluder/Gore endoprosthesis® to achieve better fit in the tortuous aortic neck, without evidence of endoleak at 6 months. This method is still experimental, with few reported cases, and no strict definition of which cases are favorable for it and with evident limitations depending on the device used, such as stent grafts with nose cones or suprarenal fixation.
Most of the literature on the Palmaz stent describes its use for correcting type Ia endoleaks in angled aortic necks, after endoprosthesis placement, either at the same surgical intervention or in surgical reapproaches after CT control scans show leakage.^9-11^ There is scant literature on the primary use of stents to remodel the proximal neck and rectify angulation immediately before implantation of the prosthesis. One of the advantages of this preparatory stent placement is to avoid “overballooning” of the proximal neck and to avoid possible dissections and ruptures, since the aortic anatomical configuration has been positively modified, ensuring good circumferential apposition of the prosthesis material to the aortic wall.^9^
Considering the small number of published studies in which the Palmaz stent is previously implanted in the aorta, the main idea of previously implanting the Palmaz stent in an infrarenal position is precisely not to interfere with the fixation of the endoprosthesis, considering that we only use suprarenal fixation devices. With regard to the relationship between the endoprosthesis material and the stent mesh, in this small series we did not identify any interference.
The global literature suggests that the E-XL transrenal stent® (not available in Brazil) is preferred over the Palmaz stent for rectifying the aortic neck, as it is more flexible.^9,10^ This is due to the E-XL’s hybrid nitinol configuration, with an open-cell design in the middle, closed at both ends, constant external radial force along the length of the device. In contrast, the shorter closed cells of the Palmaz stent, made of stainless steel, do not allow such a constant external radial force.^11^ In addition, endoprostheses may continue to expand as the aorta degenerates in one third of patients, generating an enlargement of the neck, with a risk of loss of Palmaz stent apposition to the endoprosthesis, and consequent loss of the proximal sealing zone.^11^ However, as the E-XL stent has a more adequate external radial force, it usually accommodates degenerative neck dilation better, ensuring good apposition and sealing of the graft. The Palmaz stent was deployed in the present study because it is the only option available in Brazil.
Despite being a less invasive treatment than open repair, EVAR employed in cases of unfavorable anatomy, such as hostile aortic necks, generally progresses to a greater need for reinterventions and associated complications.^4^ Use of the Neoneck Palmaz stent technique is presented, both in the literature and in this case series, as a suitable option, with fewer reapproaches in the short and medium term.^9^ However, studies with larger samples and longer follow-up are not yet available to assess the long-term behavior and confirm the most favorable evolution.
The health department where the described treatments were carried out is accredited by the Brazilian Unified Health System (SUS), providing care free of charge, where access to materials is subject to financial limitations. It is often not possible to use the most modern and suitable current devices available or to perform treatments considered gold standard for complex aortic pathologies. In this scenario of limited expenditure, combined with cases of unfavorable aortic angulation and patients with clinical conditions that limit open surgical repair, primary use of the Palmaz stent seems to represent a viable option.
Despite the reduced sample size and brief follow-up time, the data presented in this initial experiment suggest that the “Neoneck” is a promising, effective, technique with a satisfactory rate of technical success (100%), with no evidence of migration and/or type IA endoleak.
CONCLUSION
This paper presents a series of cases in which the Neoneck technique was feasible and achieved a high rate of technical success, with favorable results in the short and medium term. Prospective studies with long-term clinical follow-up are still needed to fully assess the safety of the technique and validate it.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ashton HA Buxton MJ Day NE et al The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: a randomized controlled trial Lancet 200236093451531153910.1016/S 0140-6736(02)11522-412443589 · doi ↗ · pubmed ↗
- 2Bown MJ Sutton AJ Bell PRF Sayers RD A meta-analysis of 50 years of ruptured abdominal aortic aneurysm repair Br J Surg 200289671473010.1046/j.1365-2168.2002.02122.x 12027981 · doi ↗ · pubmed ↗
- 3Hoornweg LL Storm-Versloot MN Ubbink DT Koelemay MJ Legemate DA Balm R Meta analysis on mortality of ruptured abdominal aortic aneurysms Eur J Vasc Endovasc Surg 200835555857010.1016/j.ejvs.2007.11.01918226567 · doi ↗ · pubmed ↗
- 4Patel R Sweeting MJ Powell JT Greenhalgh RM Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomized controlled trial Lancet 2016388100582366237410.1016/S 0140-6736(16)31135-727743617 · doi ↗ · pubmed ↗
- 5Mendonça CT Moreira RCR Timi JRR et al Comparison between open and endovascular treatment of abdominal aortic aneurysms in high-risk patients J Vasc Bras 20054232242
- 6Mendonça CT Moreira RCR Carvalho CA Moreira BDA Weingärtner J Shiomi AY Endovascular treatment of abdominal aortic aneurysms in high surgical risk patients J Vasc Bras 200981566410.1590/S 1677-54492009000100009 · doi ↗
- 7Matsumura JS Brewster DC Makaroun MS Naftel DC A multicenter controlled clinical trial of open versus endovascular treatment of abdominal aortic aneurysm J Vasc Surg 200337226227110.1067/mva.2003.12012563194 · doi ↗ · pubmed ↗
- 8Schanzer A Greenberg RK Hevelone N et al Predictors of abdominal aortic aneurysm sac enlargement after endovascular repair Circulation 2011123242848285510.1161/CIRCULATIONAHA.110.01490221478500 · doi ↗ · pubmed ↗