Cytomegalovirus Gastritis Mimicking a Gastroesophageal Junction Malignancy in an AIDS Patient: A Case Report
Connor Lovingood, Nancy Jhanji, William K Oelsner, James E Pitcher, Laxmi Parsa

TL;DR
This case report describes a rare instance of CMV gastritis in an AIDS patient that mimicked a cancerous tumor at the stomach-esophagus junction.
Contribution
The novelty lies in highlighting the rare endoscopic presentation of CMV gastritis at the gastroesophageal junction and its potential to mimic malignancy.
Findings
CMV gastritis can present with endoscopic features resembling malignancy in AIDS patients.
Immunohistochemistry is essential for accurate diagnosis of CMV gastritis.
CMV ulcers at the GE junction are occasionally associated with underlying malignancy.
Abstract
Cytomegalovirus (CMV) gastritis is a rare opportunistic infection that often affects immunosuppressed patients. It is a DNA virus belonging to the Herpes family most commonly spread through contaminated bodily fluids such as blood, urine, saliva, tears, breast milk, semen, and vaginal fluids. Here, we present a case of a newly diagnosed HIV-positive patient with acquired immunodeficiency syndrome (AIDS) found to have a gastroesophageal (GE) junction ulceration with endoscopic characteristics suggestive of malignancy due to CMV gastritis in the absence of underlying malignancy. Most immunocompetent patients experience mild or no symptomatology and thus often require no treatment. On the contrary, immunosuppressed patients may be greatly affected by CMV including death. Because of this, it is necessary to treat and potentially prophylax against CMV within this population depending on the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
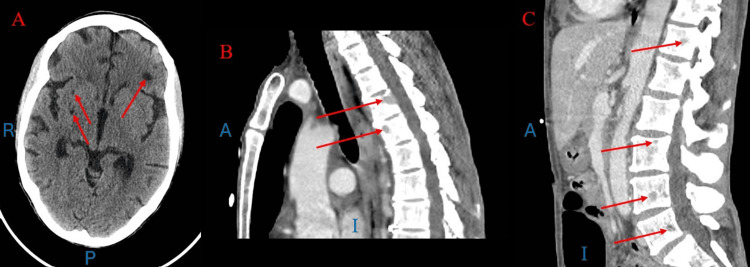 Figure 1
Figure 1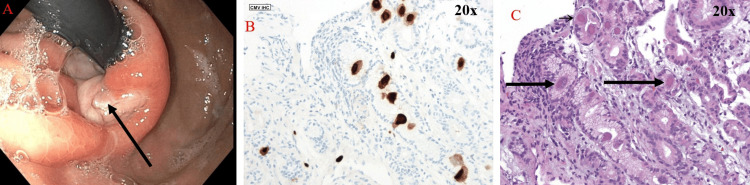 Figure 2
Figure 2| Lab | Patient Values | Reference Range |
| Sodium | 129 mmol/L | 136-145 mmol/L |
| Potassium | 3.5 mmol/L | 3.5-5.1 mmol/L |
| Calcium | 7.9 mg/dL | 8.9-10.8 mg/dL |
| Chloride | 98 mmol/L | 98-107 mmol/L |
| Bicarb | 25 mmol/L | 22-31 mmol/L |
| BUN | 15 mg/dL | 7-26 mg/dL |
| Creatinine | 0.4 mg/dL | 0.6-1.1 mg/dL |
| Glucose | 79 mg/dL | 80-99 mg/dL |
| AST | 11 U/L | 5-34 U/L |
| ALT | 20 U/L | 3-55 U/L |
| ALP | 72 U/L | 40-150 U/L |
| T. Protein | 6.3 g/dL | 6-8.3 g/dL |
| Albumin | 2.7 g/dL | 3.5-5 g/dL |
| T. Bilirubin | 0.4 mg/dL | 0.2-1.2 mg/dL |
| Hemoglobin | 7.7 g/dL | 12-16 g/dL |
| WBCs | 5 Th/mm3 | 4.8-10.8 Th/mm3 |
| Platelets | 314 Th/mm3 | 130-400 Th/mm3 |
| INR | 1.01 | 1.00 |
| APTT | 29 Sec | 25.1-36.5 Sec |
| Iron saturation | 11.7% | 20-50% |
| Serum Iron | 19 ug/dL | 40-145 ug/dL |
| TIBC | 163 ug/dL | 226-426 ug/dL |
| Transferrin | 124 mg/dL | 191-379 mg/dL |
| Ferritin | 584.5 ng/dL | 11-306.8 ng/dL |
| LDH | 172 U/L | 117-242 U/L |
| Haptoglobin | 380 mg/dL | 33-346 mg/dL |
| Ammonia | 41 umol/L | 16-53 umol/L |
| TSH | 12.042 uIU/mL | 0.34-5.60 uIU/mL |
| T4, free | 0.57 ng/dL | 0.54-1.24 ng/dL |
| CD4 | 34 cells/uL | 359-1519 cells/uL |
| HIV-1 RNA PCR | 788,000 copies RNA/mL | <20 copies RNA/mL |
| Cryptococcus | NEGATIVE | NEGATIVE |
| Hepatitis panel | NON-REACTIVE | NON-REACTIVE |
| RPR | NON-REACTIVE | NON-REACTIVE |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Viral-associated cancers and disorders · Herpesvirus Infections and Treatments
Introduction
Cytomegalovirus is a DNA virus that belongs to the Herpesviridae family with a wide seroprevalence range depending on the source of 40-100% [1]. CMV rarely affects immunocompetent individuals but usually presents with symptoms common in mononucleosis such as fever, chills, fatigue, lymphadenopathy, splenomegaly, nausea/vomiting, and general malaise. It is usually self-resolving within a few weeks. Immunocompromised patients from a variety of medical illnesses or undergoing certain treatments including those with HIV/AIDS and CD4 counts less than 50 are more commonly affected as the virus undergoes reactivation. Clinical presentations are typically more severe for these patients and may include esophagitis, gastritis, gastric ulcer, gastroparesis, pancreatitis, ileitis, appendicitis, proctitis, and colonic obstruction. The virus is more likely to undergo reactivation in the setting of immunocompromise leading to a wide range of clinical manifestations including those aforementioned along with encephalitis, pneumonitis, retinitis, and fulminant hepatitis [2]. The most common CMV gastrointestinal manifestation is colitis [1]. However, CMV gastritis has also been recorded in the literature, although much more infrequent [1,3-7]. In this case report, a newly diagnosed HIV-positive patient with AIDS was found to have a malignant appearing gastroesophageal junction ulceration due to CMV gastritis in the absence of esophagitis or underlying malignancy. The location of the lesion in this patient is what makes this case exceptionally rare as an isolated ulceration caused by CMV at the gastroesophageal junction in the absence of esophagitis has only been documented a handful of times in the literature. The objective of this case report is to highlight a rare variation of CMV gastritis.
Case presentation
A 60-year-old woman with a past medical history of recently diagnosed HIV with AIDS, pancytopenia, B12 and folate deficiency, irritable bowel syndrome, colon polyps, and hypothyroidism presented with acute encephalopathy, gait instability, and failure to thrive. She was admitted with hyponatremia, anemia, and malnutrition. The patient had been diagnosed with HIV one month prior; however, she had not started antiretroviral therapy or infection prophylaxis. CMV does not routinely require empiric prophylaxis in AIDS patients given its overall low incidence. Her outpatient labs confirmed a diagnosis of AIDS with a CD4 count of 34, placing her at risk of several opportunistic infections including CMV, and HIV RNA >700,000 two weeks prior (Table 1).
At the time of admission, labs were notable for sodium of 129 and hemoglobin of 7.7 with a previous baseline of around 10 (Table 1). CT brain showed focal hypodensities in the left frontal region and right basal ganglia; however, MRI was negative for demyelination or other acute abnormalities (Figure 1A). CT chest/abdomen/pelvis showed numerous lytic lesions concerning metastatic disease, later discovered to most likely be related to disseminated infection with CMV as they were not present in the CT scan two months prior (Figures 1B, 1C). The patient reported difficulty eating due to nausea and dysphagia. A review of systems was negative for vomiting, fevers, diarrhea, constipation, melena, hematochezia, or hematemesis. The patient denied any NSAID, anticoagulation, or antiplatelet use. She reported no alcohol, smoking, or illicit drug use. Her last colonoscopy was three years prior with multiple small polyps, and she had no prior esophagogastroduodenoscopy (EGD). During admission, she was evaluated by infectious disease and started on fluconazole 200mg daily for seven days for oropharyngeal candidiasis as well as trimethoprim-sulfamethoxazole DS daily for P. jirovecii prophylaxis and a multivitamin.
Panel A: Hypodensities in the L frontal and R basal ganglia regions from CT brain without contrast. Panels B and C: Numerous lytic lesions concerning for disseminated infection vs metastatic disease. Panel B at the levels of T4-T5 and Panel C at the levels of T12, L3-L5 from CT chest, abdomen, and pelvis with contrast.Blue letters represent the orientation of the image; R: Right; P: Posterior; A: Anterior; I: Inferior
Gastroenterology was consulted for further evaluation of failure to thrive and dysphagia. She endorsed a 55-pound weight loss over three months in addition to iron deficiency anemia and epigastric pain. An EGD was performed and showed a normal-appearing esophagus with erythematous mucosa throughout the stomach along with a large ulceration at the GE junction with findings concerning for malignancy including a rolled, irregular border, seemingly deep tissue invasion, and pale color (Figure 2A). Pathological examination revealed CMV inclusion bodies without evidence of malignancy (Figures 2B, 2C) and the patient was started on IV valganciclovir 900mg twice daily for six weeks and proton-pump inhibitor therapy daily. At this time, she also began HIV treatment with bictegravir 50mg/emtricitabine 200mg/tenofovir alafenamide 25mg.
Panel A showing gross depiction via endoscopy of malignant-appearing, non-bleeding, cratered ulceration measuring 2mm in largest dimension at GE junction. Panel B 20x photomicrograph of biopsied ulcer with immunohistochemical staining for CMV inclusion bodies. Panel C 20x photomicrograph of biopsied ulcer with CMV inclusion bodies.GE: Gastroesophageal; CMV: Cytomegalovirus
The patient was discharged to a skilled nursing facility with a subsequent presentation two weeks later for recurrent falls and failure to thrive. The patient elected to transition to hospice care at that time and forwent additional work-up.
Discussion
Immunocompromised patients with HIV have nearly double the lifetime risk of esophageal and gastric cancers as CMV proteins are often present in cancer cells and have been shown to cause epithelial transformation via the presence of oncogenes, increase local inflammation, and promote tumor angiogenesis [8]. CMV has also been shown to be present in the prostate, breast, B-cell lymphoma, and glioblastoma [9]. However, opportunistic infections can often present with signs and symptoms similar to malignancy in patients with severe immunosuppression [5]. Here, we present a case of a malignant appearing GE junction ulceration that was found to be CMV gastritis. Mucosal ulceration is typically caused by local invasion into the endothelium leading to vasculitis, ischemia, and tissue necrosis.
CMV gastritis is extremely rare and a largely undiagnosed disease, often found in the setting of disseminated infection [1]. In advanced disease, CMV is known to create pseudo-malignancies and ulcerations [10,11]. While CMV colitis is the predominant clinical phenotype, upper GI manifestations have also been reported [1,6]. One retrospective study by Marques et al. found the gastric antrum (42%) and lower esophagus (33%) to be the most common sites of CMV disease in the upper GI tract [3]. The location of our patient’s ulceration at the GE junction is exceedingly rare.
Currently, there are few case reports of CMV ulcerations at the GE junction. However, of the three reports in the literature, one patient had a CMV pseudo-malignant mass, while the other two patients had an underlying hematologic malignancy [12,13]. While our patient was not diagnosed with malignancy, she was subsequently found on re-hospitalization to have lytic bone lesions, suggestive of an opportunistic infection versus undiagnosed malignancy. While CMV is currently not known to have malignant transformation, it has been shown to be a risk factor for post-transplant lymphoproliferative disease in conjunction with Epstein-Barr virus infection [14]. It is interesting to note the observed association of CMV ulcers at the GE junction with underlying hematologic malignancies.
Conclusions
In summary, this case report highlights the importance of maintaining a broad differential and considering CMV gastritis for gastric ulcerations in immunocompromised patients, particularly those with advanced HIV or T-cell dysfunction. The rarity of our patient’s lesion at the GE junction underscores the need for heightened clinical suspicion and thorough evaluation given its potential to mimic malignancy. Moreover, CMV reactivation is a known risk factor for lymphoproliferative disease, and patients with CMV gastritis may have concurrent hematologic malignancies necessitating repeat endoscopy and biopsy pending overall clinical suspicion as no current guidelines exist at this time. Lastly, this case emphasizes the importance of early initiation of antiretroviral therapy in HIV-positive patients to reduce the risk of opportunistic infections and improve overall outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical characteristics of cytomegalovirus gastritis: a retrospective study from a tertiary medical center Medicine (Baltimore) Chen D Zhao R Cao W 099202010.1097/MD.0000000000018927 PMC 700459532000406 · doi ↗ · pubmed ↗
- 2Cytomegalovirus hepatitis in immunocompetent and immunocompromised hosts J Clin Transl Hepatol Da Cunha T Wu GY 106115920213360426110.14218/JCTH.2020.00088 PMC 7868697 · doi ↗ · pubmed ↗
- 3Cytomegalovirus disease of the upper gastrointestinal tract: a 10-year retrospective study GE Port J Gastroenterol Marques S Carmo J Pinto D Bispo M Ramos S Chagas C 2622682420172925576610.1159/000479232 PMC 5731150 · doi ↗ · pubmed ↗
- 4Cytomegalovirus gastritis in a patient with severe acute respiratory syndrome coronavirus 2 infection: a case report and literature review Respir Med Case Rep Taherifard E Mortazavi R Mokhtari M Taherifard A Kiani Salmi S Taherifard E 1016443720223539255010.1016/j.rmcr.2022.101644 PMC 8975752 · doi ↗ · pubmed ↗
- 5Cytomegalovirus infective gastritis in an immunocompetent host misdiagnosed as malignancy on upper gastrointestinal endoscopy: a case report and review of literature Hum Pathol Xiong X Liu F Zhao W Ji X Chen W Zou H Li F 1071129220193058489210.1016/j.humpath.2018.12.005 · doi ↗ · pubmed ↗
- 6CMV-related gastric ulcer and gastroduodenitis in an immunocompetent patient: a case report and literature review Case Rep Gastrointest Med Beany A Rainis T 3513223202120213480461710.1155/2021/3513223 PMC 8604585 · doi ↗ · pubmed ↗
- 7Cytomegalovirus associated with gastric ulcer: case report and literature review Gastroenterol Hepatol Martínez Huguet C Arguedas Lázaro Y Del Valle Sánchez E Omiste Sanvicente T Bernal Monterde V Montoro Huguet M 25625842201910.1016/j.gastrohep.2018.05.01430007786 · doi ↗ · pubmed ↗
- 8Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis Lancet Grulich AE Van Leeuwen MT Falster MO Vajdic CM 5937020071761727310.1016/S 0140-6736(07)61050-2 · doi ↗ · pubmed ↗