Characteristics, treatment patterns, and biomarker testing of patients with advanced RET fusion-positive non-small cell lung cancer in a real-world multi-country observational study: a brief report
Urpo Kiiskinen, Grace Segall, Hollie Bailey, Cameron Forshaw, Tarun Puri

TL;DR
This study examines real-world data on patients with RET fusion-positive non-small cell lung cancer, focusing on their clinical features, biomarker testing, and treatment approaches across multiple countries.
Contribution
The study provides real-world insights into RET fusion-positive non-small cell lung cancer patients, emphasizing the importance of biomarker testing and targeted therapies.
Findings
RET fusion-positive patients were more likely to be White/Caucasian, never smokers, and have adenocarcinoma.
Only 31% of advanced NSCLC patients were tested for RET fusions, with 84% of results available before treatment initiation.
The RET fusion-positive cohort showed less use of immunotherapy or targeted therapy compared to the overall cohort.
Abstract
Approximately 1−2% of non-small cell lung cancers (NSCLCs) are positive for rearranged during transfection (RET) gene fusions. The aim of this real-world multi-national study was to describe clinical characteristics, biomarker testing, and treatment patterns of patients with RET fusion-positive NSCLC. This observational study was conducted in 2020 in nine countries using electronic patient record forms, following Adelphi Disease Specific Programme (DSP™) methodology. Patients with advanced NSCLC (aNSCLC) were included in the overall cohort. A smaller RET fusion-positive cohort comprised patients from the overall aNSCLC cohort who had RET fusion-positive disease and no other co-alterations, plus an oversample of patients with RET fusion-positive disease and no other co-alterations. Patient characteristics were generally similar between the overall aNSCLC cohort (n=2947) and the RET…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
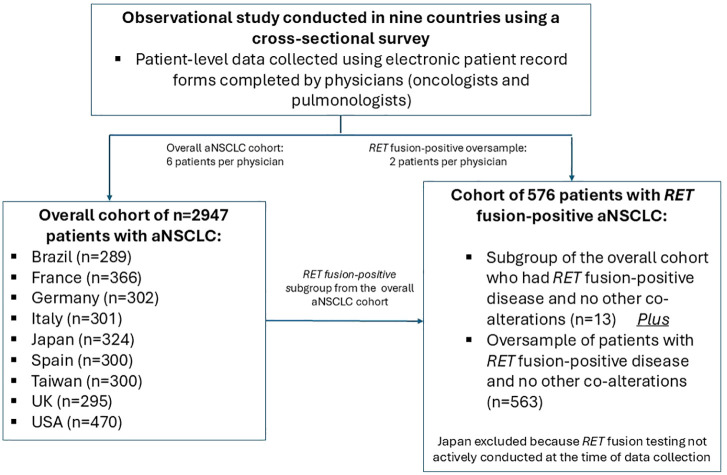 Figure 1
Figure 1| Characteristic | Overall aNSCLC (n=2947) |
| ||
|---|---|---|---|---|
| Age, median (IQR), years | 67 | (60−72) | 65 | (57−70) |
| Sex, n (%) | ||||
| Male | 1788 | (61) | 327 | (57) |
| Female | 1159 | (39) | 249 | (43) |
| Ethnic origin, n (%) | ||||
| White/Caucasian | 2017 | (68) | 486 | (84) |
| Japanese | 324 | (11) | 0 | (0) |
| Han Chinese | 293 | (10) | 27 | (5) |
| African American | 76 | (3) | 12 | (2) |
| Hispanic/Latino | 50 | (2) | 13 | (2) |
| Other | 187 | (6) | 38 | (7) |
| Smoking status, n (%) | ||||
| Current smoker | 455 | (15) | 46 | (8) |
| Former smoker | 1779 | (60) | 306 | (53) |
| Never smoked | 669 | (23) | 208 | (36) |
| Unknown | 44 | (1) | 16 | (3) |
| Disease stage at initial diagnosis, n (%) | ||||
| Stage I | 50 | (2) | 1 | (<1) |
| Stage II | 101 | (3) | 16 | (3) |
| Stage III | 634 | (22) | 81 | (14) |
| IIIA | 96 | (3) | 6 | (1) |
| IIIB | 337 | (11) | 33 | (6) |
| IIIC | 201 | (7) | 42 | (7) |
| Stage IV | 2138 | (73) | 471 | (82) |
| Unknown/not assessed | 24 | (1) | 7 | (1) |
| Histology, n (%) | ||||
| Adenocarcinoma | 2064 | (70) | 509 | (88) |
| Squamous cell carcinoma | 746 | (25) | 36 | (6) |
| Large cell carcinoma | 93 | (3) | 24 | (4) |
| Other | 33 | (1) | 6 | (1) |
| Unknown/not assessed | 11 | (<1) | 1 | (<1) |
| ECOG PS score at advanced diagnosis, n (%) | (base n=2941) | |||
| 0−1 | 2292 | (78) | 458 | (80) |
| 2 | 431 | (15) | 69 | (12) |
| ≥3 | 183 | (6) | 44 | (8) |
| Unknown/not assessed | 35 | (1) | 5 | (1) |
| Presence of CNS metastases at any time (primary site), n (%) | (base n=2439) | (base n=518) | ||
| Brain | 189 | (8) | 30 | (6) |
| Other CNS | 54 | (2) | 24 | (5) |
| Presence of CNS metastases at any time (secondary site), n (%) | (base n=2439) | (base n=518) | ||
| Brain | 228 | (9) | 32 | (6) |
| Other CNS | 72 | (3) | 19 | (4) |
| PD-L1 expression, n (%) | ||||
| <1% | 560 | (19) | 179 | (31) |
| 1−49% | 1182 | (40) | 248 | (43) |
| ≥50% | 692 | (23) | 66 | (11) |
| Unknown/not assessed | 513 | (17) | 83 | (14) |
| Parameter | Overall aNSCLC | USA | Brazil (n=289) | UK | Italy | France (n=366) | Spain (n=300) | Germany (n=302) | Taiwan (n=300) | Japan (n=324) |
|---|---|---|---|---|---|---|---|---|---|---|
| Biomarkers tested, n (%) | ||||||||||
| RET | 899 (31) | 313 (67) | 85 (29) | 52 (18) | 82 (27) | 147 (40) | 86 (29) | 62 (21) | 25 (8) | 47 (15) |
| PD-L1 | 2487 (84) | 392 (83) | 216 (75) | 277 (94) | 278 (92) | 349 (95) | 288 (96) | 218 (72) | 220 (73) | 249 (77) |
| EGFR | 2461 (84) | 419 (89) | 210 (73) | 235 (80) | 266 (88) | 297 (81) | 251 (84) | 246 (81) | 270 (90) | 267 (82) |
| ALK | 2294 (78) | 391 (83) | 190 (66) | 235 (80) | 264 (88) | 289 (79) | 245 (82) | 210 (70) | 236 (79) | 234 (72) |
| ROS1 | 1881 (64) | 364 (77) | 131 (45) | 189 (64) | 223 (74) | 244 (67) | 229 (76) | 137 (45) | 188 (63) | 176 (54) |
| KRAS | 1200 (41) | 336 (71) | 100 (35) | 95 (32) | 105 (35) | 240 (66) | 104 (35) | 111 (37) | 44 (15) | 65 (20) |
| BRAF | 1084 (37) | 322 (69) | 82 (28) | 62 (21) | 114 (38) | 185 (51) | 83 (28) | 96 (32) | 34 (11) | 106 (33) |
| TRK | 533 (18) | 246 (52) | 57 (20) | 31 (11) | 29 (10) | 44 (12) | 43 (14) | 39 (13) | 18 (6) | 26 (8) |
| MET | 784 (27) | 284 (60) | 75 (26) | 40 (14) | 64 (21) | 136 (37) | 58 (19) | 45 (15) | 27 (9) | 55 (17) |
| HER2 | 689 (23) | 266 (57) | 71 (25) | 31 (11) | 46 (15) | 114 (31) | 45 (15) | 48 (16) | 22 (7) | 46 (14) |
| NGS used, n | (base n=820) | (base n=291) | (base n=71) | (base n=49) | (base n=75) | (base n=137) | (base n=74) | (base n=58) | (base n=19) | (base n=46) |
| Yes | 628 (77) | 251 (86) | 58 (82) | 27 (55) | 51 (68) | 99 (72) | 41 (55) | 51 (88) | 13 (68) | 37 (80) |
| No | 192 (23) | 40 (14) | 13 (18) | 22 (45) | 24 (32) | 38 (28) | 33 (45) | 7 (12) | 6 (32) | 9 (20) |
| Results of | (base n=820) | (base n=291) | (base n=71) | (base n=49) | (base n=75) | (base n=137) | (base n=74) | (base n=58) | (base n=19) | (base n=46) |
| Positive | 39 (4.8) | 8 (2.7) | 19 (26.8) | 3 (6.1) | 1 (1.3) | 3 (2.2) | 0 (0) | 2 (3.4) | 1 (5.3) | 2 (4.3) |
| Negative | 781 (95.2) | 283 (97.3) | 52 (73.2) | 46 (93.9) | 74 (98.7) | 134 (97.8) | 74 (100) | 56 (96.6) | 18 (94.7) | 44 (95.7) |
|
| (base n=820) | (base n=291) | (base n=71) | (base n=49) | (base n=75) | (base n=137) | (base n=74) | (base n=58) | (base n=19) | (base n=46) |
| Yes | 689 (84) | 249 (86) | 53 (75) | 39 (80) | 70 (93) | 113 (82) | 56 (76) | 55 (95) | 14 (74) | 40 (87) |
| No | 119 (15) | 37 (13) | 15 (21) | 9 (18) | 5 (7) | 24 (18) | 18 (24) | 0 (0) | 5 (26) | 6 (13) |
| Unknown | 12 (1) | 5 (2) | 3 (4) | 1 (2) | 0 (0) | 0 (0) | 0 (0) | 3 (5) | 0 (0) | 0 (0) |
| Parameter | Overall aNSCLC cohort |
| USA (n=106) | Brazil (n=70) | UK (n=88) | Italy (n=56) | France (n=67) | Spain (n=85) | Germany (n=77) | Taiwan (n=27) |
|---|---|---|---|---|---|---|---|---|---|---|
| Chemotherapy, n (%) | 977 (33) | 185 (32) | 10 (9) | 14 (20) | 29 (33) | 32 (57) | 25 (37) | 40 (47) | 23 (30) | 12 (44) |
| Chemotherapy plus immunotherapy, n (%) | 548 (19) | 104 (18) | 13 (12) | 9 (13) | 29 (33) | 6 (11) | 13 (19) | 17 (20) | 15 (19) | 2 (7) |
| Immunotherapy, n (%) | 523 (18) | 52 (9) | 6 (6) | 8 (11) | 12 (14) | 3 (5) | 5 (7) | 5 (6) | 13 (17) | 0 (0) |
| Targeted therapy (+/- other), n (%) | 774 (26) | 92 (16) | 11 (10) | 21 (30) | 4 (5) | 3 (5) | 15 (22) | 6 (7) | 23 (30) | 9 (33) |
| Best supportive care only, n (%) | 51 (2) | 14 (2) | 1 (1) | 7 (10) | 2 (2) | 1 (2) | 1 (1) | 0 (0) | 1 (1) | 1 (4) |
| Other, n (%) | 70 (2) | 129 (22) | 65 (61) | 11 (16) | 12 (14) | 11 (20) | 8 (12) | 17 (20) | 2 (3) | 3 (11) |
- —Eli Lilly and Company 10.13039/100004312
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Radiomics and Machine Learning in Medical Imaging
Introduction
1
Non-small cell lung cancer (NSCLC) represents approximately 80−90% of all lung cancers (1, 2). Recently, treatment options for patients with advanced NSCLC (aNSCLC) have greatly expanded with the identification of targetable oncogenic driver alterations and the regulatory approval of several targeted therapies. One of these biomarkers is rearranged during transfection (RET) (3). Approximately 1−2% of all NSCLCs are positive for RET gene fusions (4, 5). Targeted treatments for RET fusion-positive aNSCLC include the selective RET kinase inhibitors selpercatinib and pralsetinib (6, 7).
Understanding real-world patient characteristics and treatment patterns, alongside more comprehensive information on biomarker testing, can provide important context for the rapidly evolving landscape of aNSCLC therapy and aid the generalizability of clinical trial data to routine clinical practice. The aim of this real-world multi-national study was to describe the clinical characteristics, biomarker testing, and treatment patterns of patients with RET fusion-positive aNSCLC.
Material and methods
2
This observational study was conducted from July to December 2020 in nine countries (Brazil, France, Germany, Italy, Japan, Spain, Taiwan, the UK, and the USA) following Adelphi DSP™ methodology, which involves large, multinational, cross-sectional surveys that collect real-world data from physicians and patients (8). Here, we report on patient-level data using electronic patient record forms (ePRFs) completed by physicians.
Recruitment, eligibility criteria, and data collection
2.1
Oncologists and pulmonologists (and respiratory surgeons in Japan) were identified using publicly available lists of clinicians in each country. Eligible specialists were responsible for managing patients with aNSCLC and saw at least three patients with a diagnosis of aNSCLC per month. A sample was then randomly selected from willing clinicians meeting the inclusion criteria.
Clinicians completed an online anonymized ePRF based on prior medical records for six consulting eligible patients with aNSCLC who were included in a pseudorandom sample (hereafter referred to as the overall aNSCLC cohort). An additional two patients were part of an oversample of patients with RET fusion-positive aNSCLC and no other co-alterations (hereafter referred to as the RET fusion-positive cohort). This latter cohort also included patients from the overall aNSCLC cohort whose disease was RET fusion-positive with no other co-alterations (Figure 1). Japanese patients were excluded from the RET fusion-positive cohort because RET fusion testing was not actively conducted in Japan at the time. Eligible patients were ≥18 years old, not participating in a clinical trial, and had a diagnosis of aNSCLC.
Schematic flow chart showing study design. aNSCLC, advanced non-small cell lung cancer; RET, rearranged during transfection.
Study variables
2.2
Physicians provided information on patient demographics, clinical characteristics, biomarker testing, and first-line treatment. In particular, the ePRFs captured individual patient data on RET testing, including whether RET testing was conducted, results of RET testing, and whether next-generation sequencing (NGS) was used.
Statistical analyses
2.3
Descriptive statistics are provided for demographics and disease characteristics, using median with interquartile range (IQR) for continuous variables, and the frequency and percentage within each category for categorical variables. Missing data were excluded from the analysis and no imputation was conducted.
Ethical considerations
2.4
Data collection was in line with European Pharmaceutical Marketing Research Association guidelines (9). Study materials and protocol were reviewed and exempted by the Western Institutional Review Board (study protocol number AG8757) and were in full accordance with relevant legislation at the time of data collection (10, 11).
Results
3
Demographic and clinical characteristic data were available for 2947 patients in the overall aNSCLC cohort and 576 patients in the RET fusion-positive cohort (Table 1). Characteristics were generally similar between these cohorts for most parameters, including median age (67 [IQR 60−72] years vs. 65 [IQR 57−70] years), presence of central nervous system metastases, and programmed cell death ligand 1 (PD-L1) expression, and with most patients in each cohort being male, having stage IV disease and Eastern Cooperative Oncology Group performance status (ECOG PS) 0−1 (Table 1). Median age for the overall aNSCLC cohort was similar across the nine countries (data not shown).
Although statistical comparisons were not made, there were notable numerical differences between the overall aNSCLC cohort and the RET fusion-positive cohort for some parameters, including higher proportions of White/Caucasian patients (68% vs. 84%), never smokers (23% vs. 36%), and histology of adenocarcinoma (70% vs. 88%), and lower proportion of squamous cell carcinoma (25% vs. 6%), in the RET fusion-positive cohort. All comparisons between cohorts came with a caveat that the RET fusion-positive cohort excluded Japanese patients and included a small number of patients from the overall cohort. In the RET fusion-positive cohort, there was wide variation in the proportion of never smokers across countries, ranging from 24% and 31% in France and the USA, respectively, to 70% in Taiwan (data not shown).
The testing rate for RET gene fusions at diagnosis of advanced disease was 31% (899 of 2947 patients) in the overall aNSCLC cohort, but varied widely across countries, from 8% in Taiwan to 67% in the USA (Table 2). Testing for epidermal growth factor receptor (EGFR) mutations was more consistent across countries, ranging from 73% in Brazil to 90% in Taiwan. In general, the USA had the highest rates of testing across all biomarkers (Table 2). For patients in the overall aNSCLC cohort with available results (n=820), the prevalence of RET gene fusions was 4.8%, but was as high as 26.8% in Brazil. Most patients (77%) had been tested using NGS, and 84% had test results available prior to initiation of treatment for advanced disease (Table 2).
The percentage of patients receiving chemotherapy (33% vs. 32%) or chemotherapy plus immunotherapy (19% vs. 18%) as first-line treatment was very similar between the overall aNSCLC cohort and the RET fusion-positive cohort (Table 3). In the RET fusion-positive cohort, across the eight countries evaluated, chemotherapy was prescribed for 9−57%, and chemotherapy plus immunotherapy for 7−33%, in the first-line setting (Table 3). Compared to the overall aNSCLC cohort, the percentage of patients treated with immunotherapy only (18% vs. 9%) or with targeted therapy (26% vs. 16%) was numerically lower in the RET fusion-positive cohort.
Discussion
4
This observational study provides real-world data from nine countries on the clinical characteristics, biomarker testing, and treatment patterns of patients with aNSCLC, focusing on data from patients with RET fusion-positive aNSCLC and no other co-alterations. Demographic and clinical characteristics, such as median age (65 years; IQR 57−70), advanced disease stage at diagnosis, predominantly adenocarcinoma histology, and a relatively high proportion of never smokers among the RET fusion-positive cohort were generally as expected for this patient population (3, 6). However, other studies have reported a preponderance of female patients (12), whereas in our RET fusion-positive cohort, 43% were female.
The RET testing rate of 31% across the nine countries in this study is much lower than those for EGFR and ALK (≈80%), the more established biomarkers for NSCLC. This has various clinical implications. First, RET is an emerging biomarker (13); selective RET inhibitors have been available only for the last 4 years but at the time of writing are still not widely available or reimbursed across all lines of therapy among the countries in this study, including Brazil and Taiwan (no access across any line of therapy) and France and Italy (no access for first-line therapy). As access to selective RET inhibitors expands, we expect testing rates to increase. Second, education and awareness for RET as an actionable biomarker needs to be pursued, as evidence clearly suggests that patients derive benefit when tested for RET and treated, if appropriate, with a selective RET inhibitor in the first-line setting (14). Third, as more actionable biomarkers emerge for NSCLC, broad testing with NGS should become the norm and this will help increase testing rates across the spectrum for all biomarkers. The 4.8% positivity rate for RET fusions in the overall aNSCLC cohort who were tested was somewhat higher than the expected rate of ≈1−2% for RET fusion-positive aNSCLC (4, 5), although the positivity rate was reduced to 2.7% after excluding data from Brazil, which had a positivity rate much higher than any other country (26.8%). The exact reason for this difference is not known.
The proportion of patients treated with first-line chemotherapy or chemotherapy plus immunotherapy was almost the same in both cohorts. However, the use of targeted treatment was numerically lower in the RET fusion-positive cohort than in the overall aNSCLC cohort, possibly because selective RET inhibitors were just becoming available at the time of the study. The use of immunotherapy was also numerically lower in the RET fusion-positive cohort, which appears to be consistent with the lower rate of PD-L1 expression ≥50% in this cohort.
Limitations of this study include its observational design, making it subject to potential biases inherent in non-randomized research, such as selection bias and confounding factors that could influence treatment choices and outcomes. For example, selection of consecutive patients may have resulted in over-representation of patients who consult more frequently. In addition, there may have been potential biases in selecting the RET fusion-positive cohort. This cohort included both a subgroup of patients with RET fusion-positive disease and no other co-alterations from the overall aNSCLC cohort and an oversample of those with RET fusion-positive disease and no other co-alterations, which may not accurately reflect the broader population of RET fusion-positive aNSCLC patients with varying molecular profiles. The retrospective study design using electronic patient records may have provided incomplete or inconsistent data across different sites, potentially affecting the accuracy of clinical information. The study was conducted across nine countries, which may have led to variability in treatment patterns and access to biomarker testing due to differences in healthcare systems, guidelines, and resources. Although 31% of patients in the overall aNSCLC cohort were tested for RET fusions, this may not represent the full patient population, and the availability of RET testing could be limited in some regions or settings, leading to underreporting of RET fusion-positive cases. It is also noteworthy that the study mainly focused on descriptive analysis of clinical characteristics and treatment patterns, rather than directly evaluating the effectiveness of different treatments in the RET fusion-positive cohort. This study was conducted almost 4 years ago and, while we believe the findings are still relevant, a repeat study should be performed to assess the impact of the advancements in diagnostic and treatment paradigms (e.g., availability of selective RET inhibitors) over these years.
In conclusion, this study provides insights into the clinical characteristics, biomarker testing, and treatment patterns of patients with RET fusion-positive aNSCLC and highlights the need for increased RET testing rates, preferably with NGS, with the option to treat with selective RET inhibitors in the event of RET fusion-positive disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer.org. Key statistics for lung cancer. Available online at: https://www.cancer.org/cancer/lung-cancer/about/key-statistics.html (Accessed November 3, 2023).
- 2Planchard D Popat S Kerr K Novello S Smit EF Faivre-Finn C. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2018) 29:iv 192–237. doi: 10.1093/annonc/mdy 275 30285222 · doi ↗ · pubmed ↗
- 3Choudhury NJ Drilon A. Decade in review: a new era for RET-rearranged lung cancers. Transl Lung Cancer Res. (2020) 9:2571–80. doi: 10.21037/tlcr-20-346 PMC 781536433489819 · doi ↗ · pubmed ↗
- 4Kohno T Nakaoku T Tsuta K Tsuchihara K Matsumoto S Yoh K. Beyond ALK-RET, ROS 1 and other oncogene fusions in lung cancer. Transl Lung Cancer Res. (2015) 4:156–64. doi: 10.3978/j.issn.2218-6751.2014.11.11 PMC 438421325870798 · doi ↗ · pubmed ↗
- 5Hess LM Han Y Zhu YE Bhandar NR Sireci A. Characteristics and outcomes of patients with RET-fusion positive non-small lung cancer in real-world practice in the United States. BMC Cancer. (2021) 21:28. doi: 10.1186/s 12885-020-07714-3 33402119 PMC 7786962 · doi ↗ · pubmed ↗
- 6Drilon A Oxnard GR Tan DSW Loong HHF Johnson M Gainor J. Efficacy of selpercatinib in RET fusion-positive non-small-cell lung cancer. N Engl J Med. (2020) 383:813–24. doi: 10.1056/NEJ Moa 2005653 PMC 750646732846060 · doi ↗ · pubmed ↗
- 7Griesinger F Curigliano G Thomas M Subbiah V Baik CS Dan TSW. Safety and efficacy of pralsetinib in RET fusion-positive non-small-cell lung cancer including as first-line therapy: update from the ARROW trial. Ann Oncol. (2022) 33:1168–78. doi: 10.1016/j.annonc.2022.08.002 35973665 · doi ↗ · pubmed ↗
- 8Anderson P Higgins V Courcy J Doslikova K Davis VA Karavali A. Real-world evidence generation from patients, their caregivers and physicians supporting clinical, regulatory and guideline decisions: an update on Disease Specific Programmes. Curr Med Res Opin. (2023) 39:1707–15. doi: 10.1080/03007995.2023.2279679 37933204 · doi ↗ · pubmed ↗