Fatal Neutropenia Sepsis Following Acute Methotrexate Toxicity
Nicholsan Jesiah, Yathukulan Siva, Sundaresan KT

TL;DR
A patient with chronic kidney disease and diabetes developed severe sepsis after a methotrexate dosing error, highlighting the need for careful medication management.
Contribution
This case report highlights the risk of acute methotrexate toxicity in elderly patients with CKD and emphasizes the importance of proper dosing education.
Findings
A dosing error led to acute methotrexate toxicity with neutropenic sepsis in a high-risk patient.
Treatment with folinic acid, GM-CSF, and antibiotics led to recovery within 12 days.
The case underscores the need for patient education to prevent life-threatening methotrexate complications.
Abstract
Methotrexate (MTX) is widely used to manage autoimmune diseases such as rheumatoid arthritis, psoriasis, and eczema due to its anti-inflammatory and immunosuppressive properties. We present the case of a 69-year-old male individual with stage 3b chronic kidney disease (CKD) and diabetes mellitus, who developed acute MTX toxicity following a dosing error. The patient, prescribed MTX 7.5 mg weekly for chronic lower leg eczema, mistakenly took 5 mg every eight hours for four days. He presented with erythematous rashes, oral mucosal ulcerations, and pancytopenia, later diagnosed as neutropenic sepsis. Management included discontinuation of MTX, intravenous folinic acid, granulocyte-macrophage colony-stimulating factor (GM-CSF), and broad-spectrum antibiotics. By day 7, his blood counts and symptoms improved, and he was discharged on day 12. This case underscores the importance of patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2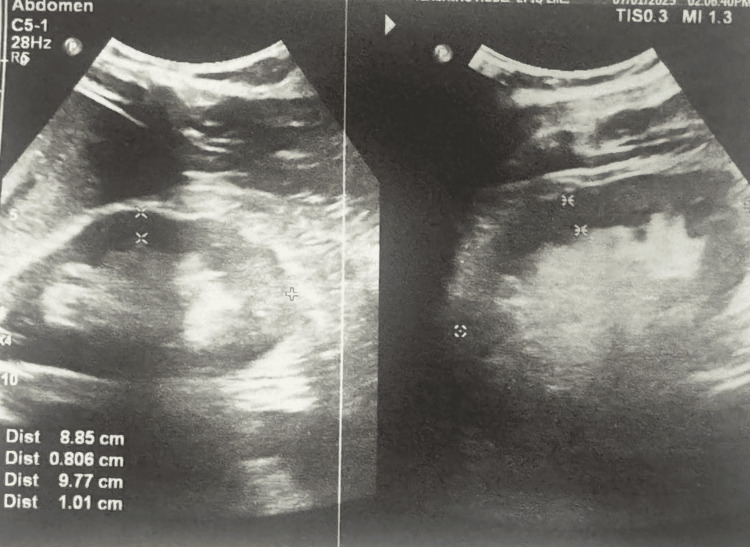 Figure 3
Figure 3| Test (unit) | Value | On discharge | Normal value |
| WBC (*103/uL) | 0.47 | 11.1 | 4-11 |
| Neutrophil (*103/uL) | 0.06 | 75.3 | 2-7 |
| Hemoglobin (g/dL) | 8.2 | 9.5 | 12-16 |
| Platelet (*103/uL) | 12 | 100 | 150-450 |
| AST (U/L) | 31 | 15-37 | |
| ALT (U/L) | 41 | 12-78 | |
| Serum Creatinine (micmol/L) | 200 | 62-115 | |
| CRP (mg/L) | 424 | 48 | 0-5 |
| ESR (mm/1st hour) | 125 | 55 | <20 |
| Serum sodium (mmol/L) | 142 | 136-145 | |
| Serum potassium (mmol/L) | 3.5 | 3.5-5.1 | |
| INR | 1.2 | <1.2 | |
| Blood culture & Urine culture | Negative | ||
| Ultrasound scan of abdomen & KUB | Features of chronic kidney disease only (poor corticomedullary demarcation) | ||
| Blood picture | Pancytopenia due to possible MTX toxicity | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeutropenia and Cancer Infections · Blood disorders and treatments · Chemotherapy-related skin toxicity
Introduction
Methotrexate (MTX) is a folic acid antagonist widely used in oncology and for managing chronic inflammatory and autoimmune diseases such as rheumatoid arthritis, psoriasis, and eczema [1]. It inhibits cellular proliferation, particularly affecting rapidly dividing cells, which accounts for its therapeutic benefits and potential toxicities. Common adverse effects include mucositis, cytopenia, and increased risk of infections, with toxicity risk heightened in specific populations [2].
MTX is primarily eliminated by the kidneys, with 80%-90% excreted unchanged in the urine. Patients with chronic kidney disease (CKD) are at greater risk of toxicity, even at low doses, due to impaired drug clearance. Clinical guidelines emphasize starting MTX at lower doses in such patients [3]. However, incorrect dosing or mismanagement, especially in elderly patients with multiple comorbidities, can lead to serious complications like pancytopenia and neutropenic sepsis.
Approximately 1.4% of patients on low-dose MTX develop pancytopenia [4], often triggered by errors in administration or inadequate monitoring [5]. Neutropenic sepsis, a life-threatening complication of pancytopenia, carries a high mortality rate if not promptly treated. Here, we present the case of a 69-year-old male individual with CKD and chronic eczema, who developed pancytopenia and neutropenic sepsis following an accidental MTX overdose, highlighting the critical importance of patient education and monitoring in MTX therapy.
Case presentation
A 69-year-old male individual with a history of non-insulin-dependent diabetes mellitus, stage 3b chronic kidney disease (CKD), and chronic eczema on both feet presented with generalized skin rashes and painful oral mucosal sores for one week. He had mistakenly taken methotrexate (MTX) 5 mg every eight hours for four days instead of the prescribed weekly dose of 7.5 mg, which was initiated for eczema management. The patient had been on oral hypoglycemic medications and regularly attended medical clinic follow-ups.
On admission, the patient was conscious and oriented, with stable vital signs (blood pressure 115/70 mmHg, pulse rate 92 beats per minute, respiratory rate 16 breaths per minute, temperature 99.5°F, and oxygen saturation of 99% on room air). Examination revealed pallor, large painful ulcerative lesions with bleeding in the oral cavity (Figure 1), and generalized erythematous scaly rashes with ulcerative lesions, most prominent on the lower limbs (Figure 2). Systemic examination findings were unremarkable.
Oral mucosal inflammation with bleeding and ulceration.
Erythematous lesions over the lower limb with scaling and ulceration.
Laboratory investigations showed Impaired renal function (eGFR {estimated glomerular filtration rate} 31 mL/min/1.73m²), pancytopenia (neutrophils 0.06×10³/µL, hemoglobin 8.2 g/dL, and platelets 12×10³/µL), elevated inflammatory markers (CRP {C-reactive protein} 424 mg/L, procalcitonin 56 ng/mL, and ESR {erythrocyte sedimentation rate} 125 mm/hr) but liver function tests were normal. Cultures from blood, urine, and wound swabs were sterile, and screening for HIV, hepatitis B, and hepatitis C was negative. Table 1 presents a summary of the relevant investigations.
Abdominal ultrasound findings were consistent with chronic kidney disease (Figure 3).
Bilateral kidneys show hyperechoic renal cortex with altered corticomedullary demarcation favors chronic kidney disease.
A diagnosis of severe neutropenia sepsis secondary to MTX-induced bone marrow suppression was made. On day 2, the patient was transferred to the high-dependency unit (HDU) and managed with intravenous piperacillin-tazobactam (4.5 g every eight hours), oral fluconazole (100 mg weekly), intravenous folinic acid (15 mg every six hours) and subcutaneous granulocyte-macrophage colony-stimulating factor (G-CSF) (300 MU/day). Supportive care was given including analgesics, antihistamines, intravenous fluids, multivitamins, oral antivirals, and topical applications (liquid paraffin, fusidic ointment, chlorhexidine mouthwash, and local lignocaine) while maintaining the reverse barrier method.
By day 7, the patient’s blood counts and symptoms improved significantly, with mucosal bleeding and skin lesions resolution. He was discharged on day 12 with a follow-up arranged with the dermatologist for ongoing eczema management.
Discussion
MTX, in low weekly doses, is a first-line treatment for chronic inflammatory diseases and certain cancers due to its anti-inflammatory and immunosuppressive properties [6]. Despite its benefits, MTX can cause severe adverse effects, including pancytopenia, mucositis, and cutaneous ulcerations, especially in high-risk populations. Risk factors for MTX toxicity include advanced age, CKD, hypoalbuminemia, infections, and polypharmacy [7,8]. Among these, CKD is a critical factor due to impaired drug clearance, which prolongs exposure and exacerbates toxicity.
In this case, the patient’s inadvertent daily dosing of MTX, combined with the absence of folic acid supplementation and underlying CKD, led to acute toxicity. MTX-induced pancytopenia and mucositis were prominent, with the latter contributing to decreased oral intake and prerenal acute kidney injury, further worsening renal function. These findings underscore the importance of identifying predisposing factors when prescribing MTX.
Management of MTX toxicity involves immediate drug discontinuation and initiation of supportive care [9,10]. In this patient, intravenous folinic acid and granulocyte-colony stimulating factor (G-CSF) effectively managed hematological toxicity. Broad-spectrum antibiotics addressed the risk of neutropenic sepsis, a life-threatening complication [10]. Although serum MTX levels were not measured, clinical signs strongly suggested toxicity, reinforcing the need for early intervention based on presentation rather than laboratory markers.
This case highlights several critical learning points, which are CKD and hypoalbuminemia increase the risk of MTX-induced bone marrow suppression by enhancing drug exposure [3], early signs of MTX toxicity such as mucositis, which has led to decreased oral intake causing prerenal acute kidney injury which worsened his renal function and proper patient counseling and regular follow-up are essential to prevent dosing errors, especially in elderly patients with multiple comorbidities.
Preventing MTX toxicity requires a multidisciplinary approach, including tailored dosing, education on medication use, and vigilant monitoring for early signs of complications. Comparisons with similar cases emphasize that adherence to clinical guidelines and proactive measures can minimize morbidity and mortality associated with MTX therapy.
Conclusions
Methotrexate (MTX) is a valuable medication for managing autoimmune and inflammatory conditions when used appropriately. However, this case highlights the potential for severe toxicity, even at low doses, when dosing errors or predisposing factors such as chronic kidney disease and advanced age are present. Acute MTX toxicity can lead to life-threatening complications like pancytopenia and neutropenic sepsis, underscoring the need for careful monitoring and individualized dosing.
This case emphasizes the critical importance of thorough patient counseling to ensure a proper understanding of the dosing schedule and potential risks. Regular follow-ups and adherence to clinical guidelines are essential to prevent avoidable errors and reduce morbidity and mortality associated with MTX therapy. By prioritizing patient education and monitoring, clinicians can minimize adverse outcomes and enhance the safe use of this effective but potentially hazardous drug.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intoxication due to high dose methotrexate in a patient with arthritis: a case report Turk J Rheumatol AltındağÖ Küçükoğlu B 5860262011
- 2Iatrogenically-related, fatal methotrexate intoxication: a series of four cases Forensic Sci Int Moisa A Fritz P Benz D Wehner HD 1541571562006 https://doi.org/10.1016/j.forsciint.2004.12.0311634383210.1016/j.forsciint.2004.12.031 · doi ↗ · pubmed ↗
- 3Acute methotrexate toxicity: a fatal condition in two cases of psoriasis Case Rep Dermatol Med Jariwala P Kumar V Kothari K Thakkar S Umrigar DD 94671620142014 https://doi.org/10.1155/2014/9467162527644210.1155/2014/946716 PMC 4172992 · doi ↗ · pubmed ↗
- 4How should we manage low-dose methotrexate-induced pancytopenia in patients with rheumatoid arthritis?Clin Rheumatol Cansu DÜ Teke HÜ Bodakçi E Korkmaz C 34193425372018 https://doi.org/10.1007/s 10067-018-4242-83005652310.1007/s 10067-018-4242-8 · doi ↗ · pubmed ↗
- 5Acute methotrexate toxicity Indian J Drugs Dermatol Madke B Singh AL 464912015 https://journals.lww.com/iodd/fulltext/2015/01010/acute_methotrexate_toxicity.19.aspx
- 6Systemic methotrexate therapy for psoriasis: past, present and future Clin Exp Dermatol Dogra S Mahajan R 573588382013 https://doi.org/10.1111/ced.120622383793210.1111/ced.12062 · doi ↗ · pubmed ↗
- 7Factors associated with toxicity, final dose, and efficacy of methotrexate in patients with rheumatoid arthritis Ann Rheum Dis Hoekstra M van Ede AE Haagsma CJ van de Laar MA Huizinga TW Kruijsen MW Laan RF 423426622003 https://ard.bmj.com/content/62/5/423.short 1269515310.1136/ard.62.5.423PMC 1754533 · doi ↗ · pubmed ↗
- 8Methotrexate-induced pancytopenia: serious and under-reported? Our experience of 25 cases in 5 years Rheumatology (Oxford) Lim AY Gaffney K Scott DG 10511055442005 https://doi.org/10.1093/rheumatology/keh 6851590190310.1093/rheumatology/keh 685 · doi ↗ · pubmed ↗