Formative Study to Inform a Physical Activity Intervention Targeted to Rural Men in the United States
Jacob Gallagher, Emine O. Bayman, Lisa A. Cadmus‐Bertram, Nathaniel D. M. Jenkins, Amy Pearlman, Kara M. Whitaker, Lucas J. Carr

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
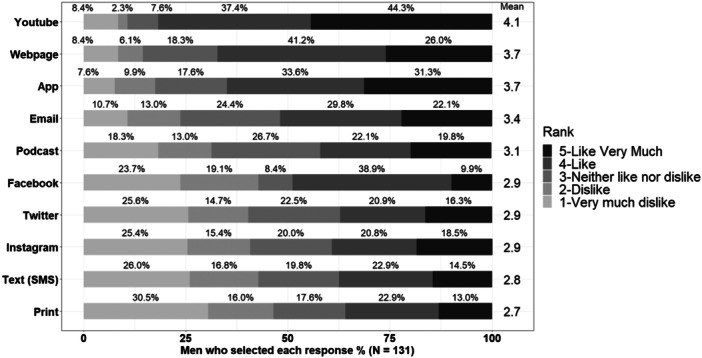 Figure 1
Figure 1| Behavior change technique | % of respondents selecting as a helpful feature |
|---|---|
| Demonstrations and instructions on how to exercise | 75.6% |
| Benefits of physical activity (including weight loss and management, disease prevention, healthy aging) | 68.9% |
| Encouragement to be physically active | 67.8% |
| Biofeedback on your physical activity (e.g., steps per day) | 67.8% |
| Techniques to help you stay active (e.g., goal setting, developing habits, tips/tricks) | 65.6% |
| Tools/techniques to manage time | 54.4% |
| Stress management techniques | 53.3% |
| Info on how to overcome barriers that are preventing you from being active | 51.1% |
| Personalized feedback on your physical activity goals | 42.2% |
| Info on how active I should be | 41.1% |
| Info on how to set physical activity goals | 35.6% |
| Costs of different physical activities | 33.3% |
| Opportunities to connect with others through an online community | 32.2% |
| Risks of being inactive | 30.0% |
| Reminders throughout the day to be physically active | 30.0% |
| How other men view exercise | 22.2% |
| Comparison to other men's physical activity (e.g., leaderboards. competitions) | 20.0% |
| Opportunities to speak with a health coach | 20.0% |
- —This research was supported by the Graduate and Professional Student Government at the University of Iowa.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Obesity, Physical Activity, Diet · Obesity and Health Practices
Introduction
1
American rural men have a higher risk of inactivity‐related disease and premature mortality compared to rural women and urban men [1, 2, 3]. However, only 27.6% of rural men meet the physical activity guidelines [4]. Our previous study found that 80% of rural American men were interested in a physical activity intervention [5], yet rural men make up a small proportion (< 15%) of people in physical activity interventions [6].
Preliminary evidence from Australia suggest that rural men may be interested in tailored interventions [7]. While rare, physical activity interventions specifically tailored to men have been effective at recruiting and retaining men; however, these past studies have been targeted primarily to urban men outside of the United States [8, 9].
The Obesity‐Related Behavior Intervention Trials (ORBIT) model [10] was developed to develop behavioral interventions efficiently, effectively, and targeted to the needs of specific populations, and uses similar terminology to testing new pharmaceutics. During Phase Ia (define), the basic elements of the intervention are defined, including the behavior change theory used, appropriate population, and barriers to be addressed. In Phase Ib (refine) of the ORBIT model, the mode of delivery and intervention features need to be identified.
Our prior research met the benchmark in Phase Ia [5], but additional evidence is needed to meet the benchmarks in Phase Ib of the ORBIT model. The aim of this study is to reach those milestones by identifying: (1) potential psychosocial constructs to targets, (2) behavior change techniques, (3) channels of delivery (how information is delivered and by whom), and (4) a specific focus of the program.
Methods
2
Participants
2.1
Rural men (447 total invites), who completed our initial needs assessment [5], were recontacted via Amazon's Mechanical Turk. To be included, participants needed to self‐identify as male, be over 18 years old, and live in the United States in a town of less than 2500 people or outside of a town. All procedures were approved by the Institutional Review Board at the University of Iowa and were performed in accordance with the Declaration of Helsinki. All participants provided informed consent before participating in the study.
Measures
2.2
Psychosocial Constructs
2.2.1
Participants completed an online survey (see Rhodes, 2021 [11]) that measured psychosocial constructs related to physical activity behavior (attitudes, capability, opportunity, behavior regulation, habit, and identity) that align with the multi‐process action control theory, a meta‐theory that draws from multiple existing psychosocial theories related to physical activity [12, 13].
Behavior Change Techniques
2.2.2
Participants were asked to select behavior change techniques previously identified in Michie's behavior change taxonomy [14] that they would find helpful in a physical activity program (e.g., demonstrations, encouragement).
Channels of Delivery
2.2.3
Participants were asked to rank their preference for various channels of receiving information (e.g., website, app.) and the mode of presentation (e.g., presenter characteristics).
Focus of the Program
2.2.4
Lastly, participants selected preferred program focuses including modes of exercise (e.g., strength, cardio) and targeted health benefits (e.g., physical fitness, mental health).
Data Analysis
2.3
Data were summarized by descriptive statistics, including frequencies, means, standard deviation, and percentages using R.
Results
3
Men completing the survey (n = 131) were mostly White (89.5%), non‐Hispanic (93.9%), college educated (84.2%), married (57.0%), and full‐time workers (62.6%). Ages ranged from 18 to 79 years (median: 39 years old). Using IP address, participants were from the Midwest (n = 43), Northeast (n = 21), South (n = 38), and West (n = 21) census bureau regions (8 without an identifiable region) in the United States.
Participants reported high levels of instrumental attitudes (Mean ± standard deviation: 16.1 ± 2.0 out of 18), perceived capability (15.1 ± 3.1 out of 18), perceived opportunity (14.9 ± 3.4 out of 18), and affective attitude (13.2 ± 3.6 out of 18), but reported lower levels of behavioral regulation (17.4 ± 8.8 scored out of 36), habit formation (13.5 ± 7.0 out of 24), and physical activity identity (16.1 ± 5.8 out of 24). Rural men reported exercise demonstrations as the top choice (selected by 74.0%) of behavior change techniques (Table 1).
More than half of all participants (55.7%) reported a preference for a male presenter in exercise demonstration videos while a third (32.8%) had no preference. A fitness professional (e.g., exercise physiologist) was the most preferred person to demonstrate an exercise (Mean ± SD: 4.3 ± 0.9 on a scale of 1‐Dislike a great deal to 5‐like a great deal), followed by a peer (3.6 ± 2.0), medical professional (3.2 ± 1.2), spokesperson (e.g., celebrity; 2.9 ± 1.3), and local leaders (2.7 ± 1.4).
YouTube videos (Mean ± SD: 4.1 ± 1.2 on a scale of 1‐dislike very much to 5‐like very much) was the most preferred method of receiving educational information (Figure 1). When asked who should deliver the information, rural men's top choices were fitness professionals (Mean ± SD: 4.2 ± 0.9 on a scale of 1‐Dislike a great deal to 5‐like a great deal) and medical professionals (3.8 ± 1.0). For delivery of educational materials, 51.9% preferred a male, while 38.0% had no preference.
The percent of men selecting like or dislike for modes of delivery with the mean response represented on the right‐side column.
Rural men reported wanting information on how physical activity can improve “physical fitness” (selected by 84.0%), “mental health” (69.5%), and “sleep” (58.0%). Most men (68.7%) reported they wanted a program that focuses on self‐improvement compared to 46.6% who selected a leisurely program and 38.9% who selected a competitive program. The modalities of exercise men most preferred were strength (80.9%), cardio (69.5%), and balance (67.2%).
Discussion
4
Our findings support the use of YouTube videos of a male fitness professional demonstrating rural men's preferred exercises, strength, aerobic (cardio), and balance with an emphasis on self‐improvement. Previous research suggests such videos should use simple, straightforward language, and humor when appropriate [9].
American rural men may view purposeful physical activity (e.g., manual labor) as more socially acceptable and are motivated to slow aging and maintain strength [15]. In line with this, we found a slight preference for strength training and a focus on self‐improvement instead of leisurely focus. In tailored men's health research, it may be important to tailor to masculine norms to draw men in to the program, but once in the program, these norms might be slightly modifiable [16]. For example, advertising a strength program may get men through the door, but once they “buy in,” they may be convinced to do more aerobic activity or other health behaviors (e.g., eat healthier).
An intervention that promotes behavioral regulation, such as providing a tracking device, may be best suited for rural men, as attitude and capability were both reported near maximum values. In a previous study using a weight loss app, rural men found behavior regulation an acceptable and helpful feature [17]. However, the efficacy of app was limited [18], which suggest that not only does the psychosocial elements need to be targeted but other features (channel of delivery, focus of program) may need to be tailored to promote efficacy.
Our sample was more educated and had more White participants than the national average for rural communities [19]. To improve representation of education status of rural men, alternative recruitment methods are warranted, such as ads (radio, newspapers) and through existing networks (e.g., extension outreach, Farm Bureau). This may be particularly important to how information is presented and received by those with less education. A strength of this study is the use of a nationwide survey, allowing for more generalizability in the United States than a geographic specific study. Similarly, there was a wide age range represented.
Conclusion
5
These findings provide a basis for a Phase IIa proof‐of‐concept study to test the initial feasibility, acceptability, efficacy of an intervention that tailors to rural men by focusing on demonstrations of physical activity and behavioral regulation.
Author Contributions
Jacob Gallagher: conceptualization, investigation, funding acquisition, writing – original draft, methodology, validation, visualization, writing – review and editing, software, formal analysis, project administration, data curation, supervision, resources. Emine O. Bayman: writing – review and editing, formal analysis, conceptualization. Lisa A. Cadmus‐Bertram: writing – review and editing, methodology, conceptualization. Nathaniel D. M. Jenkins: writing – review and editing, formal analysis, conceptualization. Amy Pearlman: conceptualization, writing – review and editing. Kara M. Whitaker: conceptualization, writing – review and editing. Lucas J. Carr: conceptualization, funding acquisition, writing – review and editing, supervision, project administration.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Jacob Gallagher affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. A. Harrington , R. M. Califf , A. Balamurugan , et al., “Call to Action: Rural Health: A Presidential Advisory From The American Heart Association and American Stroke Association,” Circulation 141, no. 10 (2020): e 615–e 644.32078375 10.1161/CIR.0000000000000753 · doi ↗ · pubmed ↗
- 2T. H. Callaghan , S. D. Towne , J. Bolin , and A. O. Ferdinand , “Diabetes Mortality in Rural America: 1999‐2015,” Southwest Rural Health Research Centre 4 (2017): 1, https://www.ruralhealthresearch.org/publications/1140.
- 3G. K. Singh , S. D. Williams , M. Siahpush , and A. Mulhollen . “Socioeconomic, Rural‐Urban, and Racial Inequalities in US Cancer Mortality: Part I—All Cancers and Lung Cancer and Part II—Colorectal, Prostate, Breast, and Cervical Cancers,” Journal of Cancer Epidemiology 2011 (2011): e 107497.10.1155/2011/107497 PMC 330701222496688 · doi ↗ · pubmed ↗
- 4NHIS ‐ Tables of Summary Health Statistics [Internet]. 2021 [cited 2022 June 8], https://www.cdc.gov/nchs/nhis/shs/tables.htm.
- 5J. Gallagher , E. O. Bayman , L. A. Cadmus‐Bertram , et al., “Physical Activity Among Rural Men: Barriers and Preferences,” Preventing Chronic Disease 20 (2023): E 88.37797290 10.5888/pcd 20.230046 PMC 10557978 · doi ↗ · pubmed ↗
- 6E. S. George , G. S. Kolt , M. J. Duncan , et al., “A Review of the Effectiveness of Physical Activity Interventions for Adult Males,” Sports Medicine 42, no. 4 (2012): 281–300.22350570 10.2165/11597220-000000000-00000 · doi ↗ · pubmed ↗
- 7M. D. Mc Donald , K. Hunt , J. Moullin , D. Kerr , N. Ntoumanis , and E. Quested , “A Different Ball Game’: Adaptation of a Men's Health Program for Implementation in Rural Australia,” BMC Public Health 23, no. 1 (2023): 1387.37468854 10.1186/s 12889-023-16247-w PMC 10355060 · doi ↗ · pubmed ↗
- 8J. L. Bottorff , C. L. Seaton , S. T. Johnson , et al., “An Updated Review of Interventions That Include Promotion of Physical Activity for Adult Men,” Sports Medicine 45, no. 6 (2015): 775–800.25430599 10.1007/s 40279-014-0286-3PMC 4440891 · doi ↗ · pubmed ↗