Mesenteric panniculitis: A case report
Rabti Souphia, Ben Marzouk Sawssen, Farjaoui Wael, Mohamed Hedi Mannai, Khalifa Mohamed Bechir

TL;DR
This paper reports a case of mesenteric panniculitis, a rare benign condition involving inflammation of abdominal fat, and highlights its diagnosis and treatment.
Contribution
The paper contributes a new case report and reinforces the importance of CT imaging and conservative management in mesenteric panniculitis.
Findings
Mesenteric panniculitis was diagnosed in a 49-year-old woman through imaging and biopsy.
Conservative treatment successfully managed the patient's symptoms.
CT scans are essential for identifying the condition, often incidentally.
Abstract
Mesenteric panniculitis is a rare, benign condition characterized by chronic inflammation and fibrosis of mesenteric adipose tissue (Hussein and Abdelwahed, 2015; Gögebakan et al., 2018 [1, 2]). While its etiology remains unclear in many cases, it has been associated with various conditions including abdominal surgery, trauma, and inflammatory diseases (Buragina et al., 2019 [3]). Understanding its presentation and management is crucial for proper patient care. We present a case of mesenteric panniculitis in a 49-year-old woman who presented with significant weight loss. The diagnosis was confirmed through imaging studies and tissue biopsy, with successful symptomatic management through conservative treatment. The condition typically presents with nonspecific symptoms including abdominal pain, nausea, and weight loss, though it may be discovered incidentally. Diagnosis relies on a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
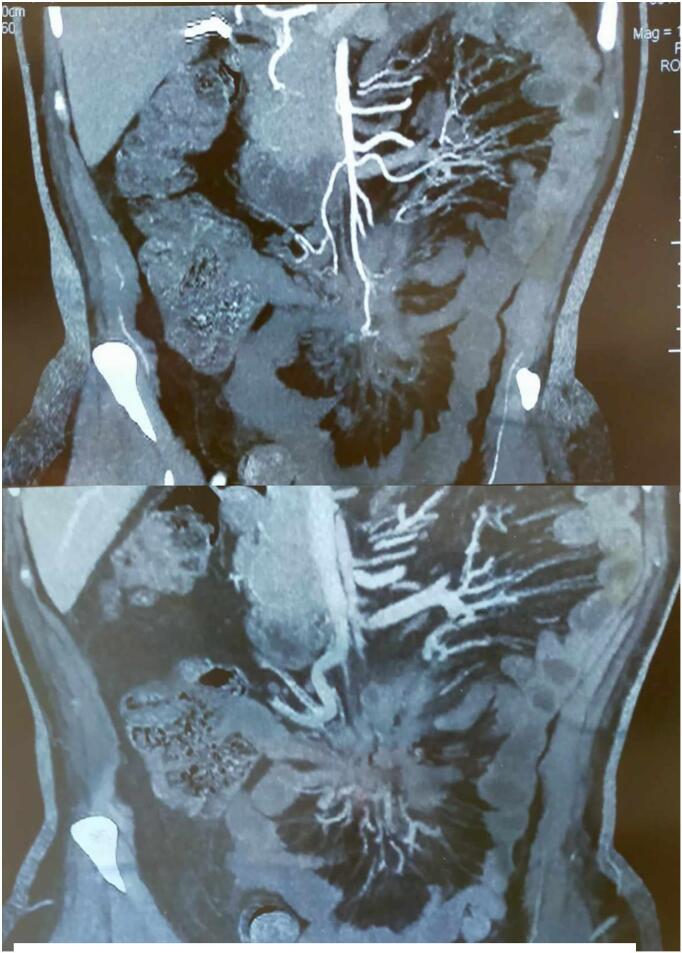 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Abdominal vascular conditions and treatments · Pancreatitis Pathology and Treatment
Introduction
1
Mesenteric panniculitis represents a rare inflammatory condition affecting the adipose tissue of the mesentery [1,2]. The condition progresses through three distinct stages: lipodystrophy, panniculitis, and finally retractile mesenteritis [4]. Its prevalence remains uncertain, though studies suggest it affects approximately 0.6–2.5 % of patients undergoing abdominal CT scans [5].
The etiology remains poorly understood, with various proposed mechanisms including autoimmune responses, previous abdominal surgery, trauma, and underlying malignancy [3,6]. Recent studies have highlighted associations with IgG4-related disease and various inflammatory conditions [7,8]. Understanding this condition is crucial due to its potential impact on patient quality of life and its association with other underlying pathologies.
This work has been reported in line with the SCARE criteria [9].
Case report
2
Patient information
2.1
A 49-year-old woman presented with a 15-kg weight loss over six months. Her initial BMI was 28.4 kg/m^2^, decreasing to 22.7 kg/m^2^ at presentation. The patient has a medical history of controlled arterial hypertension, managed with a daily dose of amlodipine 5 mg. Surgical interventions include a McBurney appendectomy performed at the age of eight, an epigastric hernia repair with mesh placement in 2016, and an abdominoplasty in 2020 to address post-pregnancy abdominal wall laxity. Additionally, she underwent a laparoscopic cholecystectomy in 2022 due to symptomatic cholelithiasis.
On physical examination, the patient had stable vital signs, with a blood pressure of 125/75 mmHg, a heart rate of 76 beats per minute, and a temperature of 36.8 °C. Abdominal examination revealed a soft abdomen with mild tenderness in the periumbilical region, without palpable masses, and well-healed surgical scars. Laboratory investigations showed a white blood cell count of 7.2 × 10^9^/L, hemoglobin at 13.4 g/dL, and platelets at 245 × 10^9^/L. The comprehensive metabolic panel, thyroid function tests, serum calcium, and phosphate levels were within normal limits, while inflammatory markers indicated an ESR of 22 mm/h and a CRP of 8 mg/L. Imaging studies, including an abdominal CT with contrast, revealed mesenteric panniculitis characterized by a “misty mesentery” appearance and mesenteric adenopathy (Figs. 1, 2). A colonoscopy was performed to rule out underlying inflammatory bowel disease or malignancy, with normal findings.Figs. 1, 2Scans of mesenteric panniculitis.Figs. 1, 2
The patient was initially treated with analgesics (acetaminophen 1 g TID) and low-dose prednisone (20 mg daily with gradual taper), alongside regular monitoring of symptoms and inflammatory markers. At the three-month follow-up, there was a resolution of abdominal pain, stabilization of weight, and improvement in inflammatory markers. A six-month follow-up CT showed stable mesenteric changes, and the patient continues to undergo annual monitoring to assess for disease progression or the development of associated conditions.
Discussion
3
Mesenteric panniculitis presents a diagnostic challenge due to its nonspecific symptoms and varying clinical course. First described by Jura in 1924, the condition predominantly affects males with a ratio of 2–3:1 [10]. Understanding of its pathogenesis has evolved, with recent literature suggesting a complex interplay between inflammatory mediators and immune response [11].
The progression of the disease occurs in three stages: lipodystrophy, characterized by fat cell necrosis; panniculitis, marked by an inflammatory infiltrate; and retractile mesenteritis, distinguished by fibrosis and tissue retraction. Imaging plays a crucial role in diagnosis, with CT being the preferred modality, revealing characteristic findings such as a “misty mesentery” appearance, the fat ring sign, pseudocapsule formation, and lymph node involvement. While MRI can provide complementary information, particularly in cases where CT findings are inconclusive, it is considered an adjunct diagnostic tool rather than a second-line option [12]. Management strategies depend on symptom severity and the underlying cause, with conservative treatment using anti-inflammatory medications often providing adequate symptom control. However, surgical intervention is reserved for complications such as bowel obstruction or perforation [13].
Conclusion
4
Mesenteric panniculitis requires a high index of suspicion for diagnosis. While often benign, thorough evaluation is essential to exclude underlying malignancy. Regular monitoring and appropriate symptomatic management typically lead to favorable outcomes. This case highlights the importance of systematic evaluation and long-term follow-up in patients with mesenteric panniculitis.
Author contribution
Rabti Souphia and Ben Marzouk Sawssen contributed to manuscript writing and editing, and data collection; Wael Farjaoui contributed to data analysis; Mohamed Hedi Mannai and Med Bachir Khalifa contributed to conceptualization and supervision; All authors have read and approved the final manuscript.
Patient consent
Written informed consent was obtained from the patient for the publication of this case report and its accompanying images. A copy of the written consent is available for the Editor-in-Chief of this journal to review upon request.
Ethical approval
Ethical approval is not applicable/waived at our institution. Due to the specific nature of case reports, which involve detailed descriptions of observations and interventions that have already been conducted on patients, as opposed to prospective studies involving planned interventions, our institution does not require formal ethical approval for such cases. We recognize the importance of ethics in medical research and are fully committed to upholding ethical standards in our medical and research practices.
Guarantor
Rabti Souphia.
Guarantor
Rabti Souphia.
Research registration number
N/A.
Funding
This research did not receive funding from any specific grant provided by public, commercial, or not-for-profit organizations.
Conflict of interest statement
No conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hussein M.R.A.Abdelwahed S.R.Mesenteric panniculitis: an update Expert Rev. Gastroenterol. Hepatol.91201567782522029910.1586/17474124.2014.939632 · doi ↗ · pubmed ↗
- 2GögebakanÖ.Osterhoff M.Albrecht T.Mesenteric panniculitis (MP): a frequent coincidental CT finding of debatable clinical significance Fortschr. Röntgenstr.1901120181044105210.1055/a-0633-355830189433 · doi ↗ · pubmed ↗
- 3Buragina G.Magenta Biasina A.Carrafiello G.Clinical and radiological features of mesenteric panniculitis: a critical overview Acta Biomed 90420194114223191016410.23750/abm.v 90i 4.7696 PMC 7233778 · doi ↗ · pubmed ↗
- 4Mirabile A.Moschetta M.Lucarelli N.Scardapane A.Ianora A.A.S.A diagnostic dilemma: pedunculated mesenteric lipodystrophy Int. J. Surg. Case Rep.7220201831873254482610.1016/j.ijscr.2020.05.083PMC 7298552 · doi ↗ · pubmed ↗
- 5Van Putte-Katier N.van Bommel E.F.Elgersma O.E.Hendriksz T.R.Mesenteric panniculitis: prevalence, clinicoradiological presentation and 5-year follow-up Br. J. Radiol.87104420142014045110.1259/bjr.20140451 PMC 424319925271412 · doi ↗ · pubmed ↗
- 6Arvanitakis M.Dumonceau J.M.Albert M.Mesenteric panniculitis: a systematic review of 808 cases Intern. Med. J.518202112011210
- 7Sharma P.Yadav S.Needham C.M.Feuerstadt P.Sclerosing mesenteritis: a systematic review of 192 cases Clin. J. Gastroenterol.10220171031112819778110.1007/s 12328-017-0716-5 · doi ↗ · pubmed ↗
- 8You J.S.Heo J.W.Choi J.I.The clinical and pathological features of mesenteric panniculitis and their relationship with malignancy: a single-center study of 48 cases Medicine (Baltimore)99262020 e 20657