Insights into leprosy epidemiology from an isolated population located in the Brazilian Amazon
Ciane Cristina de Oliveira Mackert, Fernando Panissa Lázaro, Márcia Olandowski, Helena Regina Salomé D’Espindula, Andressa Mayra dos Santos, Priscila Verchai Uaska Sartori, Rafael Saraiva de Andrade Rodrigues, Geison Cambri, Marília Brasil Xavier, Erwin Schurr, Alexandre Alcaïs

TL;DR
This study explores leprosy patterns in an isolated Brazilian Amazon village, revealing higher prevalence and earlier diagnosis among locals compared to newcomers.
Contribution
The study provides novel insights into leprosy epidemiology using data from a unique, hyper-endemic, isolated population.
Findings
Cumulative leprosy prevalence was 22.9% among villagers born in the village versus 5.9% among those not born there.
The median age at diagnosis was 15 years for villagers born in the village versus 28 years for others.
No gender difference in leprosy case distribution was observed in the study population.
Abstract
Leprosy, a chronic infectious disease caused mainly by Mycobacterium leprae (M. leprae), is still an important public health problem in countries such as Brazil and India. Here, we estimate key epidemiological parameters in the Prata Village, a unique, hyper-endemic, former leprosy colony isolated in the Brazilian Amazon. This is a population-based study in which the entire Prata Village population has been enrolled. Clinical, socioeconomic, and demographic data were obtained and validated by cross-checking using three independent information sources. Validated data was used for descriptive epidemiological analysis. From a total of 2,005 inhabitants by the time of the enrollment, 1,084 (56.2%) were born in the Village and, therefore, likely under lifelong exposure to leprosy cases. We observed differences between the sub-populations born and not born in the village in the cumulative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
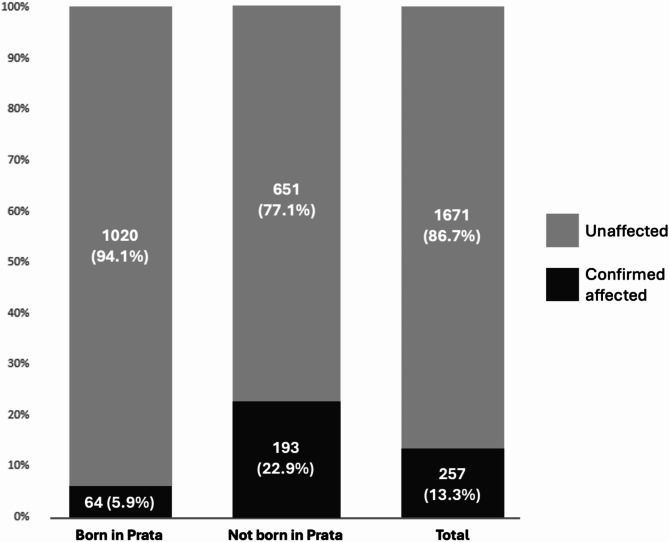 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeprosy Research and Treatment · Mycobacterium research and diagnosis · Infectious Diseases and Tuberculosis
Introduction
Leprosy is a chronic infectious disease caused mainly by Mycobacterium leprae (M. leprae), an obligate and highly specialized intracellular bacteria that primarily infects skin macrophages and Schwann cells in the peripheral nervous system^1^. According to the Ridley-Jopling classification system, leprosy manifests clinically in a spectrum consisting of two polar—tuberculoid and lepromatous—and three intermediate borderline forms^2^. The latest data from the World Health Organization (WHO) indicates 182,815 newly reported cases of leprosy in 2023^3^, mainly concentrated in India and Brazil. The disease is effectively treated through multidrug therapy (MDT) following a WHO protocol considering the number of lesions and the bacillary load: paucibacillary patients (PB) present up to five skin lesions, and the absence of bacilli in bacilloscopy or histopathology, whereas multibacillary (MB) patients have a positive bacilloscopy and/or six or more lesions^4^.
The village of Santo Antônio do Prata (the Prata Village) was established in 1898 by Franciscan monks in the Amazon forest of the Northern Brazilian state of Pará. In 1923, the location was designated a compulsory isolation site for individuals diagnosed with leprosy from Brazil’s Northern and Northeastern states. Compulsory isolation was lifted in 1962^5^; however, due to the strong social stigma associated with the disease, the emigration of affected individuals and the immigration of non-affected families to the village has been limited over the decades. Consequently, the Prata Village remained socially and geographically isolated until recent years. The population of the village concentrates in an area of around 10 km^2^, and all residents share the same limited social infrastructure, such as a single church, two elementary schools, one social club, and a large central square serving as a communal gathering space for leisure activities such as soccer games and outdoor celebrations. Despite extensive efforts to reduce its incidence, leprosy remains highly prevalent and uniformly distributed throughout the community^6^. In 2010, a complex segregation analysis provided evidence of a significant major gene effect controlling susceptibility to leprosy within the Prata population, a finding compatible with the hypothesis that, given the history of the village, genetic risk factors for leprosy are enriched within this population^6^.
We propose that Prata village can serve as a compelling epidemiological model for leprosy, given that (i) the village is confined in a small, geographically isolated area, (ii) it is a leprosy hyperendemic cluster, (iii) the disease is distributed homogenously across the entire village, (iv) the population shares few social interaction spaces, consequently, (v) exposure to the disease is likely homogeneous and widespread among the community. Finally, (vi) the Prata population is enriched in genetic risk factors controlling leprosy susceptibility. Here, we present a population-based descriptive epidemiological study involving the entire population of the Prata Village.
Methods
Enrollment of the entire population of the Prata Village was performed between 2006 and 2007; a detailed description of the enrollment strategy can be found in Lázaro F.P. et al. 2010^6^. In brief, every household in the village was visited by a research team member, and all adult members of resident families were interviewed; the parents or legal guardians provided information about individuals younger than 18 years old. Socio-economic data has been collected through a questionnaire. All individuals self-reported their present and previous leprosy status as affected or non-affected. All self-reported leprosy cases, active and historical, have been checked using three independent sources available at the village’s health unit: (i) the original medical records, (ii) copies of the compulsory notification forms, and (iii) a logbook containing registries of all cases for treatment follow-up. Self-reported cases confirmed at all three sources were validated as leprosy cases; clinical information was obtained from the medical records upon confirmation. The research was conducted in accordance with relevant guidelines and regulations, as outlined in the Helsinki Declaration (2008 revision). All subjects enrolled in the study agreed to participate and signed a written informed consent. The research project was approved by the Research Ethics Committee of the Pontifícia Universidade Católica do Paraná (51/07/CEP-PUCPR) and the Brazilian National Board for Ethics in Research (222/2006; 25000.001992/2006-17). Of note, only two individuals declined to participate and were not included in the study.
Given that this population-based study involved the recruitment of the entire Prata village, no inferential statistics were applied. Descriptive statistics was used to describe and compare two sub-populations: individuals born versus individuals not born in the village, the rationale being that, whereas no information about life conditions pre-Prata was available for the sub-population of individuals not born in the village, individuals born in the village have been living their entire lives in a homogenous environment, hyperendemic for leprosy. Median and mean age at diagnosis were estimated and depicted in a cumulative age plot.
Results
A complete characterization of the population of the Prata village is summarized in Table 1. Of the 2,005 individuals enrolled, 1,672 self-reported as non-affected by leprosy, 319 self-reported as affected, and 14 did not disclose their leprosy status. Data verification confirmed 257 out of the 319 self-reported leprosy cases. For subsequent analyses, 76 individuals with unknown leprosy status (comprised of the 14 individuals who did not disclose their status and an additional 62 individuals with unavailable medical reports) were excluded. Consequently, the accumulated prevalence rate of leprosy for the period (including active and historical cases) was calculated as 12.8% (257 cases out of 2,005 individuals), evenly distributed across males and females. When stratifying the affected population by clinical form, 104 (40.5%) cases were lepromatous, 53 (20.6%) were tuberculoid, 53 (20.6%) were borderline, and 47 (18.3%) were indeterminate (Table 2). Therefore, the highest proportion of the Prata patients had a higher bacillary load.
About half of the Prata village population—1,084 individuals (56.2%)—were born there. Among these, 64 were confirmed leprosy cases, resulting in a cumulative prevalence of 5.9%. Among the individuals not born in the village, the cumulative leprosy prevalence was 22.9% (193 confirmed cases/844 individuals) (Fig. 1). The median age at diagnosis among the individuals born in the village was 15 years old (mean = 18.1, ranging from 5 to 75 years old, standard deviation of ± 12.9). In contrast, the median age at diagnosis was 28 years old among the individuals not born in the village (mean = 30.1, ranging from 2 to 74 years old and standard deviation of ± 15.2) (Table 2, supplementary Fig. 1). A comparative description of the subpopulations born and not born in the village is presented in the supplementary Table 1.
Table 1. Epidemiological characterization of the confirmed affected and unaffected subjects in Prata Village.Confirmed affected subjectsUnaffected subjectsTotal subjectsn%n%n%Total sample size (n)25716721929Age (years) n^a^25716681925 Mean47.820.324.0 Median491619 Minimum1000 Maximum898289 Standard deviation19.915.919.0Sex Male15359.5%81949.0%97250.4% Female10440.5%85351.0%95749.6%Ethnicity White2710.5%17110.2%19810.3% Black5019.5%19511.7%24512.7% Mixed race18070.0%130177.8%148176.8% Others00.0%40.2%40.2% Unknown00.0%10.1%10.1%Marital status Single8432.7%114768.6%123163.8% Stable Union/Married13954.1%47428.3%61331.8% Divorced20.8%90.5%110.6% Widowed3112.0%382.3%693.5% Others10.4%30.2%40.2% Unknown00.0%10.1%10.1%Birthplace Prata6424.9%102061.0%108456.2% Others19375.1%65138.9%84443.7% Unknown00.0%10.1%10.1%Education Illiterate6625.7%865.1%1527.9% Incomplete Elementary School9235.8%59035.3%68235.3% Complete Elementary School197.4%714.2%904.7% Incomplete Middle School3915.2%31218.7%35118.2% Complete Middle School72.7%714.2%784.0% Incomplete High School135.0%1106.6%1236.4% Complete High School114.3%1116.6%1226.3% More than High School31.2%27616.6%27914.5% Unknown72.7%452.7%522.7%Alcohol drinking habit Yes8934.6%33720.2%42622.1% No16865.4%133579.8%150377.9%Smoking0 Yes9235.8%29217.5%38419.9% No16564.2%138082.5%154580.1%Recreative drug using habit Yes51.9%251.5%301.5% No24996.9%163597.8%188497.7% Unknown31.2%120.7%150.8%n, number; n ^a^, number of individuals with available information.
Table 2. Clinical characterization of the Prata village—confirmed affected subjects.Confirmed affected subjectsTotal sample size (n)257Age at diagnosis (years) n^a^257 Mean27.2 Median25 Minimum2 Maximum75 Standard deviation15.5Age at diagnosis—born in Prata (years) n^a^64 Mean18.1 Median15 Minimum5 Maximum75 Standard deviation12.9Age at diagnosis—not born in Prata (years) n^a^193 Mean30.1 Median28 Minimum2 Maximum74 Standard deviation15.2Clinical classification Tuberculoid53 (20.6%) Borderline53 (20.6%) Lepromatous104 (40.5%) Indeterminate47 (18.3%)n, Number; n ^a^, number of individuals with the information available.
Fig. 1. The proportion of affected individuals in the total population and the sub-populations of individuals born and not born at the Prata village. Numbers inside the bars: total number of individuals and proportion in %.
Discussion
Here, we present a descriptive, population-based study of a well-controlled, hyperendemic, isolated leprosy-affected community that might bring insights into the epidemiology of this elusive disease. Our most striking findings are the difference between leprosy prevalence and age at diagnosis between two sub-populations of individuals born and not born in the village. We also describe a homogenous distribution of cases across males and females.
Leprosy cumulative prevalence among those born and those not born in the village was 5.9% and 22.9%, respectively. It is reasonable to assume that the high cumulative prevalence of leprosy among the population not born in the village is because many of these individuals moved to the village due to compulsory isolation, in place in Brazil at the time the village was designated as an isolation site (1923) and until the early-1960s. In contrast, the much lower cumulative prevalence among the subpopulation born in the village is aligned with previous estimates indicating that approximately 5% of the population is naturally susceptible to leprosy^7,8^, a proportion that seems to stand even in a hyperendemic, socially homogenous environment. Previous attempts to determine the proportion of individuals naturally susceptible to leprosy have yielded varied results, ranging from less than 1–12%^5,9^. It is important to highlight that susceptibility to leprosy depends on multiple factors, including genetics.
Three factors may contribute to the age-onset difference between the village subpopulations born and not born. First, more frequent epidemiological surveys in a village well known for being hyperendemic may lead to earlier detection and diagnosis; second, individuals born in the village are mostly descendants of leprosy-affected individuals and, therefore, likely more genetically susceptible to the disease^6^; finally, individuals born in the village may be under lifelong exposure to leprosy cases, potentially increasing their risk of infection. If true, the 15-year average age of diagnosis in this sub-population may indicate the time between early exposure and clinical manifestation of the disease. The occurrence of leprosy cases among children is considered an indicator of ongoing transmission in the community^10,11^, which supports our findings. The leprosy incubation period has been a research subject for several decades. It has been proposed that the disease has an average incubation period of approximately five years^4,12^. An early attempt to estimate the incubation period of leprosy based on patient self-reports reached 8.4 years^13^. In one study, data from secondary cases of leprosy among household contacts revealed an average time of disease onset of 4.3 (± 3.3) years, irrespective of the clinical form^14^; in this study, the time between the diagnosis of an index leprosy patient and the occurrence of a leprosy secondary case in a household contact was considered a proxy for incubation. It should be noted, however, that the study was performed in a hyper-endemic region; thus, the estimate may be biased by the assumption that exposure occurs only through the index case living in the same household. A study involving 35 military veterans reported a median onset time ranging from 2 to 5 years for tuberculoid and 8 to 12 years for lepromatous leprosy; however, these findings did not reach statistical significance^15^. Furthermore, estimates of a 15 to 30-year incubation period in animal models primarily rely on non-human primates, a non-consensus model for leprosy studies^15–17^. A screening of the available literature shows that many references of the incubation period refer to a book Chap^18^, describing it as being between 2 and 5 years; careful analysis of the references used in the book revealed that the information is based on studies of different experimental designs, resulting in findings ranging from 2 to 30 years. More recently, a case report was published about a male individual with an incubation period of 50 years before symptom onset^19^. Together, these studies emphasize the variability in the data related to the incubation period of leprosy.
Another interesting observation is the distribution of leprosy across sexes in the Prata population. While it is commonly reported that leprosy is more prevalent in males compared to females^20,21^, we found that this difference is not clear among sub-populations born and not born in the Prata Village. The proportions of males and females among both sub-populations were similar, with 51.5% males and 48.5% females among those born in the village and 48.9% males and 51.1% females among those not born in the village. Given that the disease is incorporated into the culture of the village and is thus more naturally perceived by the population, our data suggests that the sex effect on leprosy distribution may be more influenced by behavioral factors rather than inherent biological differences between males and females. This is supported by the lack of gender-related differences in prevalence observed among wild armadillos^22^ and wild chimpanzees^23^.
Importantly, if the population in the Prata Village indeed has increased natural susceptibility to leprosy, we would expect to observe a higher incidence of reinfection/relapse cases. This is supported by a recent study that reported high rates of leprosy recurrence in the village, along with a high prevalence of drug-resistant strains of M. leprae^24^. These observations suggest that the Prata Village population may be both (i) more susceptible to leprosy as well as (ii) exposed to resistant bacteria; the combination of these independent aspects of the disease pathogenesis creates an ideal environment for the persistence of leprosy hyperendemicity.
This study has several limitations to consider. For example, as we are confident in our strategy of cross-checking clinical records of different sources to characterize a case, we are also aware that clinical examination would be interesting, particularly for the self-reported non-affected population. However, examining the entire population of the village would be an enormous task; also, we believe that the risk of a self-reported non-affected individual being affected is reduced by (i) the fact that the village is maintained under constant surveillance, with an MD dermatologist visiting the village on regular basis, and (ii) because leprosy is widespread and part of the local culture, the stigma associated with the status of affected is reduced amongst the villagers, favoring seeking for medical help. Our observations also suggest that some villagers may perceive being diagnosed with leprosy as a positive outcome, as they may become eligible for financial governmental support^25^.
Another limitation, particularly regarding our arguments on the proportion of naturally susceptible individuals and the disease’s incubation period, is that one must assume equal and permanent exposure of all newborn individuals to M. leprae throughout their lives, which is impossible to prove. For example, our approach does not consider the exact clinical form of each leprosy case and the presence or absence of an index case within the household of a new case^26^. On the other hand, the Prata village presents (i) a high prevalence of leprosy (12.8%), (ii) most of the cases of high bacillary load (40.5% were lepromatous), and (iii) a homogenous environment with a low degree of social isolation between leprosy affected and non-affected individuals. These observations favor the assumption that the Prata population is under constant high exposure.
In summary, the opportunity to compare two distinct subpopulation samples sharing a geographically limited, homogenous environment revealed differences in both the cumulative prevalence and the median age of diagnosis of leprosy between the groups born versus not-born in the village. Interestingly, no sex-related differences were observed between the two groups. In conclusion, although extrapolating our findings to more open populations must be done carefully, we believe we used a unique population as a model to provide additional insights into the epidemiology of leprosy.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Britton, W. J. & Lockwood, D. N. J. Leprosy Lancet 363, 1209–1219 (2004).10.1016/S 0140-6736(04)15952-715081655 · doi ↗ · pubmed ↗
- 2World Health Organization. Global leprosy (Hansen disease) update, 2023: Elimination of leprosy disease is possible—time to act! [Internet]. https://www.who.int/publications/i/item/who-wer 9937-501-521 (2024).
- 3World Health Organization. Guidelines for the Diagnosis, Treatment and Prevention of Leprosy (World Health Organization, Regional Office for South-East Asia, 2018).
- 4Massone, C. & Nunzi, E. Pathogenesis of leprosy. In Leprosy and Buruli Ulcer–A Practical Guide, vol. 2 (eds. Nunzi, E. et al.) 1–570 (Springer, 2022).
- 5Lockwood, D. N. J. & Suneetha, S. Leprosy: Too Complex a Disease for a Simple Elimination Paradigm, vol. 83 (Bulletin of the World Health Organization, 2005).PMC 262421015798849 · pubmed ↗
- 6World Health Organization. Weekly epidemiological record. Global leprosy (Hansen disease) update, 2022: new paradigm—control to elimination [Internet]. https://www.who.int/publications/i/item/who-wer 9837-409-430 (2023).
- 7Rajani, A. J. et al. Half a century in hiding: a unique case of Tuberculoid Leprosy with an unprecedented incubation period. Am. J. Med. Case Rep.25, 7 (2024).10.12659/AJCR.942048 PMC 1087764038351602 · doi ↗ · pubmed ↗
- 8Pescarini, J. M. et al. Socioeconomic risk markers of leprosy in high-burden countries: a systematic review and meta-analysis. P Lo S Negl. Trop. Dis.12, 7 (2018).10.1371/journal.pntd.0006622 PMC 605325029985930 · doi ↗ · pubmed ↗