Pulmonary Enteric Adenocarcinoma in a Super‐Elderly Patient: A Case Report and Literature Review
Akira Shimamoto, Natsumi Kojo, Haruko Saiki, Akinobu Hayashi, Motoshi Takao

TL;DR
This paper reports a rare case of lung cancer in an 85-year-old man, showing successful diagnosis and surgery despite his age.
Contribution
The case highlights the use of immunohistochemistry for diagnosing PEAC and successful surgery in a super-elderly patient.
Findings
The patient had a 9-year history of a growing pulmonary nodule before diagnosis.
Immunohistochemistry confirmed PEAC with CK7, CK20, and CDX2 positivity.
The patient remained disease-free one year after surgery without adjuvant therapy.
Abstract
Pulmonary enteric adenocarcinoma (PEAC) is an extremely rare subtype of non‐small cell lung cancer, characterised by histopathological features that resemble colorectal adenocarcinoma. Here, we report a case of PEAC in an 85‐year‐old male who presented with a pulmonary nodule initially identified at the age of 76. Initial PET‐CT (maximum standardised uptake value [SUVmax] = 2.8) was inconclusive, leading to strict follow‐up. Over 9 years, the nodule enlarged significantly (3.2 cm, SUVmax = 8.4). A transbronchial biopsy confirmed adenocarcinoma, and the patient underwent successfully video‐assisted thoracoscopic surgery with lymph node dissection. The histopathological analysis revealed CK7 and CK20 positivity, focal CDX2 positivity, and TTF‐1 negativity, confirming PEAC. Despite advanced age, the patient tolerated surgery well without adjuvant therapy. At the one‐year postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
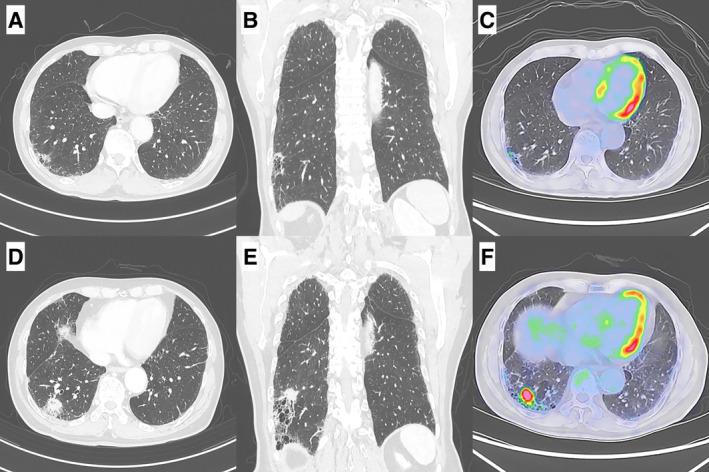 FIGURE 1
FIGURE 1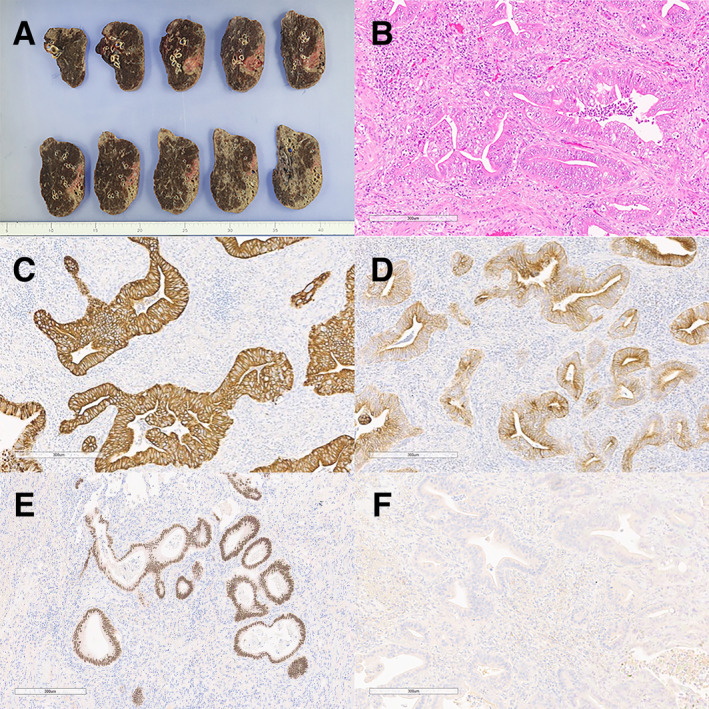 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Genetic factors in colorectal cancer · Gastrointestinal disorders and treatments
Introduction
1
Pulmonary enteric adenocarcinoma (PEAC) is an exceptionally rare subtype of non‐small cell lung cancer (NSCLC), accounting for less than 0.5% of all primary lung adenocarcinomas [1]. It is characterised by histopathological features resembling colorectal adenocarcinoma, including irregular glandular structures lined by columnar epithelial cells and immunohistochemical positivity for intestinal markers such as CK20 and CDX2. First described in 1991, PEAC was officially classified as a distinct variant of invasive lung adenocarcinoma by the World Health Organization (WHO) in 2015 [2].
Diagnosing PEAC is particularly challenging due to its histopathological and immunohistochemical similarities with metastatic colorectal cancer (MCRC). Accurate differentiation relies on a combination of clinical, radiological, and pathological analyses. Immunohistochemical studies play a pivotal role, especially in distinguishing PEAC from MCRC in patients without a known history of colorectal cancer.
Here, we report a rare case of PEAC in an 85‐year‐old male, emphasising the diagnostic approach, surgical treatment, and favourable postoperative outcome. This case underscores the importance of immunohistochemical markers in establishing the diagnosis and highlights the potential for successful surgical management in a super‐elderly patient.
Case Report
2
A male patient with a history of non‐alcoholic liver disease underwent routine whole‐body CT at the age of 76, which revealed a 5 mm solitary nodule in the lateral basal segment of the right lung. A subsequent PET‐CT was performed for further evaluation, revealing a maximum standardised uptake value (SUVmax) of 2.8. This finding made it challenging to differentiate between lung cancer and inflammation. The lesion was closely monitored through serial CT scans due to its indeterminate nature.
At the age of 85, after 9 years of strict CT follow‐up, the nodule demonstrated significant enlargement, forming a solid, irregular mass measuring 3.2 cm. PET‐CT revealed significant ^18^F‐fluorodeoxyglucose uptake (SUVmax = 8.4) within the lesion, with no evidence of extrathoracic metastasis (Figure 1). A transbronchial lung biopsy confirmed the diagnosis of adenocarcinoma. Although super‐elderly, his good performance status and the localised stage of the tumour (cT2aN0M0, stage IB) made him a candidate for surgical resection. The patient also underwent upper gastrointestinal endoscopy (UGIF) and colonoscopy (CF) as part of an unrelated evaluation, revealing no abnormalities.
Chest CT and PET/CT findings. (A, B) Chest CT showed a 5 mm solitary nodule in the lateral basal segment of right lung at 9 years before surgery. (C) PET/CT showed an increased 18F‐fluorodeoxyglucose (FDG) uptake in the lesion (maximum standardised uptake value [SUVmax] = 2.8) at 9 years before surgery. (D, E) Chest CT revealed the lesion had grown to 3.2 cm immediately before surgery. (F) PET/CT revealed an increased FDG uptake (SUVmax = 8.4) in the lesion immediately before surgery.
The patient subsequently underwent video‐assisted thoracoscopic surgery (VATS) with right lower lobectomy and systematic lymph node dissection (ND2a‐1). The postoperative course was uneventful, with the chest drain removed on postoperative day 1 and discharge on postoperative day 4.
Detailed histopathological examination of the resected specimen revealed irregular glandular structures with columnar epithelial cells exhibiting eosinophilic cytoplasm. Immunohistochemical analysis showed positivity for CK7 and CK20, focal positivity for CDX2, and negativity for TTF‐1 and MUC‐2 (Figure 2). These findings confirmed the diagnosis of PEAC. The tumour, including its invasive component, measured 4.2 cm in maximum diameter upon histopathological examination, resulting in a final pathological stage of pT2bN0M0 (stage IIA).
Representative histopathological findings of the resected specimen. (A) Macroscopic image of the resected specimen showing a well‐demarcated tumour in the lateral basal segment of the right lung. (B) Haematoxylin and eosin staining demonstrating irregular glandular structures with columnar epithelial cells exhibiting eosinophilic cytoplasm. (C) Immunohistochemical staining showing strong positivity for CK7. (D) Immunohistochemical staining showing positivity for CK20. (E) Immunohistochemical staining showing focal positivity for CDX2. (F) Immunohistochemical staining showing negativity for TTF‐1.
Considering his advanced age and lack of high‐risk features, adjuvant therapy was not administered. At the one‐year postoperative follow‐up, the patient remained disease‐free with no evidence of recurrence.
Discussion
3
PEAC is a diagnostically challenging and rare subtype of NSCLC. First reported in 1991 and officially classified by the WHO in 2015, PEAC accounts for less than 0.5% of all primary lung adenocarcinomas. To date, fewer than 100 cases have been documented in the literature. The rarity of PEAC has resulted in a lack of standardised diagnostic and treatment guidelines, and most published studies consist of single‐institution case series or isolated case reports.
Accurate differentiation between PEAC and MCRC is critical due to their overlapping histopathological and immunohistochemical characteristics. Key immunohistochemical markers, including CK20, CDX2, and TTF‐1, play a pivotal role in distinguishing PEAC from other adenocarcinomas. CK20 and CDX2 positivity, combined with TTF‐1 negativity, strongly suggest intestinal differentiation in primary lung adenocarcinomas. Recent studies have also emphasised the utility of next‐generation sequencing alongside immunohistochemistry in differentiating PEAC from MCRC [3]. Additionally, the absence of gastrointestinal symptoms, no history of colorectal cancer, and normal findings on UGIF and CF examinations were critical in ruling out a primary gastrointestinal malignancy.
Surgical resection remains the cornerstone of treatment for localised PEAC, as supported by multiple case studies. In elderly patients, the risks and benefits of surgery must be carefully weighed. Despite his advanced age, the patient successfully underwent VATS with systematic lymph node dissection, demonstrating that advanced age should not preclude surgical consideration in well‐selected cases. The procedure was well tolerated, and the postoperative course was uneventful, highlighting the feasibility of surgical management even in super‐elderly patients with good performance status.
The prognosis of PEAC appears comparable to that of conventional NSCLC when appropriately treated [4]. Emerging studies highlight that PEAC may harbour actionable mutations, including KRAS and mismatch repair deficiencies, suggesting potential avenues for personalised therapy and future clinical trials [5]. Although our patient did not receive adjuvant therapy due to his advanced age and early‐stage disease, the absence of recurrence at the one‐year follow‐up supports the efficacy of surgical intervention alone in this context.
This case is consistent with existing literature in terms of immunohistochemical profile and favourable surgical outcomes. However, it underscores the importance of individualised surgical planning and careful risk assessment, particularly in super‐elderly patients. Further research is needed to establish the role of targeted therapies and immunotherapy in the management of PEAC and to develop standardised diagnostic and treatment protocols.
Author Contributions
Akira Shimamoto wrote the manuscript. Haruko Saiki examined the patient, and Akira Shimamoto, Natsumi Kojo, and Motoshi Takao performed surgery. Akinobu Hayashi diagnosed pathologically. All authors have approved the final version of the manuscript for submission.
Ethics Statement
The authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. F. Tu , L. Y. Sheng , J. Y. Zhou , et al., “Diagnosis and Treatment of Primary Pulmonary Enteric Adenocarcinoma: Report of Six Cases,” World Journal of Clinical Cases 9, no. 30 (2021): 9236–9243.34786410 10.12998/wjcc.v 9.i 30.9236 PMC 8567515 · doi ↗ · pubmed ↗
- 2M. S. Tsao and R. S. Fraser , “Primary Pulmonary Adenocarcinoma With Enteric Differentiation,” Cancer 68, no. 8 (1991): 1754–1757.1913519 10.1002/1097-0142(19911015)68:8<1754::aid-cncr 2820680818>3.0.co;2-e · doi ↗ · pubmed ↗
- 3J. Zhang , C. Xiang , Y. Han , et al., “Differential Diagnosis of Pulmonary Enteric Adenocarcinoma and Metastatic Colorectal Carcinoma With the Assistance of Next‐Generation Sequencing and Immunohistochemistry,” Journal of Cancer Research and Clinical Oncology 145, no. 1 (2019): 269–279.30415301 10.1007/s 00432-018-2788-0PMC 11810349 · doi ↗ · pubmed ↗
- 4Q. Wang , L. Zhang , H. Li , L. Liu , X. Sun , and H. Liu , “Clinical Features and Prognosis of Pulmonary Enteric Adenocarcinoma: A Retrospective Study in China and the SEER Database,” Frontiers in Oncology 13 (2023): 1099117.37051525 10.3389/fonc.2023.1099117 PMC 10083384 · doi ↗ · pubmed ↗
- 5S. Kishikawa , T. Hayashi , K. Takamochi , et al., “Frequent Nuclear Beta‐Catenin Expression in Pulmonary Enteric‐Type Adenocarcinoma According to the Current World Health Organization Criteria,” Virchows Archiv 483, no. 5 (2023): 699–703.37740071 10.1007/s 00428-023-03657-9 · doi ↗ · pubmed ↗