Understanding the Impact of Skull Base Osteomyelitis: A Retrospective Analysis of 14 Cases
Padmanabhan Karthikeyan, P.S. Divya, Kirubhagaran Ravichandran, Venkataramani Agathiyanathan

TL;DR
This study examines 14 cases of skull base osteomyelitis, focusing on symptoms, treatment effectiveness, and outcomes, particularly in diabetic patients.
Contribution
The paper provides a detailed retrospective analysis of SBO cases, highlighting treatment resistance and rare complications like septic arthritis.
Findings
All 14 patients were diabetic and presented with otalgia and purulent otorrhea.
21% of cases had facial palsy, and 14% developed septic arthritis of the temporomandibular joint.
43% of SBO cases showed resistance to ciprofloxacin, but all achieved disease resolution with combined treatment.
Abstract
Purpose Skull base osteomyelitis (SBO) or malignant otitis externa (MOE) is an invasive bacterial infection (a rarely fungal as well as potentially aggressive infection that involves the external auditory canal up to the temporal bone and skull base. This study provides insight into the various clinical presentations of skull base osteomyelitis, the effectiveness of different treatment approaches, and the overall prognosis of SBO based on our case series. Materials and methods This observational study comprises 14 SBO cases, including their diagnosis, follow-up, and treatment. Results Otalgia and purulent otorrhea were observed in all our cases as common symptoms. All patients were diabetic. Three cases (21%) presented with facial palsy and two cases (14%) reported a rare progression of SBO resulting in septic arthritis of the temporomandibular joint. In our study, 43% of the cases…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2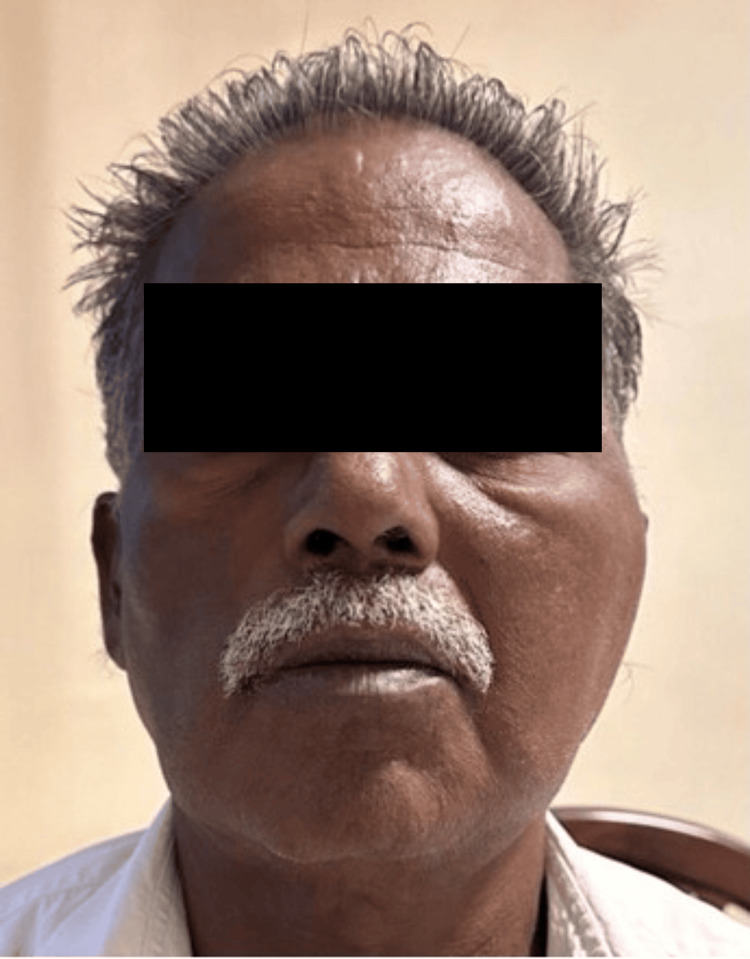 Figure 3
Figure 3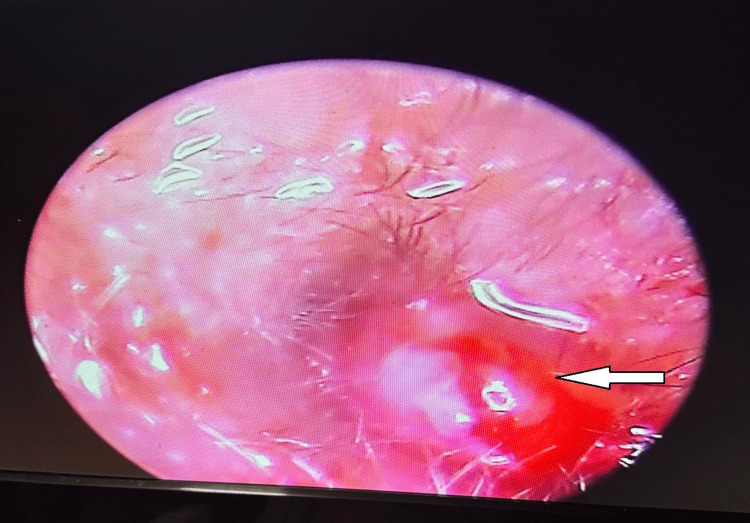 Figure 4
Figure 4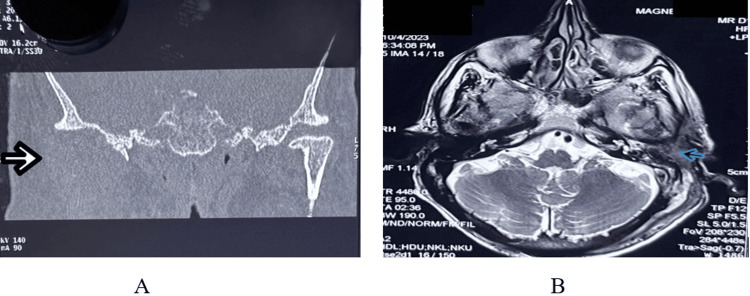 Figure 5
Figure 5| Diagnostic criteria of skull base osteomyelitis |
| Major (obligatory) signs |
| 1) Pain |
| 2) Exudate |
| 3) Edema |
| 4) Granulations |
| 5) Micro abscesses |
| 6) Positive technetium-99 (99Tc) scan or failure of local treatment after more than one week |
| Minor (occasional) signs |
| 7) Pseudomonas |
| 8) Positive radiograph |
| 9) Diabetes mellitus |
| 10) Cranial nerve involvement |
| 11) Debilitating conditions |
| 12) Old age |
| Findings | Numbers |
| Involvement of disease outside EAC | 14 |
| Evidence of bone erosion | 4 |
| Intracranial involvement | - |
| Cases of SBO presenting with complications | ||||||
| CASE | 9 | 10 | 11 | 12 | 13 | 14 |
| Age/Sex | 85/M | 82/M | 52/F | 70/M | 76/M | 87/F |
| Symptoms | Left ear pain, Left ear discharge, Swelling behind the left ear. | Left ear pain | The patient came with a recurrence of left ear pain after 2 months. | The patient came with a recurrence of the disease after 3 months with left ear pain and left preauricular area swelling. | Right ear pain, swelling in front of the right ear. | Right ear pain, swelling in front of the right ear. |
| Ear examination | Left postauricular - A diffuse, erythematous, warm, and tender swelling of approximately 3x2 cm present; it was cystic, fluctuant, with no pus point, and no discharging sinus. | Left preauricular region - swelling +, warmth +. | Right preauricular region - swelling +, tenderness +, warmth + | Right preauricular region - swelling +, tenderness +, warmth + | ||
| Duration of diabetes (years) | 35 | 40 | 10 | 25 | 20 | 35 |
| On regular treatment for diabetes | + | + | + | + | + | + |
| Total count cells/cumm | 18700 | 10000 | 8000 | 6400 | 8000 | 8400 |
| HbA1c (%) | 8.8 | 10 | 11 | 8.6 | 8 | 8 |
| Pus culture sensitivity | Pseudomonas aeruginosa, Klebsiella pneumoniae | Pseudomonas aeruginosa, Klebsiella pneumoniae | Pseudomonas aeruginosa, Klebsiella pneumoniae | Pseudomonas aeruginosa | Pseudomonas aeruginosa | - |
| Cranial nerve involvement | Left lower motor neuron facial palsy (Grade II) | Left lower motor neuron facial palsy (Grade IV) | Left lower motor neuron facial palsy (Grade I) | - | - | - |
| HRCT | + | + / MRI + | + | + | + ( Figure | + |
| Resistance to ciprofloxacin | + | + | + | + | - | - |
| Treatment given | Piperacillin and tazobactam 4.5g (IV,1-1-1) for 10 days. Ceftazidime 1g, IV, 1-0-1 for 5 days. Tab. levofloxacin 500 mg: 1-0-1 for 3 weeks | Piperacillin and tazobactam 4.5 g (IV, 1-1-1) for 10 days. Ceftazidime 1g IV, 1-0-1 for 5 days. Tab. levofloxacin. 500 mg: 1-0-1 for 3 weeks | Pperacillin and tazobactam 4.5g (IV, 1-1-1) for 10 days. Ceftazidime 1g: IV, 1-0-1 for 2 days 3. Tab. levofloxacin 500mg: 1-0-1 for 3 weeks | Piperacillin and tazobactam 4.5g (IV,1-1-1) for 10 days. Tab. levofloxacin 500mg: 1-0-1 for 3 weeks | Tab levofloxacin 500 mg 1-0-1 for 4 weeks | Tab levofloxacin 500 mg 1-0-1 for 4 weeks |
| Examination under microscopy | Granulation tissue with aural polyp excision and biopsy | Granulation tissue with aural polyp excision and biopsy | Granulation tissue with aural polyp excision and biopsy | Granulation tissue with aural polyp excision and biopsy. | - | Anterior wall of EAC granulation + |
| Biopsy results | Inflammatory aural polyp with dead bone | Inflammatory aural polyp with dead bone | Inflammatory aural polyp with dead bone | Inflammatory aural polyp | - | - |
| Surgical procedures | Incision and drainage of the left subperiosteal abscess under local anesthesia (Figure | Left mastoid exploration | Left aural polypectomy with surgical debridement of EAC | Left aural polypectomy with surgical debridement of EAC | - | - |
| Diagnosis | Left SBO with left subperiosteal abscess, left LMN facial palsy | Left SBO with left LMN facial palsy | Left SBO with left LMN facial palsy | Left SBO with septic arthritis of the left TMJ | Right SBO with septic arthritis of the right TMJ | Right SBO with septic arthritis of the right TMJ |
| Cases of SBO (Uncomplicated) | ||||||||
| CASE | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Age/Sex | 58/M | 70/M | 70/M | 85/M | 62/M | 50/M | 70/M | 70/M |
| Symptoms | Left ear pain, left ear blocking sensation, left ear discharge | Left ear pain, left ear discharge, Left ear blocking sensation | Left ear pain, left ear blocking sensation | Left ear pain, left ear discharge, and left hard of hearing | Left ear pain | Left ear pain and left ear discharge | Right ear pain | Right ear pain |
| Duration of diabetes (years) | 15 | 10 | 15 | 20 | 15 | 12 | 15 | 7 |
| On regular treatment for diabetes | + | - | + | - | + | + | + | + |
| Total count cells/cumm | 10,900 | 9,000 | 6800 | 8400 | 9200 | 9200 | 9200 | |
| HbA1c (%) | 11.2 | 12.2 | 7.3 | 7.1 | 14 | 9.4 | 14 | 7.5 |
| Pus culture sensitivity | Pseudomonas aeruginosa, Klebsiella pneumoniae | Escherichia coli, Pseudomonas aeruginosa | Pseudomonas aeruginosa, Klebsiella pneumoniae | Pseudomonas aeruginosa, Staphylococcus | Pseudomonas aeruginosa, Staphylococcus | Pseudomonas aeruginosa | Pseudomonas aeruginosa, Staphylococcus | Pseudomonas aeruginosa |
| Cranial nerve involvement | - | - | - | - | - | - | - | - |
| HRCT | + | + | + | + | + | + | - | - |
| Resistance to ciprofloxacine | - | - | - | + | - | + | - | - |
| Treatment given | Ciprofloxacin 400mg (IV, 1-0-1) for 7 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ciprofloxacin 400mg (IV, 1-0-1) for 10 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ciprofloxacin 400mg (IV 1-0-1) for 7 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ceftazidime 1g (IV 1-0-1) for 5 days. Levofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ciprofloxacin 400mg (IV 1-0-1) for 7 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Piperacillin and tazobactam 4.5g (IV,1-1-1) for 10 days. Levofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ciprofloxacin 400mg (IV, 1-0-1) for 7 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks | Ciprofloxacin 400mg (IV, 1-0-1) for 7 days. Ciprofloxacin 500mg (Per oral, 1-0-1) for 3 weeks |
| Examination under microscopy | Granulation tissue with aural polyp excision and biopsy | Granulation tissue excision and biopsy | Granulation tissue excision and biopsy | - | - | Granulation tissue with aural polyp excision and biopsy | - | Granulation tissue excision and biopsy |
| Biopsy results | Inflammatory aural polyp with dead bone | inflammatory aural polyp with dead bone | Inflammatory aural polyp | - | - | Inflammatory aural polyp with dead bone. | - | Granulation tissue |
| Surgical procedures | - | - | - | - | - | - | - | - |
| Diagnosis | Left SBO | Left SBO | Left SBO | Left SBO | Left SBO | Left SBO | Right SBO | Right SBO |
| Summary of clinical presentation, outcome, and management of MOE cases | ||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Head and Neck Surgical Oncology · Sinusitis and nasal conditions
Introduction
Skull base osteomyelitis (SBO), also known as necrotizing otitis externa (NOE) or malignant otitis externa (MOE), is an invasive bacterial infection as well as potentially aggressive infection that involves the external auditory canal (EAC) up to the temporal bone and skull base. Meltzer first reported SBO in 1959 [1]. Pseudomonas aeruginosa is a common causative organism, reported in up to 95% of cases in some studies [2]. Pseudomonas aeruginosa is a ubiquitous gram-negative rod. SBO is typically seen in elderly diabetes mellitus (DM) patients or immunocompromised patients.
SBO often presents with initial symptoms, such as ear pain (otalgia), discharge from the ear (otorrhea), and a sensation of fullness in the ear (aural fullness). These symptoms overlap with those of otitis externa (OE), potentially complicating diagnosis and delaying the initiation of appropriate treatment. The distinction is made when symptoms persist or worsen despite standard OE treatment, with red flags such as severe pain, cranial nerve involvement, or systemic signs. In more severe cases of SBO, patients may develop cranial neuropathies, with facial nerve palsy occurring in 17% to 26% of instances [3].
Antipseudomonal antimicrobials are the mainstay of therapy for malignant external otitis. Prior to the development of systemic agents, the mortality from this disease approximated 50%, with frequent recurrences. The cure rate has increased to 90% with the introduction of fluoroquinolones [1].
This study provides insight into the various clinical presentations of SBO, the effectiveness of different treatment approaches, and the overall prognosis of SBO based on our case series.
Materials and methods
Fourteen consecutive patients admitted to our hospital, Mahatma Gandhi Medical College and Research Institute (MGMCRI), affiliated with Sri Balaji Vidyapeeth (SBV), Puducherry, with a diagnosis of skull base osteomyelitis (SBO) within a period of six months from July 2023 to December 2023 were selected for this study. The diagnosis of SBO was based on Cohen and Friedman’s diagnostic criteria (Table 1) of major and minor signs. The patients' average age was 71 years (min 50 - max 87 years). The clinical presentation, management, outcome, and complication of SBO were analyzed in our case series.
Results
Out of 14 patients, 12 were male and 2 were female. On clinical history, patients presented with purulent otorrhea and otalgia, which were observed in all our patients. All of our cases presented with granulation tissue and polyps in the EAC on examination. On examination, tympanic membrane perforations were present in two cases. All 14 patients had a preexisting diagnosis of diabetes mellitus for more than 10 years. All the patients had documented microbiological evidence of Pseudomonas in ear swab cultures. There was a left-sided predominance of disease (11 cases of left SBO), with no involvement of the contralateral side. The patients' average age was 71 years (min 50 - max 87 years). The most frequent symptoms observed initially were prolonged ear pain and discharge. Notably, the ear pain was severe and frequently occurred during nighttime (termed nocturnal otalgia). Glycated hemoglobin (HbA1c) levels were recorded in all the patients. Almost all our patients (14 cases) underwent high-resolution computed tomography (HRCT) of the temporal bone. Cases showed evidence of soft tissue density in the left EAC with involvement of the disease around the mastoid and middle ear. Four cases had evidence of bony erosion (Table 2).
In our series of cases, there were no fatalities associated with SBO. Out of the 14 patients, 3 (23%) had presented with seventh cranial nerve palsy (Table 3, Figure 1), and 1 patient presented with left subperiosteal abscess requiring incision and drainage (Figure 2).
Left LMN facial palsyLMN: lower motor neuron
A postoperative picture of the incision and drainage done for a left subperiosteal abscess
Three cases (23%) presented with a rare progression of SBO, resulting in septic arthritis of the TMJ, which was treated with oral antibiotic levofloxacin, and excision of granulation tissue was performed, which showed complete resolution (Figure 3, Table 3).
Left TMJ septic arthritis (left preauricular swelling)TMJ: temporomandibular joint
All our patients had daily cleaning of the auditory canal, application of antimicrobial ear drops, and long-term systemic antibiotic therapy followed by three weeks of oral antibiotic therapy. Five patients had betamethasone (0.1% w/w) plus neomycin (0.5% w/w) ointment filled in the EAC over the granulation, out of which four patients had significant improvement with reduction of granulation tissue (Figure 4).
Otoendoscopy of the left external auditory canal showing left aural polyp and granulation tissue (arrow)
Local debridement of granulating tissue was performed in patients. The patients were prescribed a three-week course of oral ciprofloxacin at a dosage of 500 mg twice daily for treatment. Since, in our case series, 6 (43%) cases had resistance to ciprofloxacin, these patients were initially treated with intravenous ceftazidime or intravenous piperacillin and tazobactam for 7 to10 days along with oral levofloxacin for three weeks. We noted that six cases having resistance to ciprofloxacin had an elevated risk of experiencing recurrences, advancing to facial nerve palsy, and developing septic arthritis of the TMJ. A resolution of the disease was achieved in almost all our cases. All our cases were reviewed after three weeks (Tables 3, 4).
A: High-resolution computed tomography showing right TMJ septic arthritis. B: Magnetic resonance imaging of the brainA: High-resolution computed tomography showing right TMJ septic arthritis and anterior dislocation of the right TMJ. B: T2-weighted MRI showing hyperintense signal due to diffuse fluid accumulation filling the left middle ear cavity, mesotympanum, posterior epitympanum, and retrotympanic recess, with extension into the peri-ossicular region abutting the facial nerve canal.TMJ: temporomandibular joint
Discussion
MOE has become manageable with the introduction of new antibiotics. However, the prognosis deteriorates with the onset of skull-base osteomyelitis or other complications. MOE is a potentially fatal infection affecting the lateral temporal bone. According to our study, the predominant symptoms of MOE include ear pain (nocturnal otalgia), ear discharge, and ear-blocking sensation [5].
As in our study, the data exhibited a mean of 65, ranging from a minimum of 50 to a maximum of 85. The increasing age has a significant impact on disease incidence. Several hypotheses have been proposed for the physiologic connection between advanced age and SBO, including decreased epithelial migration of the ear canal and microvascular disease inhibiting a proper immune response [2]. Advanced age has been linked to comorbidities, including diabetes, which is known to be associated with impaired immune response and microvascular disease [6].
The duration of DM and the patient’s serum glucose levels were considered to influence the prognosis of MOE [7]. Our study showed that an increase in blood glucose level (HbA1C) and irregular treatment had an impact on the disease course and severity.
In the available literature, men are more commonly affected than women [8]. Our study similarly observes a higher incidence of SBO in men as compared to women.
There are no studies signifying the incidence of affected sides in SBO. In our study, we observed that the left ear was affected more than the right ear, although the etiology of this could not be explained.
Pseudomonas aeruginosa has been identified as the predominant pathogen in 80-98% of skull base osteomyelitis cases [9]. In our case series, Pseudomonas aeruginosa was cultured in all patients. However, it is important to note that fungal pathogens, such as Aspergillus and Candida species, also play a significant role, particularly in immunocompromised patients, including those with hematologic malignancies or poorly controlled diabetes [10]. The prevalence of specific pathogens varies significantly across studies and patient populations, highlighting the need for individualized diagnostic approaches and targeted therapy. Additional studies reporting fungal infections as a cause of skull base osteomyelitis emphasize this variability.
CT is a fast and economical tool for confirming the diagnosis of SBO but has limited value in predicting outcomes [11]. Anatomical imaging enables the localization of the disease and assessment of its progression or resolution. Bone erosion can only be demonstrated on CT scans once bone demineralization has occurred [12]. However, HRCT of the temporal bone was taken in all our cases, through which the extent of the disease was assessed.
The facial nerve is the most commonly affected cranial nerve due to its proximity to the EAC [12]. In our study, three patients were affected by facial nerve palsy.
Over the past 15 years, oral ciprofloxacin has been the standard treatment for MOE, caused by Pseudomonas aeruginosa, due to which a gradual resistance to ciprofloxacin is developing. In a study over a 16-month period, 5 cases of SBO progressed, with the development of cranial nerve palsies in 4 cases, despite oral ciprofloxacin [8]. In our analysis, we noted that six cases with resistance to ciprofloxacin had an elevated risk of recurrences, advancing to facial nerve palsy, and developing septic arthritis of the TMJ. Therefore, patients with resistance to ciprofloxacin have a poor prognosis.
Otitis externa spreading to the TMJ is rare. In a study of two elderly patients with predisposing factors, it was found that a high index of suspicion and early aspiration of the joint enabled the diagnosis to be made and subsequent treatment to be instigated [13]. We reported three cases with early involvement of the TMJ joint, and a complete resolution was achieved. However, early involvement of the joint from SBO could be related to anatomical factors such as failure of closure of Huschke's foramen in early life; this leads to herniation of the TMJ into the anterior wall of the bony external ear canal [13].
A multidimensional approach, including surgical debridement, is particularly important when conservative treatment alone fails or when there is significant tissue involvement, highlighting the evolving understanding of SBO management in challenging patient populations [14]. Similarly in our study, four patients underwent surgical procedures, including incision and drainage of a left subperiosteal abscess, left mastoid exploration, and left aural polypectomy with EAC debridement. These interventions were necessary for patients with refractory or extensive SBO, where conservative treatment alone was insufficient. Surgical debridement, combined with antimicrobial therapy, was crucial in controlling infection and improving outcomes.
Conclusions
In conclusion, our cases of SBO often present with otalgia, edema, and otorrhea. Physicians must be aware of the possibility that elderly, diabetic, and immunocompromised patients with persistent otalgia after refractory external otitis media may be suffering from SBO. Timely diagnosis and treatment significantly improve the prognosis of SBO. Computed tomography scans have been instrumental in diagnosing SBO. Our study revealed a noticeable tendency toward a higher occurrence on the left side in SBO cases. For this, further research is required to form a hypothesis. Poor prognosis is seen in patients with resistance to ciprofloxacin. Therefore, with early diagnosis, good control over the glycemic index, prolonged medical management, and local debridement, patients are likely to have a better prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pyocyaneous osteomyelitis of the temporal bone, mandible and zygoma Laryngoscope Meltzer PE Kelemen G 13001316691959 https://doi.org/10.1288/00005537-195910000-00006
- 2Malignant external otitis: insights into pathogenesis, clinical manifestations, diagnosis, and therapy Am J Med Rubin J Yu VL 391398851988 https://pubmed.ncbi.nlm.nih.gov/3046354/304635410.1016/0002-9343(88)90592-x · doi ↗ · pubmed ↗
- 3Cranial nerve involvement in malignant external otitis: implications for clinical outcome Laryngoscope Mani N Sudhoff H Rajagopal S Moffat D Axon PR 90791011720071747369410.1097/MLG.0b 013e 318039 b 30f · doi ↗ · pubmed ↗
- 4The diagnostic criteria of malignant external otitis J Laryngol Otol Cohen D Friedman P 2162211011987310654710.1017/s 0022215100101562 · doi ↗ · pubmed ↗
- 5Malignant otitis externa - a retrospective study of 15 patients treated in a tertiary healthcare center J Int Adv Otol Bhat V Aziz A Bhandary SK Aroor R Kamath PSD Saldanha M 7276112015 https://doi.org/10.5152/iao.2015.4302622372310.5152/iao.2015.430 · doi ↗ · pubmed ↗
- 6Clinical outcome parameters for necrotizing otitis externa Otol Neurotol Verim A Naiboğlu B KaracaÇ Seneldir L Külekçi S OysuÇ 371376352014 https://doi.org/10.1097/MAO.00000000000002492444829810.1097/MAO.0000000000000249 · doi ↗ · pubmed ↗
- 7Predicting outcome of malignant external otitis Otol Neurotol Joshua BZ Sulkes J Raveh E Bishara J Nageris BI 339343292008 https://doi.org/10.1097/MAO.0b 013e 31816618791831739610.1097/MAO.0b 013e 3181661879 · doi ↗ · pubmed ↗
- 8Resistance of Pseudomonas to ciprofloxacin: implications for the treatment of malignant otitis externa J Laryngol Otol Bernstein JM Holland NJ Porter GC Maw AR 11812312120071699595910.1017/S 0022215106002775 · doi ↗ · pubmed ↗