A comprehensive operative risk assessment driving the application of major and emergency surgery in octogenarians
Francesco Puccetti, Alessandro Francesco Armienti, Stefano Turi, Lorenzo Cinelli, Riccardo Rosati, Ugo Elmore, Lavinia Alessandra Barbieri, Lavinia Alessandra Barbieri, Silvia Battaglia, Andrea Cossu, Lorenzo Gozzini, Davide Socci, Elio Treppiedi, Alessia Vallorani

TL;DR
This paper presents a case showing that assessing octogenarians' overall health, not just age, leads to better surgical decisions.
Contribution
The paper introduces a comprehensive function-based assessment approach for surgical decision-making in elderly patients.
Findings
A multidimensional assessment improved therapeutic strategy for an 83-year-old with esophageal cancer.
Prehabilitation and tailored surgery led to successful outcomes despite the patient's frailty.
Systematic evaluation helps identify functional optimization areas in fragile elderly patients.
Abstract
Medical decisions driving the clinical management of octogenarians who require either major or urgent surgery still depend on the patient's age rather than individual functions. This report created the privileged opportunity to illustrate the clinical effectiveness of a comprehensive function‐based assessment. This was the case of an 83‐year‐old gentleman presenting with severe malnutrition and debility due to esophageal cancer. Multidimensional assessments were systematically performed to design the best‐tailored therapeutic strategy, including prehabilitation, elective esophagectomy, and emergency laparotomy with ileocolic resection for postoperative hemorrhagic shock due to an occult colonic tumor. This clinical case highlights the need for a systematic and comprehensive assessment of fragile octogenarians, allowing accurate patient evaluation, identification of areas of functional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
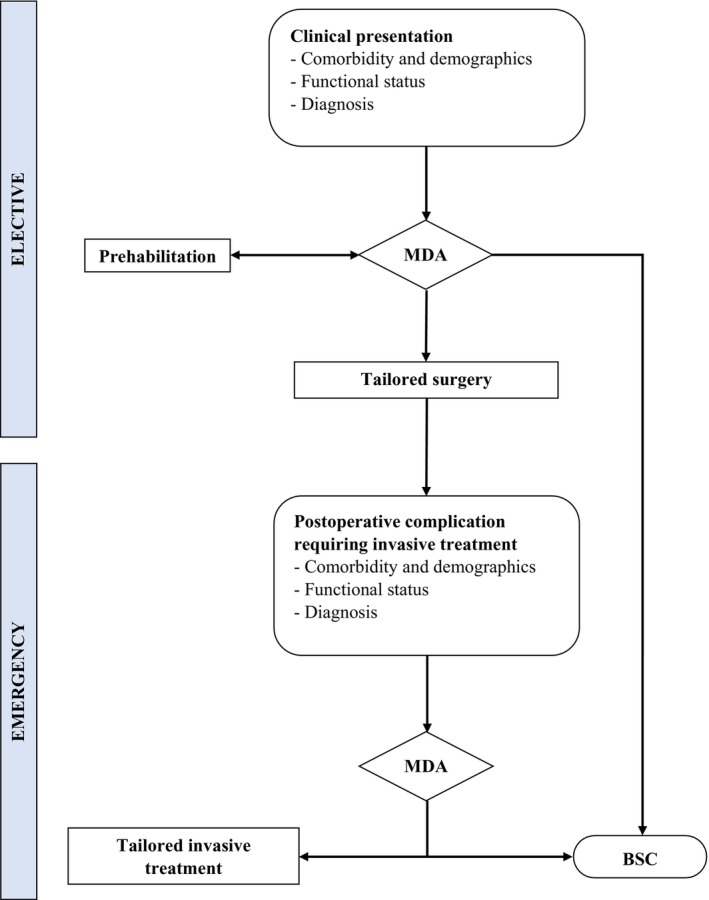 FIGURE 1
FIGURE 1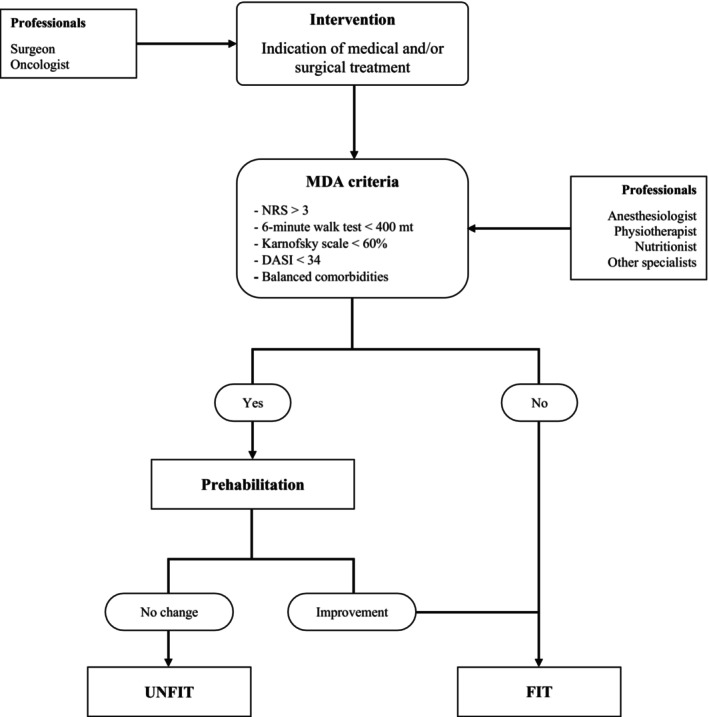 FIGURE 2
FIGURE 2| At the diagnosis | Elective major surgery | Urgent surgery | |
|---|---|---|---|
| Age | 83 | 83 | 83 |
| ASA physical status classification | 3 | 3 | 3 |
| NRS | 5 | 3 | 3 |
| Karnofsky performance scale | 50% | 70% | 30% |
| Respiratory function impairment | Moderate | Mild | Severe |
| Cardiac function impairment | Mild | Mild | Mild |
| Functional impairment | Severe | Mild | Severe |
| Decision | Non‐fit for surgery without an adequate prehabilitation | Fit for minimized surgery (transhiatal esophagectomy with two‐lung ventilation) with possible ICU recovery for postoperative monitoring | Fit for minimized surgery (no lymphadenectomy) and minimized anesthesia (regional analgesia), and possible ICU recovery for postoperative monitoring |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Hip and Femur Fractures · Enhanced Recovery After Surgery
INTRODUCTION
1
Given the considerable rise in global life expectancy, patients requiring in‐hospital invasive treatments have been gradually aging (Fowler et al., 2019). The increasing proportions of elderly patients within the surgical population has moved healthcare providers and multidisciplinary teams to early identify more specific criteria for operative risk assessment. Accordingly, the patient's age at the moment of surgery turned out to be a non‐univocal indicator of fitness to surgery, while the balance between patient's biological characteristics and type of surgical procedures may provide elements for a more precise operative risk assessment. Frailty is defined as the increased vulnerability resulting from reductions in physiological reserve and multisystem functions and represents the main determinant of the operative stress response in the elderly (Lin et al., 2016). A prompt and comprehensive multidimensional assessment (MDA) is the key element for allocation of resources, identification of optimization areas, and careful choices in geriatric or palliative settings. This report describes the clinical case of an octogenarian who, further to the precise definition and enhancement of his functional reserve, underwent tailored approaches of esophagectomy for cancer and emergency laparotomy afterward.
CASE PRESENTATION
2
The present case report has been reported in compliance with the Consensus‐based Clinical Case Reporting Guidelines (CARE). An 83‐year‐old gentleman presented with significant medical history (i.e., severe chronic obstructive pulmonary disease, insulin‐dependent diabetes, and hypertension) and physical deterioration due to malnourishment (i.e., complete dysphagia with about 8 kg weight loss in 9 weeks) secondary to a locally advanced esophageal adenocarcinoma. According to our dedicated institutional board a MDA was performed, involving different medical specialists, such as surgeon, anesthetist, oncologist, physiotherapist and nutritionist. Regarding the several patient's comorbidities, age and disease‐related disablement, a dedicated thorough respiratory, cardiac and performance status assessment was performed through specific tests (i.e. Karnofsky performance scale, spirometry, 6‐min walk test, nutritional risk screening score, Duke Activity Status Index) (Inoue et al., 2020; Wijeysundera et al., 2018, 2020) in order to define the actual patient's functional impairment guiding the medical decision (Table 1). The initial MDA (Figure 1), suggested an 8‐week prehabilitation program, including muscular and respiratory physical exercises with combined artificial (i.e., enteral + parenteral) nutrition (Table 1). Prehabilitation was mostly conducted at home with relatives' involvement and under the physiotherapist's guidance. The intermediate MDA registered general improvements in nutritional status (4 kg weight gain) and respiratory capacity (Table 1). Therefore, the patient was submitted to esophageal resection with a minimized surgical approach (i.e., transhiatal) to avoid chest opening and single‐lung ventilation. Transhiatal esophagectomy was performed with abdominal and lower‐mediastinal lymphadenectomy, cervical end‐to‐end esophagogastric anastomosis, feeding jejunostomy, and large right groin hernia repair. Operation was uneventful (307 min; blood loss of 210 mL), and ICU monitoring was not necessary after surgery. Postoperative recovery was complicated by a conservatively treated anastomotic leak and bilateral pleural effusion with pneumonia, requiring antibiotics and non‐invasive oxygen support. However, the most significant complication was a hemorrhagic shock caused by acute colonic bleeding originating from an occult cecum adenocarcinoma. To drive the urgent treatment strategy an additional MDA was performed and, given the functional reserve reduction, the patient was submitted to palliative ileocecal resection with minimization of both surgical approach (resection restricted to the source of bleeding, without radical lymphadenectomy) and anesthesia management (exclusive awake regional anesthesia) (Table 1). Emergency laparotomy was uneventful (119 min; blood loss of 120 mL), and ICU monitoring was not necessary after surgery. Afterward, postoperative recovery did not present further complications, and the patient was discharged at home after pneumonia resolution. After 90 days, the patient was alive and returned to normal daily activities with regular oral feeding along with 500 kcal nutritional supplementation, daily administered through the feeding jejunostomy.
Frailty–based multidimensional decisional approach. BSC, best supportive care; MDA, multidimensional assessment.
DISCUSSION
3
Increasing evidence has been supporting the application of major surgery to elderly population, including the most impactful operations, such as gastroesophageal resections (Laurent et al., 2022). It has been achieved that age does not represent an exclusive criterion limiting indications to surgery, while the choice should be made with regard to objective parameters, the need for surgery, and possible alternatives. The main role of the MDA (Figure 2) is to highlight the most relevant biological determinants in order to identify possible areas of optimization and to establish individual treatments tailored to patient functions. In patients undergoing major abdominal surgery, enhanced recovery after surgery (ERAS) guidelines recommend a careful preoperative cardiovascular and respiratory evaluation, to optimize the management of existing comorbidities and to plan the best intraoperative conduct and postoperative monitoring (Feldheiser et al., 2016). The development of multidisciplinary pathways to assess and improve patients' medical conditions should be especially encouraged in frail patients (Pang et al., 2021). Despite the low level of evidence, multimodal prehabilitation programs for patients receiving esophageal cancer resections appear to be associated with improvements in functional capacity (Minnella et al., 2018). In a recent prospective study by Halliday et al. (2021), esophageal cancer patients with a low baseline fitness were more likely to increase their functional capacity after prehabilitation, although these patients also presented a lower level of adherence to exercise programs. In our experience, effective prehabilitation programs can be successfully achieved through a close clinical monitoring only. The MDA implementation can be profitably extended to acute conditions and emergency surgery, demonstrating that operative stress minimization (including both surgical and anesthesiology components) aligns with treatment optimization and tailoring. We extensively explained the operative stress physiology and recovery after emergency treatments, showing management limitations or optimizations (Puccetti et al., 2023). In a recent meta‐analysis, Hajibandeh et al. (2021) reported the significantly high operative risk of octogenarians undergoing emergency general surgery, identifying risk characteristics correlating with mortality. As commented by Rubin et al. (2021), the type of anesthesia also plays a relevant role and contributes to the operative stress composition. Both general and neuraxial awake anesthesia present respectively advantages and contraindications in these specific groups of patients. Considering the severe impairment in respiratory function (i.e., recent pneumonia with the need for oxygen support), we decided to manage the emergency procedure only through a loco‐regional anesthesia, placing a thoracic epidural catheter. Also, a goal‐directed fluid management allowed the intraoperative maintenance of hemodynamic stability, although an adequate level of patient collaboration has to be ensured before treatment.
Stepwise procedure of Multidimensional Assessment (MDA).
The main limitation of this case report is the single‐patient analysis, which includes multiple elements of clinical peculiarities and potentially reduces the generalizability of these results. However, clinical aspects of perioperative management, functional assessment, and accurate patient‐tailored diagnostics could be effectively shared by other surgical units, who wondered about the best way to treat any delicate category of patients.
The present brief report suggests that octogenarians represent a frail category of patients, carrying a high risk for postoperative morbidity and early mortality. Palliative oncological surgery might include either major or urgent operations, as long as this decision is carefully considered and endorsed by a thorough multidimensional assessment. Accordingly, the choice for invasive approach demands the absence of possible therapeutic alternatives, while every potential consequence must be accurately and timely pondered within a comprehensive counseling to patients and relatives. In conclusion, either emergency or elective major surgery in elderly patients should not be excluded a priori, but these can be tailored/minimized according to the patient functional resources at a specific time. ERAS protocols and prehabilitation are strongly recommended in elderly since a high functional improvement can be attained in order to include the patient in invasive treatments. Therefore, specific and dedicated multidimensional assessment and medical protocols should be developed for elderly and frail patients.
FUNDING INFORMATION
No funding information provided.
CONFLICT OF INTEREST STATEMENT
No competing interests declared.
ETHICS STATEMENT
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of IRCCS San Raffaele Scientific Institute (Approval ID: 91/INT/2021, 30 June 2021).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Feldheiser, A. , Aziz, O. , Baldini, G. , Cox, B. P. B. W. , Fearon, K. C. H. , Feldman, L. S. , Gan, T. J. , Kennedy, R. H. , Ljungqvist, O. , Lobo, D. N. , Miller, T. , Radtke, F. F. , Ruiz Garces, T. , Schricker, T. , Scott, M. J. , Thacker, J. K. , Ytrebø, L. M. , & Carli, F. (2016). Enhanced recovery after surgery (ERAS) for gastrointestinal surgery, part 2: Consensus statement for anaesthesia practice. Acta Anaesthesiologica Scandinavica, 60, 289–334.26514824 10.1111/aas. · doi ↗ · pubmed ↗
- 2Fowler, A. J. , Abbott, T. E. F. , Prowle, J. , & Pearse, R. M. (2019). Age of patients undergoing surgery. The British Journal of Surgery, 106, 1012–1018.31115918 10.1002/bjs.11148 · doi ↗ · pubmed ↗
- 3Hajibandeh, S. , Hajibandeh, S. , Antoniou, G. A. , & Antoniou, S. A. (2021). Meta‐analysis of mortality risk in octogenarians undergoing emergency general surgery operations. Surgery, 169, 1407–1416.33413918 10.1016/j.surg.2020.11.027 · doi ↗ · pubmed ↗
- 4Halliday, L. J. , Doganay, E. , Wynter‐Blyth, V. , Osborn, H. , Buckley, J. , & Moorthy, K. (2021). Adherence to pre‐operative exercise and the response to prehabilitation in oesophageal cancer patients. Journal of Gastrointestinal Surgery, 25, 890–899.32314231 10.1007/s 11605-020-04561-2PMC 8007503 · doi ↗ · pubmed ↗
- 5Inoue, T. , Ito, S. , Kanda, M. , Niwa, Y. , Nagaya, M. , Nishida, Y. , Hasegawa, Y. , Koike, M. , & Kodera, Y. (2020). Preoperative six‐minute walk distance as a predictor of postoperative complication in patients with esophageal cancer. Diseases of the Esophagus, 33(2), doz 050.31111872 10.1093/dote/doz 050 · doi ↗ · pubmed ↗
- 6Laurent, A. , Marechal, R. , Farinella, E. , Bouazza, F. , Charaf, Y. , Gay, F. , van Laethem, J. L. , Gonsette, K. , & el Nakadi, I. (2022). Esophageal cancer: Outcome and potential benefit of esophagectomy in elderly patients. Thorac Cancer, 13, 2699–2710.36000335 10.1111/1759-7714.14596 PMC 9527164 · doi ↗ · pubmed ↗
- 7Lin, H. S. , Watts, J. N. , Peel, N. M. , & Hubbard, R. E. (2016). Frailty and post‐operative outcomes in older surgical patients: A systematic review. BMC Geriatrics, 16, 157.27580947 10.1186/s 12877-016-0329-8PMC 5007853 · doi ↗ · pubmed ↗
- 8Minnella, E. M. , Awasthi, R. , Loiselle, S. E. , Agnihotram, R. V. , Ferri, L. E. , & Carli, F. (2018). Effect of exercise and nutrition prehabilitation on functional capacity in esophagogastric cancer surgery: A randomized clinical trial. JAMA Surgery, 153, 1081–1089.30193337 10.1001/jamasurg.2018.1645 PMC 6583009 · doi ↗ · pubmed ↗