Evaluating Modern Implicit Bias Training in the Urology Workforce
John M Myrga, Shyam Patnaik, Bishoy Gayed

TL;DR
This study explores how often urology providers receive bias training and finds that it is often mandatory but not well-received.
Contribution
This is the first study to evaluate implicit bias training in the urology workforce.
Findings
Most urology providers reported exposure to bias training, often through online courses.
Only 8% of training was sponsored by urology departments, and 44% of providers felt it had a positive impact.
Topics like ageism and ableism were rarely covered in bias training.
Abstract
Introduction Implicit bias can lead to unintended influence in the treatment of other people and impact the care of patients. As such, there has been an increase in training to improve provider awareness of their own biases. There are many ways to address bias training within the medical community, but we currently do not have data on its use within urology. Our current study examined the frequency, modality, and intensity of bias training among urology providers. Methods We created a survey to evaluate exposure to bias education in members of the urologic community, with an optional exercise in implicit bias training. This survey was sent to a nationwide audience through the Society of Academic Urology (SAU) database and also shared on social media. All responses were anonymous. Institutional review board approval was obtained prior to study commencement (IRB STUDY23020038).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
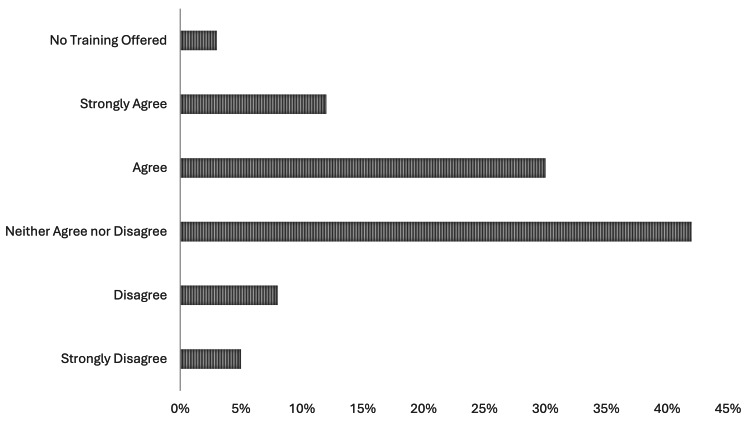 Figure 1
Figure 1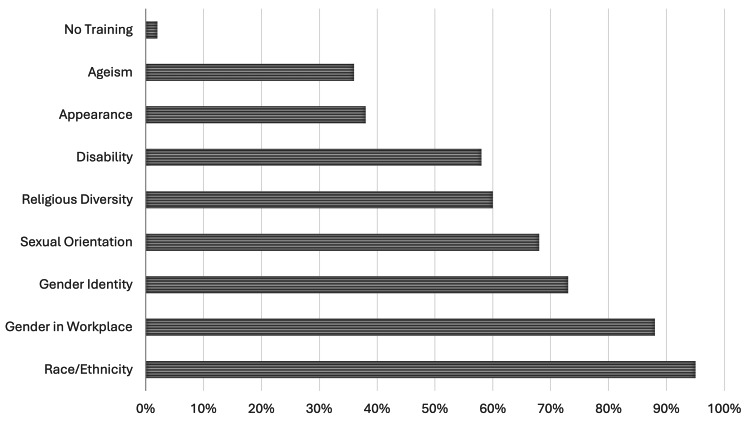 Figure 2
Figure 2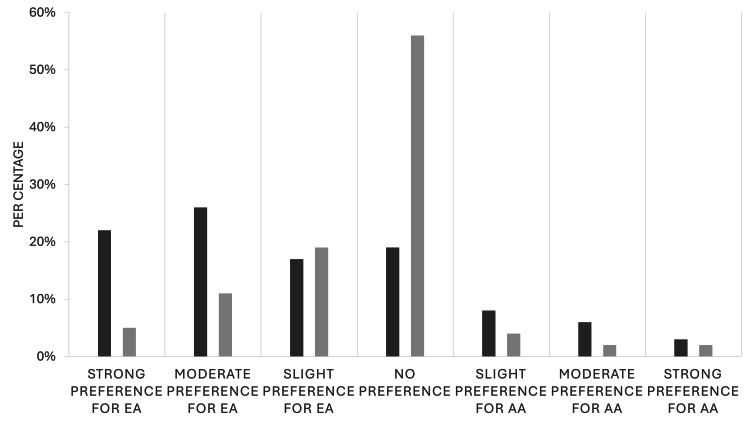 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiversity and Career in Medicine · Medical Education and Admissions · Innovations in Medical Education
Introduction
Implicit bias in medicine is a topic of interest due to the unconscious effect bias plays in providing patient care. The National Institutes of Health defines implicit bias as unintentional attitude, behavior, or actions that impact decisions or behaviors of one social group of people over another [1]. Since individuals are unaware of these biases, they can lead to unintended influence in the treatment of patients on a level not recognized by the provider [2-4]. Studies have shown that there are disparities in medical outcomes of Black patients compared to Caucasian patients, possibly related to perceived racial bias [5]. While race is the most cited area of unconscious bias, gender, religion, age, and ableism are also areas highly impacted by provider biases. Healthcare providers are not impervious to these subconscious biases and their effects on patient care [6].
Increased focus has been placed on understanding how to implement bias recognition and training in the urology community. It is not currently known if urology providers are receiving training in bias recognition and its impact on patient care. Furthermore, we do not know which modalities are being utilized and if providers find them effective. Given the known issues of provider burnout and "click fatigue," the commonly used modality of module-based training may not be an effective method [7]. Understanding the exposure of the urologic community to bias training and their experience may prove important to its effective implementation.
One way to promote knowledge of these subconscious influences is through the implicit association test (IAT). This test is a computerized assessment that measures how long a participant takes to associate pictures or words representing a social group (e.g., Black or Caucasian people) with characteristics (e.g., good, stubborn) [8]. The use of the standardized IAT has led to the identification of implicit racial bias in the treatment of patients of color [9]. While specific training in implicit bias has improved awareness in training programs such as emergency medicine and OB/GYN, there is limited data on the evaluation of implicit bias in urology [10].
We aimed to assess exposure to formal bias training among urologists, with a secondary goal of evaluating exposure to the IAT within the urologic workforce. This will help address the knowledge gap in the field. The purpose of our study is to raise awareness of implicit racial bias in urology and improve standardized training on identifying and managing implicit bias.
Materials and methods
We created a brief survey to evaluate exposure to bias training in members of the urologic community with an optional exercise in implicit bias. This survey has not previously been studied or validated. This survey was sent to a Canadian and United States audience, and all responses were anonymous. The University of Pittsburgh Institutional Review Board (IRB) deemed our study exempt from formal approval (IRB STUDY23020038).
Survey design
Our survey was created using Survey Monkey, allowing for anonymous responses that did not collect participants' personal or internet protocol (IP) information. Basic demographic information was obtained. The survey was intended to gauge participant exposure to bias training within their institution. Question formats included multiple choice, a drop-down menu, and free text fields. Patients were asked about their exposure to bias training within their institution, who provided that bias training, and if they felt the training to be effective. At the end of the survey, all participants were asked to complete the race IAT created by Project Implicit at Harvard University. Participation in this part of the study was optional. Participants were then asked to provide their final results from this exercise at the end of the study. The survey questions are included in the Appendices.
Survey distribution
We invited physicians, fellows, residents, advanced practice providers (APPs), nursing, and administrative staff within urology to complete the survey via various forms of social media with a sharable link. In addition, we sent the survey to all members subscribed to the Society for Academic Urology (SAU) email distribution service. This is made up of providers based in the United States and Canada. We also requested these members to recruit their fellow faculty, residents, and staff members to complete the study. There was no incentive for completion of the survey, and participation was voluntary. The survey was published and emailed via the SAU email server on June 19th, 2023, with a repeat email sent two weeks later. A link to the survey was also posted by the study creators on Twitter. We allowed for reposting and sharing of this link. The study was closed six weeks following the initial email response. Data was then abstracted from the Survey Monkey Collection site.
Data analysis
Data was downloaded from the Survey Monkey website and uploaded to an SPSS dataset (Aramonk, NY, Version 29, 2022). Descriptive data was then obtained and presented as appropriate. Some questions allowed for multiple responses, so data may not add to 100 percent. Graphs and figures were created using Microsoft Excel (2023 Edition).
Results
Of the 84 providers who responded to the survey, 77 (91%) were physician providers (e.g., attendings), five (5%) were resident physicians, and two (2%) were advanced practice providers (APPs). Additionally, 56 (67%) respondents reported that bias training is mandatory within their departments, while 63 (75%) indicated that the primary method of training is an online course or module. Only seven (8%) respondents noted that their bias training was sponsored by the urology department or division at their institution. Only 37 (44%) providers agreed the bias training they were provided had a positive impact (Figure 1).
Percentage of providers who agree that their current diversity training had a positive impact on their education.
The most common topics reviewed in respondents’ implicit bias training were race and gender in the workplace (Figure 2). Compared to other topics, ageism, and physical appearance were less commonly discussed.
Provider-reported content of their current diversity training.
We then examined the responses specific to the IAT. Forty-one (49%) providers had previously taken an IAT. Of the 84 providers, 55 (66%) chose to complete the racial IAT, and 42 (50%) participants elected to self-report the results of their IAT. Among those who completed the race IAT as part of the survey and chose to report their results, most showed little to no preference for European American over African American responses. The results of our study population are compared with reference values from a national, non-specific population that had taken the racial bias IAT (Figure 3).
Results of the IAT in our urology population compared to the general population who completed the race IAT.Dark grey: results from a national comparison population; light grey: results from our urology-specific populationEA: European ancestry; AA: African ancestry; IAT, implicit association test
Discussion
This study aimed to evaluate the exposure of the urologic workforce to bias training within their institution. We had a secondary aim of evaluating the exposure of participants to the racial IAT. Our results were primarily limited to academic faculty and noted that over two-thirds had required bias training within their department. Over 75% noted that this training was provided through modules, and only 37 (44%) indicated that the training was useful. About half of providers were familiar with an IAT and 42 (50%) participants elected to take an IAT as part of our study.
Bias training and the importance of diversity, equity, and inclusion continue to be a topic of interest to the medical community and the urologic community as a whole [6]. What is not clear is how to best engage and inform providers of how bias can impact patient care. IATs have been used to help providers describe and understand their own biases [6]. It is important to know that while useful, these tests are not clear markers of bias and have their own limitations [11,12]. Modules have also been widely used to introduce and teach providers about bias and diversity, but their efficacy remains questionable [13,14]. Our study confirms that this is the most common modality used to inform and engage providers regarding diversity. We note that only 44% of people who responded noted this training had a positive impact on their training. While our study is not large enough to examine this specific question, module-based learning appears to have low satisfaction with diversity training in the urologic community.
We also noted that while there was a wide variety of topics that were covered, many important topics were left out of standard diversity training. Urology is a specialty that has wide exposure to patients of different races, ethnicities, religious backgrounds, and gender identities. This further highlights the need for urology to have this exposure and training to provide the best care for our patients. Our results show that there is currently a gap in the training offered to providers as well as a high dissatisfaction with their implementation. Further steps are needed to address this knowledge gap and improve provider satisfaction in their education.
One method that has been implemented across many surgical fields is the concept of cultural complications grand rounds. This has been pioneered by the University of Maryland and The University of Michigan. This is an in-person or virtual discussion that is led by a faculty member with a pre-designed curriculum around multiple topics related to diversity and cultural components of medicine. Early studies have shown that this approach may have increased satisfaction for providers and trainees [15,16]. This allows for a discussion-based approach allowing providers of all levels to discuss these issues in a clinical setting with their peers. While this is only one option, it may help to address the lack of exposure and high dissatisfaction seen in current studies. These interventions are simple and impactful methods to increase awareness of diversity within the urology community and avoid the click fatigue often associated with module-based methods. We believe our study brings awareness to this issue and allows for targeted direction for future studies.
Our study comes with some limitations. First, we polled the academic urology community so our results are limited to members within that community. "Furthermore, our population was limited to English-speaking North American providers. Understanding the exposure of providers in community-based settings or those based outside of North America would provide important information that is missing in our study. In addition, almost 90% of our responses were attending faculty. While this is important as this is where the majority of patient-facing care is completed, understanding the exposure of allied providers, trainees, and nursing staff would be greatly informative. Our study is also limited by the nature of the questions as well. Since our goal was to obtain general information, our survey is non-standardized. Our methods of outreach also were targeted at physicians using social media and those within the academic community. We aimed to keep our study brief to increase participation but further studies should probe deeper into specific aspects of diversity training in the urologic community.
Conclusions
Our study shows that bias training within the urologic community is limited and its current implementation leads to low satisfaction among providers. Current methods, such as the IAT, are rarely used, and reliance on module-based learning may lead to low satisfaction. More engaging methods, such as the Cultural Complications Grand Rounds model, may be more effective and engaging for urology providers. Future studies should explore the use of these interventions and gain a broader understanding of bias training within the urologic community.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities J Gen Intern Med Chapman EN Kaatz A Carnes M 150415102820132357624310.1007/s 11606-013-2441-1PMC 3797360 · doi ↗ · pubmed ↗
- 2Instilling new habits: addressing implicit bias in healthcare professionals Adv Health Sci Educ Theory Pract Byrne A Tanesini A 125512622020152577174210.1007/s 10459-015-9600-6 · doi ↗ · pubmed ↗
- 3Tackling implicit bias in health care N Engl J Med Sabin JA 10510738720223580198910.1056/NEJ Mp 2201180 PMC 10332478 · doi ↗ · pubmed ↗
- 4Implicit bias in healthcare professionals: a systematic review BMC Med Ethics Fitz Gerald C Hurst S 191820172824959610.1186/s 12910-017-0179-8PMC 5333436 · doi ↗ · pubmed ↗
- 5Examining the presence, consequences, and reduction of implicit bias in health care: a narrative review Group Process Intergroup Relat Zestcott CA Blair IV Stone J 5285421920162754710510.1177/1368430216642029 PMC 4990077 · doi ↗ · pubmed ↗
- 6Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review Am J Public Health Hall WJ Chapman MV Lee KM 076105201510.2105/AJPH.2015.302903 PMC 463827526469668 · doi ↗ · pubmed ↗
- 7Rethinking EHR interfaces to reduce click fatigue and physician burnout CMAJ Collier R 05190201810.1503/cmaj.109-5644 PMC 610211330127043 · doi ↗ · pubmed ↗
- 8When best intentions aren't enough: helping medical students develop strategies for managing bias about patients J Gen Intern Med Teal CR Shada RE Gill AC Thompson BM FrugéE Villarreal GB Haidet P 0825 Suppl 2201010.1007/s 11606-009-1243-y PMC 284711920352504 · doi ↗ · pubmed ↗