Endoscopic retrograde cholangiopancreatography combined with peroral choledochoscope for the treatment of complete bile duct rupture
Qingsong Wu, Ming Zhang, Donghai Zhuang, Baochang Shi, Jinglong Guo, Yannan Yin, Kai Zhang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
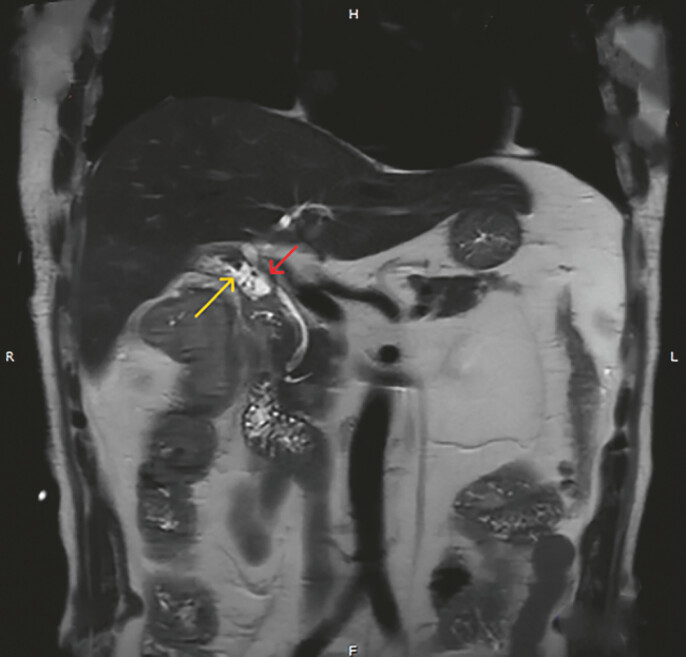 Fig. 1
Fig. 1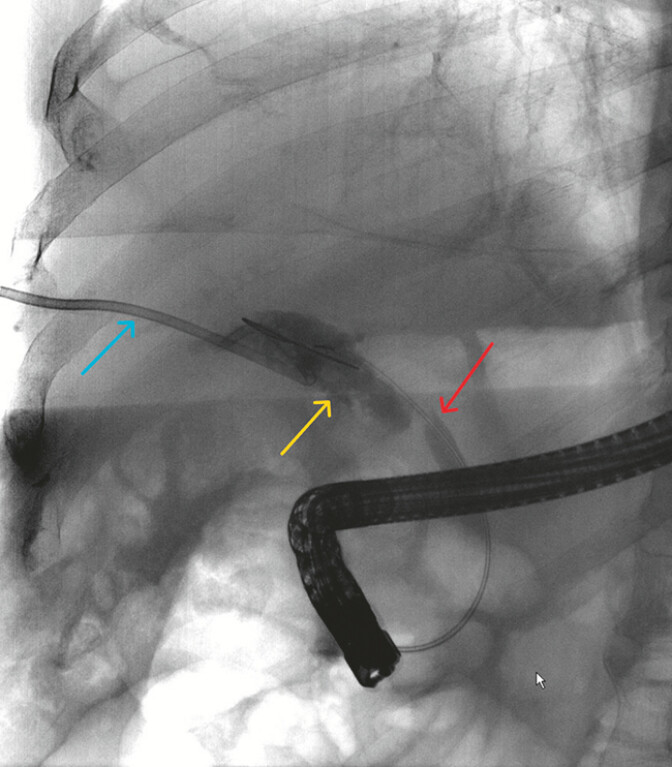 Fig. 2
Fig. 2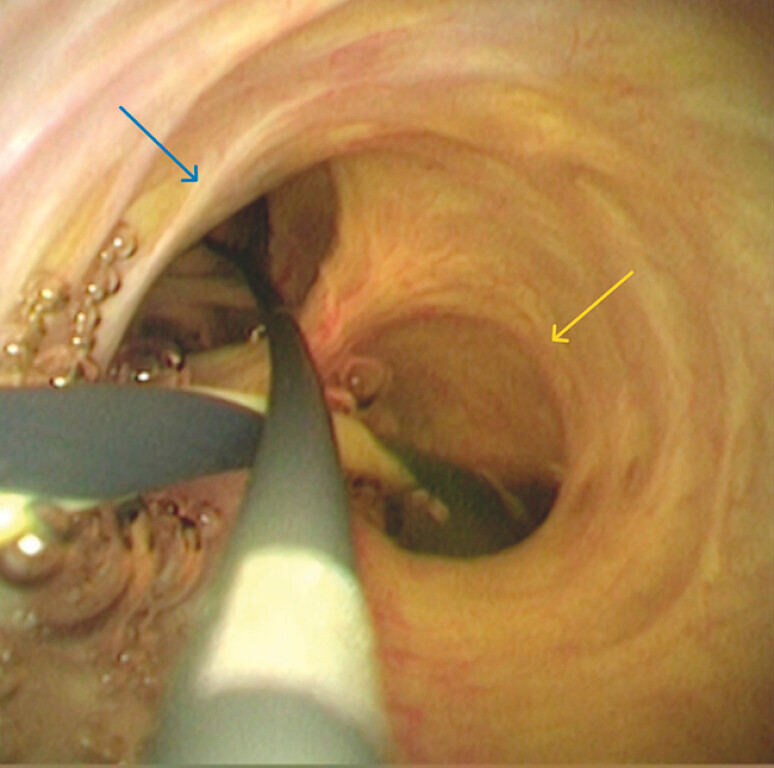 Fig. 3
Fig. 3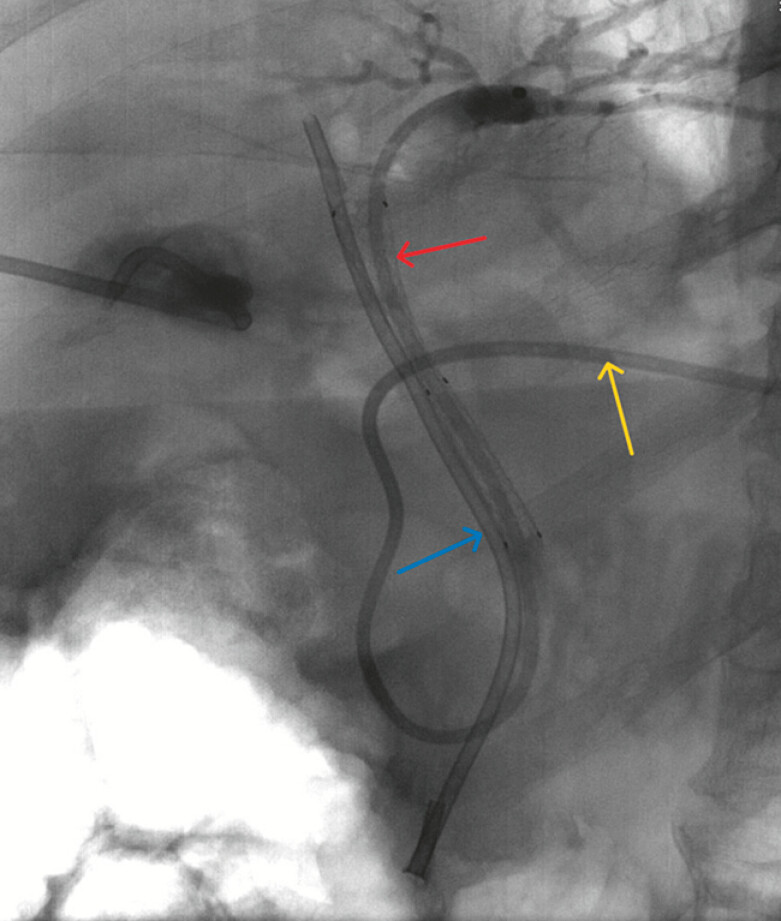 Fig. 4
Fig. 4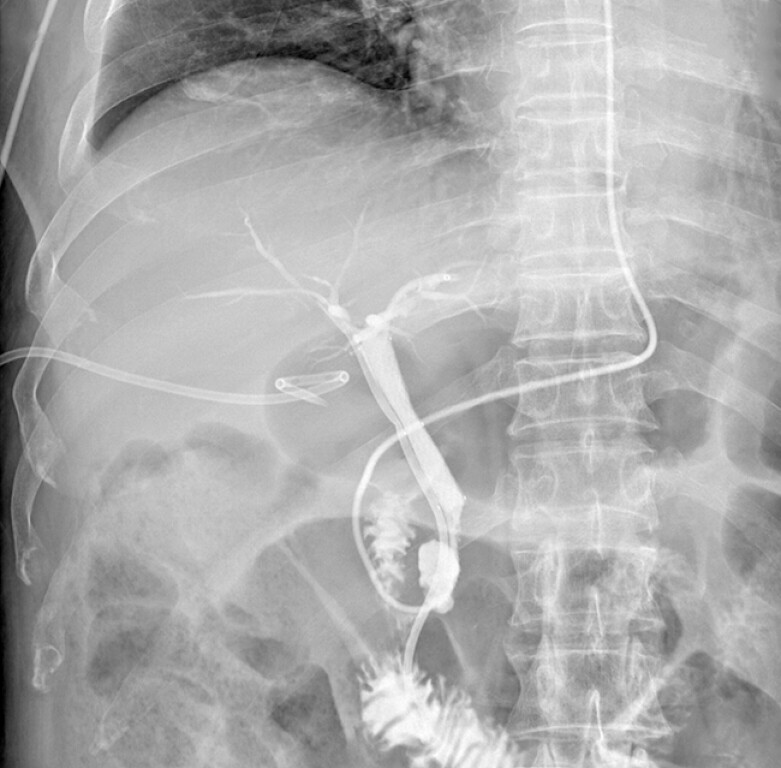 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Pancreatic and Hepatic Oncology Research
Iatrogenic bile duct injury is one of the serious complications of laparoscopic cholecystectomy 1 2 . Here, we present a patient with massive bile leakage due to complete bile duct rupture after the procedure. A 69-year-old man was admitted to the hospital due to skin and sclera jaundice with a fever for half a month. He underwent laparoscopic cholecystectomy in another hospital 20 days ago. The abdominal drainage tube drained about 800 ml of bile daily. Magnetic resonance cholangiopancreatography (MRCP) showed localized ascites and discontinuity of the common bile duct (CBD) ( Fig. 1 ).
Magnetic resonance cholangiopancreatography showed localized ascites (yellow arrow) and discontinuity of the common bile duct (CBD) (red arrow).
Endoscopic retrograde cholangiopancreatography (ERCP) showed contrast agent extravasation into the peritoneal cavity and rupture of the upper CBD ( Fig. 2 ). We then explored the CBD through the peroral choledochoscope and found that the upper part of the CBD was completely ruptured. The abdominal drainage tube and Hem-o-lok clip were seen through the peroral choledochoscope. After repeated attempts, combined with X-ray localization, we successfully inserted guidewires into the left and right hepatic ducts ( Video 1 ). The common hepatic duct, left hepatic duct, and right hepatic duct were identified through the peroral choledochoscope ( Fig. 3 ). A plastic stent (8.5 Fr, 12 cm) was placed in the right hepatic duct, followed by a fully covered metal stent (10 mm, 5 cm) in the CBD. Finally, a nasobiliary duct was placed in the left hepatic duct through the metal stent lumen ( Fig. 4 ). Bile in abdominal drainage decreased rapidly to disappear. On the 10 ^th^ day after the intervention, nasal cholangiography showed no obvious bile leakage ( Fig. 5 ). On the 24 ^th^ day, it showed the stent was unobstructed without stenosis.
Endoscopic retrograde cholangiopancreatography showed contrast agent extravasation into the peritoneal cavity (yellow arrow) and rupture of the upper CBD (red arrow). The blue arrow was the abdominal puncture drainage tube.
The common hepatic duct, left hepatic duct (yellow arrow), and right hepatic duct (blue arrow) were identified under peroral choledochoscope.
A plastic stent (blue arrow) was placed in the right hepatic duct, followed by a fully covered metal stent (red arrow) in the CBD. A nasobiliary duct (yellow arrow) was placed in the left hepatic duct through the metal stent lumen.
On the 10 th day after the intervention, nasal cholangiography showed no obvious bile leakage.
Endoscopic retrograde cholangiopancreatography combined with peroral choledochoscope for the treatment of complete bile duct rupture.Video 1
Cases with a partial defect or rupture of the bile duct after laparoscopic cholecystectomy usually require secondary surgery 3 . ERCP combined with peroral choledochoscope to bridge the ruptured bile duct has created a new, alternative minimally invasive treatment approach. However, long-term effects such as biliary stenosis require longer follow-up and more cases to provide experience.
Endoscopy_UCTN_Code_CPL_1AM_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brunt LM Deziel DJ Telem DA Safe cholecystectomy multi-society practice guideline and state-of-the-art consensus conference on prevention of bile duct injury during cholecystectomy Surg Endosc 2020342827285510.1007/s 00464-020-07568-732399938 · doi ↗ · pubmed ↗
- 2Pesce A Palmucci S La Greca G Iatrogenic bile duct injury: impact and management challenges Clin Exp Gastroenterol 20191212112810.2147/ceg.S 16949230881079 PMC 6408920 · doi ↗ · pubmed ↗
- 3deʼAngelis N Catena F Memeo R 2020 WSES guidelines for the detection and management of bile duct injury during cholecystectomy World J Emerg Surg 2021163010.1186/s 13017-021-00369-w 34112197 PMC 8190978 · doi ↗ · pubmed ↗